Covid-19

Self Assessment
- Define Nosocomial Pneumonia and list the risk factors associated with it.
- Name some of the organisms that cause Nosocomial Pneumonia.
- What are the clinical criteria that aid the diagnosis of Nosocomial Pneumonia?
- What are the principles of management of Nosocomial Pneumonia?
- A 70 year old man is admitted to a hospital , having been found collapsed at home. He has been coughing for the last few days prior to his admission. CXR reveals Right lower lobe consolidation. List the tests that you would order? Discuss likely pathogens and appropriate antibiotic choice.
(The answers to the self assessment questions are found in the text of the article.)
Nosocomial pneumonia is the second most frequent hospital acquired infection and the most common acquired infection in the intensive care unit. (ICU) The incidence is age dependent. There is no race or sex predilection. Death from nosocomial pneumonia in ventilated patients reaches 30-50% with an estimated attributable mortality of 10- 50%.
DEFINITIONS
Nosocomial Pneumonia is traditionally defined as pneumonia occurring in patients admitted to hospital for at least 48 hours. Pneumonia per se is the appearance of new lung infiltrates plus evidence that the infiltrate is of infectious origin such as fever, leucocytosis or purulent sputum. The term ventilator associated pneumonia (VAP) is often used synonymously but in fact specifically refers to pneumonia occurring in patients more than 48 hours after endotracheal intubation and initiation of mechanical ventilation.
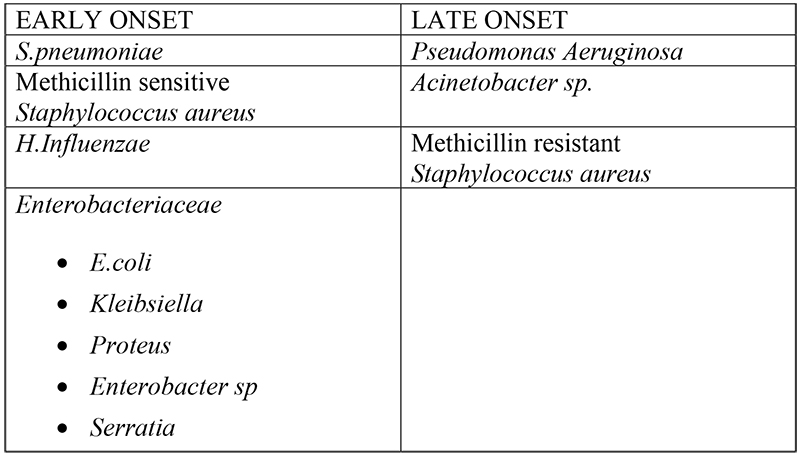
Dividing patients into two groups based on time of onset i.e. early and late is useful in predicting causative pathogens and prescribing antibiotics appropriately for nosocomial pneumonia. Early onset nosocomial pneumonia commonly results from endogenous community-acquired pathogens such as Staphylococcus aureus, Streptococcus pneumoniae and Haemophilus influenzae. Conversely late onset pneumonia follows infection with drug resistant pathogens such as Pseudomonas sp. and methicillin resistant Staphylococcus aureus (MRSA). The risk of drug resistant microorganisms in late onset pneumonia is further increased if patients had been on broad spectrum antibiotic treatment or had been invasively ventilated for more than seven days prior to the onset of the pneumonia. The definitions for early and late onset VAP have not been standardised. If time of admission to hospital is chosen as the starting point, then the American Thoracic Society (ATS) guidelines suggest using 5 days as a cut off for differentiating early and late onset VAP.
RISK FACTORS
The risk factors can be grouped into five general categories:
- host factors such as extremes of age, immunosupression.
- factors that enhance colonisation of the oropharynx and/or stomach by microorganisms e.g. antibiotics, admission to ICU, underlying chronic lung disease or coma.
- conditions favouring aspiration or reflux e.g. intubation, insertion of nasogastric tube or supine position.
- conditions requiring prolonged use of mechanical ventilatory support with potential exposure to contaminated respiratory equipment and/or contact with colonised and contaminated hands of nursing and medical staff.
- factors that impede adequate pulmonary toilet e.g. surgery to head and neck or immobilisation due to trauma.
NATURAL HISTORY
The natural history of nosocomial pneumonia and particularly VAP is not well understood, confounding the assessment of response to therapy. The course of pneumonia depends on not only the pathogen involved but also the choice of antibiotics and the host’s ability to respond. Several studies have shown a consistent improvement in patient survival if appropriate antibiotics are used from the outset of the illness and it is therefore important to choose these with care. It is difficult to determine when a patient is not responding and conversely to decide when it is possible to shorten the duration of therapy in responders to treatment.
Improvement occurs with resolution of fever, followed by improved oxygenation and leukocyte count and, finally, decreased bacterial colonization of the lower respiratory tract. Studies have shown respiratory bacterial eradication was completely successful when the pneumonia was due to the flora associated with early-onset VAP, such as Haemophilus influenzae and Streptococcus pneumoniae, partially successful (50%) with Gram-negative flora, such as the Enterobacteriaceae, and not successful with Pseudomonas species (persisted in cultures). In addition, secondary colonization occurred during the second week of therapy; this was generally with resistant organisms like P. aeruginosa, Enterobacteriaceae, and S. aureus.
Furthermore, long courses of antibiotics are also undesirable. To facilitate discontinuation, it is necessary to define resolution of Gram-negative pneumonia by using clinical, rather than bacteriologic, parameters. Recent studies looked at the resolution of VAP, diagnosed using clinical criteria, in an attempt to find indices predicting survival, including the Clinical Pulmonary Infection Score (CPIS). The authors found that in survivors of VAP, oxygenation was the first to improve (7.8 days), followed by fever and leukocytosis, with progressive reduction in the CPIS score. In nonsurvivors, the CPIS score remained high and hypoxemia never resolved. A falling CPIS may, therefore, allow for shorter course therapy. Indeed, a low or improving CPIS after 3 days of treatment has been used to identify responders that could receive short course (3 days) of antibiotic therapy.
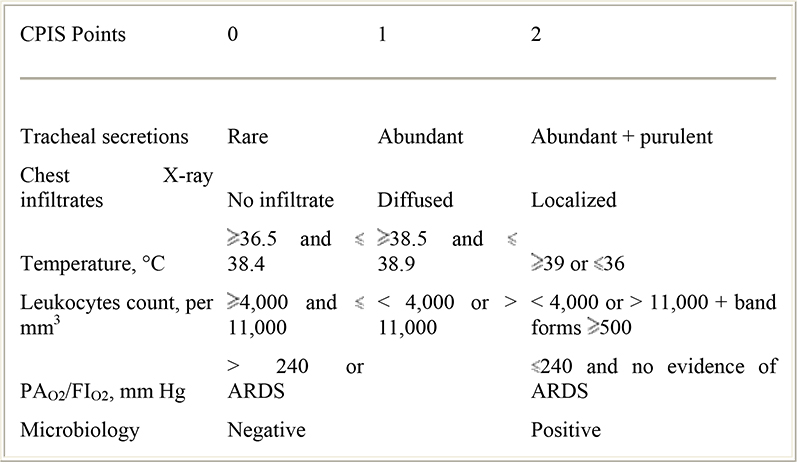
TABLE 1. The modified clinical pulmonary infection score (Fartoukh et al., Am. J. Resp. and Crit. Care Med.(2003) Vol 168. pp. 173-179.
DIAGNOSTIC CRITERIA
Diagnosis of nosocomial pneumonia is difficult, especially differentiating infection from colonisation, but a combination of criteria can be used. The centre for control of communicable diseases (CDC) criteria is :-
Three or more positive of the following parameters
- Rectal temperature > 38 or 35.5 C
- Leucocytosis 10x 109/L, left shift or leucopenia 3.109/L
- Ten leucocytes per HPF in gram stain of endotracheal aspirates.
- Positive culture from endotracheal aspirates
- New, progressive or persistent radiographic infiltrates.
However clinical observations, laboratory results and chest radiographs are of limited value in diagnosing nosocomial pneumonia. Considerable efforts have been made to establish independent microbiological criteria. A helpful initial endeavour is Gram staining of respiratory secretions, which can provide information within 15 minute. Samples can be obtained by different methods, including protected specimen techniques, bronchoalveolar lavage, and tracheal aspirates. Suitable samples have less than 1% of squamous epithelial cells and more than 10% of neutrophils.
A negative tracheobronchial aspirate culture has a high negative predictive value, so that a negative culture in a patient not receiving antimicrobial treatment essentially excludes VAP. Quantitative cultures of protected specimen brush (PSB) and bronchoalveolar lavage (BAL) specimens obtained through a bronchoscope have also been used to diagnose VAP. In nonintubated patients, PSB and BAL techniques have shown a high specificity for the diagnosis of NP. In mechanically ventilated patients with suspected VAP, the following observations have been made:
- PSB and BAL are of comparable diagnostic value;
- tracheobronchial aspirates have comparable results with PSB and BAL, but have lower specificity;
- all methods have false-negative and false-positive rates ranging from 10% to 30%.
Accurate diagnosis can be made only by open lung biopsy, evidence of cavitation in the absence of malignancy or isolation of the same pathogen with the same antibiogram from blood and respiratory secretions. However the invasive nature of these techniques limits their usefulness.
CAUSATIVE ORGANISMS
PREVENTIVE MEASURES
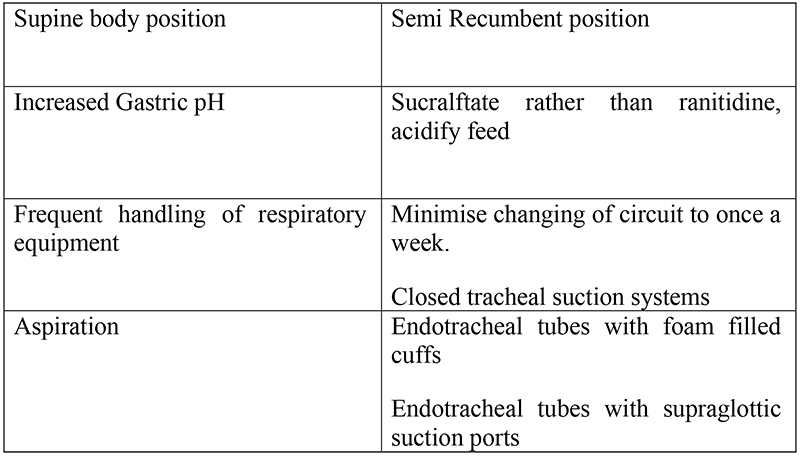
Several risk factors for NP can be minimised by simple and inexpensive preventive strategies. However these measures may not be easy to apply. Furthermore there is insufficient evidence to support the use of even the most logical of these, hand washing for instance.
Selective Decontamination of Digestive tract (SDD) is a strategy to prevent bacterial colonisation in mechanically ventilated patients. It is aimed at preventing oropharyngeal and gastric colonisation with aerobic Gram negative bacilli and Candida without altering the anaerobic flora. SDD regimes vary but most use a combination of locally administered polymixin or aminoglycoside i.e to be applied to oropharynx as a paste and given orally and an intravenous antibiotic such as cefotaxime. A recent meta-analysis has demonstrated a decrease in rates of nosocomial pneumonia with the use of SDD, however, its use in the U.K. still remains low due to concerns over the emergence of more antibiotic resistance.
Strategies that have been recommended are given in the table below.

MANAGEMENT STRATEGIES
- Initial antimicrobial treatment should always be empiric.
- Empirical antimicrobial treatment should be guided by 3 criteria: severity, time of onset, and specific risk factors.
- Selection of antimicrobial agents must be adapted to the local pattern of microbial resistance and epidemiology.
- The diagnostic workup may offer additional data that should be interpreted in the context of the patient’s condition.
- In patients with early onset VAP without risk factors for resistant pathogens, antimicrobial therapy should cover community-endogenous pathogens and nonresistant Gram-negative Enterobacteriaceae.
- In patients with late-onset VAP without risk factors, empiric antimicrobial therapy should cover potentially resistant microorganisms, including Pseudomonas aeruginosa, Acinetobacter species, and MRSA.
- In patients with early- or late-onset VAP with risk factors, empiric therapy should be the same as in late-onset without risk factors, except when Legionella species are considered.
The chance of multiple drug resistant pathogens in patients with VAP is greater in those with long hospital and ICU stays, prior antibiotic therapy, multiple comorbidities, and prolonged MV. In these patients, it is mandatory to know the local microbiological pattern and the patterns of resistance to assure adequate initial treatment.
In most studies, the most common reason for treatment failure was inadequate initial empiric antibiotic coverage, mandating initial broad-spectrum antibiotic coverage.
According to the ATS guidelines, the antibiotics suggested for the treatment of patients with severe early-onset NP should be :-
- a second-generation/third-generation cephalosporin or/
- a combined β-lactam/β-lactamase inhibitor or/
- a fluoroquinolone or/
- clindamycin plus aztreonam.
In patients with severe late-onset NP, the recommended treatment includes:-
- an aminoglycoside or/
- ciprofloxacin
plus one of the following:
- imipenem
- an anti-pseudomonal broad-spectrum penicillin
- an anti-pseudomonal third generation cephalosporin
- aztreonam.
Meropenem, piperacillin/tazobactam, or cefepime might also be administered as antipseudomonal antibiotics. A glycopeptide, such as vancomycin, should be added if MRSA is strongly suspected; linezolid or quinupristin/dalfopristin are alternatives (with evidence supporting the use of linezolid early in MRSA pneumonia in preference to vancomycin.)
Current recommendations are to start with broad-spectrum empiric antibiotics, then switch to narrow-spectrum specific therapy as guided by microbiological results. This deescalating approach is likely to ensure adequate upfront coverage, yet minimize the risk of resistance and adverse drug reactions over the treatment period. Thus, each ICU should design specific empiric treatment protocols that are likely to be effective according to local microbiology and resistance patterns and which require reevaluation after 48 to 72 hours.
Duration of Treatment
The standard duration of antibiotic therapy is 2 weeks according to clinical trials and guidelines. However, a recent study found that in patients receiving appropriate initial antibiotics, comparable results were found with 8 or 15 days of therapy.The duration of antibiotic therapy is individualized based on the clinical response and the causative pathogen. Consensus conferences suggest that patients infected with sensitive organisms may be treated for 7 to 10 days. Patients with multiresistant pathogens may require 14 to 21 days of treatment to prevent treatment failure or relapse. It has also been suggested, based on little data, that those patients with multilobar,necrotizing, or cavitary pneumonia receive extended (2–3 weeks) treatment. Minimal data exist to indicate if therapy can be discontinued at a set time. Physician education about appropriate antibiotic use may minimize the risks of antibiotic resistance. Also, scheduled changes of antibiotic regimens or routine microbiological surveillance-guided changes in antibiotic policy may reduce the emergence of resistant strains. Changes in antibiotic regimens may involve antibiotic cycling, which is the changing of usual antibiotic regimens from time to time or the use of different regimens in consecutive patients. Such heterogeneous antibiotic use may improve selective pressure and the likelihood of resistance.
CONCLUSIONS
Nosocomial pneumonia and especially VAP are the most frequent infectious complications in the ICU, and they significantly contribute to morbidity and mortality. VAP is an important determinant of ICU and hospital lengths of stay and healthcare costs. Several simple preventive measures and timely initiation of appropriate antibiotics ensure better outcomes in patients with VAP
Further Reading
- Chastre J and Fagon J. State of the Art : Ventilator Associated Pneumionia. Am J Respir Crit Care Med Vol 165 pp867-903, 2002
- Inweregbu K, Dave J and Pitard A : Nosocomial Infections. BJA CEPD vol 5;1; pp 14-17, 2005-08-27
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/