General Topics

Self Assessment
Complete these questions before reading the tutorial.
- What are the indications for inserting a double lumen tube?
- Describe insertion and checking position of a right-sided double lumen tube.
- Describe changes in ventilation & perfusion in an anaesthetised compared with an awake patient.
- A patient desaturates to 85% during one-lung anaesthesia for a lobectomy. Describe your management.
The answers can be found in the folowing text and text boxes.
One lung ventilation (OLV) is the term used in thoracic anaesthesia to describe the ability to ventilate one of a patient’s lungs, allowing the other one to collapse. This tutorial will describe indications for OLV, techniques used to achieve OLV, the physiological changes associated with OLV and ways that oxygenation can be improved during OLV.
Indications for OLV
There are 3 indications for OLV:
Improving surgical access. It is much easier for a surgeon to carry out lung surgery, or oesophageal surgery, if a lung is collapsed. Adequate surgical access can be achieved for most lung resections and oesophago-gastrectomies without collapsing a lung simply by ventilating the patient with smaller tidal volumes and the surgeon using a retractor. However, if the surgeon is not used to operating with the lung inflated, or if the tumour is technically difficult to resect, OLV will be required. It is important to discuss with the surgeon any difficulties or specific requirements that he anticipates, and to be aware exactly what he intends to do intraoperatively, as both surgeon and anaesthetist are influencing the organ that is oxygenating the body. Lack of communication can be disastrous.
Some surgery definitely needs OLV. Thoracoscopic surgery is impossible without collapsing a lung. A thoracoscopic procedure involves insufflating one side of the chest with carbon dioxide and introducing a camera and instruments through ports in the chest wall, similar to a laparoscopy in the abdomen. This technique is known as video-assisted thoracoscopic surgery (VATS). It can be used to carry out procedures such as stapling of bullae, pleurodesis, lung biopsy, thoracic sympathectomy, inspection of lesions to decide operability, and even lung resection.
Lung protection. OLV is indicated to protect the other lung from becoming contaminated by blood or pus in the diseased lung during surgery. An anaesthetised patient will lose the ability to cough and therefore the ability to prevent infected material/blood entering the normal lung.
Intensive Care ventilation. If a patient has a single lung disease, it may be desirable to ventilate the lungs independently using 2 ventilators so that the normal lung is not subjected to high pressure required to ventilate an abnormal lung. An example of this is after a single lung transplant.
Techniques for OLV
There are 3 devices that can be inserted to achieve one lung ventilation: a double lumen tube, a bronchial blocker, or a single lumen tube inserted beyond the carina.
Double lumen tubes are tubes (figure1) with one lumen opening just above the carina and the other inserted into a main bronchus.
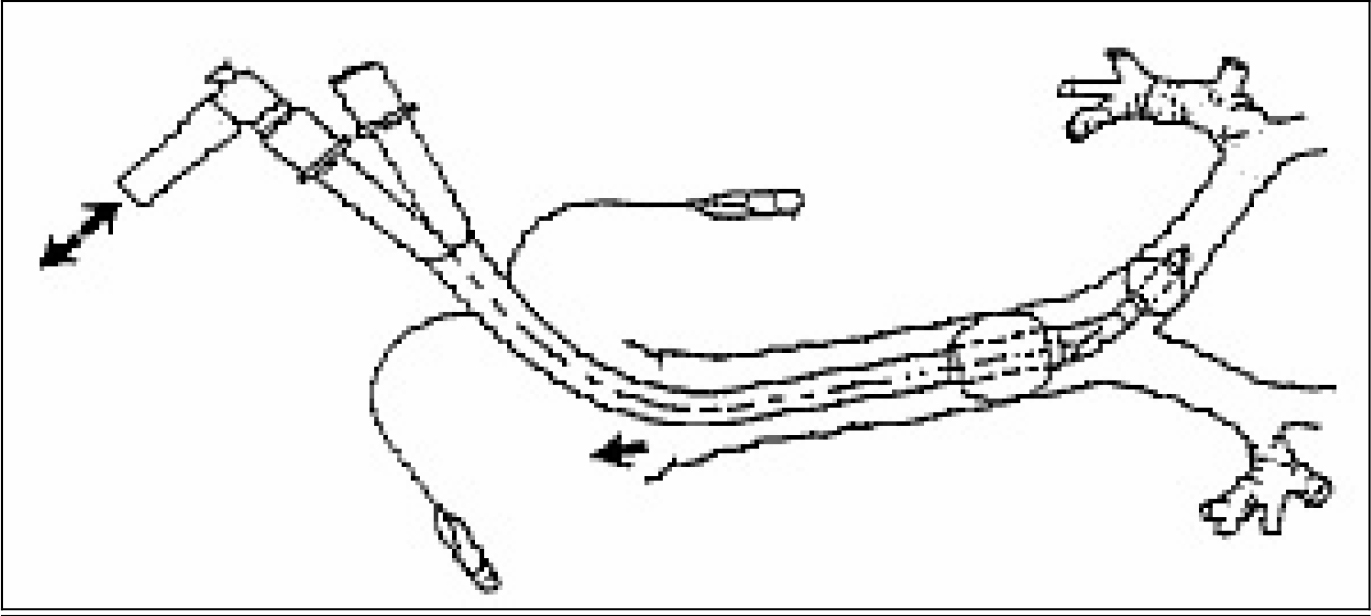
Figure 1: left sided double lumen tube
By clamping one lumen, this occludes ventilation to the lung on that side. If one lumen is opened to the atmosphere, the lung can deflate and ventilation continued through the other lumen. Tubes come in sizes 26 to 41 French gauge – 37-39 is the usual size for a female and 39-41 for a male.
There are right and left sided tubes. A left-sided tube has the endobronchial part down the left main bronchus; a right-sided tube down the right main bronchus.
Either tube can be used to ventilate either lung depending on which lumen is clamped, however a left-sided tube is usually used as it is easier to position. This is due to the anatomy of the right main bronchus. The right upper lobe comes off the right main bronchus at a variable distance from the carina in different people. It may also be anterior, lateral or posterior as you look down the bronchus. A right-sided DLT has a small hole towards the end of the endobronchial part called a Murphy eye. This has to be aligned with the entrance to the right upper lobe, or the lobe will not be ventilated. Of the currently available DLTs, the Rusch tube has a larger and more elongated Murphy eye compared to the Mallinkrodt (fig2), allowing for more variability in anatomy. Changing tube size may also compensate for variable anatomy.

Figure 2: Murphy eyes of Mallinkrodt & Rusch tubes
A left sided tube can be used for most operations. In surgery involving the left main bronchus such as a pneumonectomy with tumour involvement very near the carina, it may be preferable to use a right-sided tube, but it is perfectly possible to use a left sided tube and just withdraw it when the surgeon is about to staple the bronchus or clamp it ready to suture.
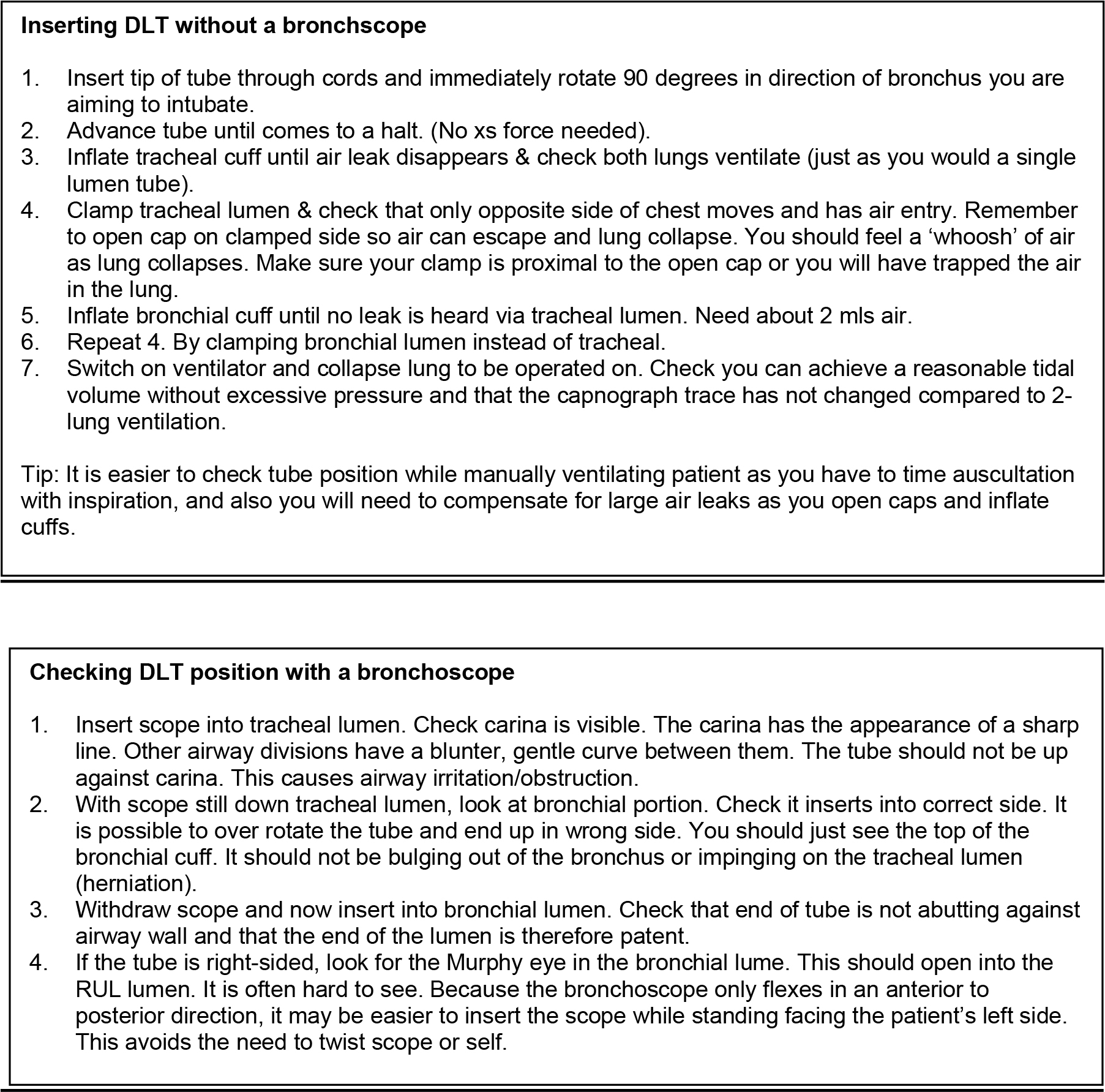
To insert a double lumen tube (DLT) the tip of the tube is inserted just through the vocal cords and then immediately rotated 90 degrees in the direction of the bronchus you are aiming to intubate. The tubes are bulky and can be awkward to place, particularly in dentulous patients. One lumen is clamped at a time and the chest auscultated to make sure that each lung can be collapsed. If possible, the tube position should be checked with a bronchoscope. It is possible that the tube is achieving the desired clinical effect, but with a tiny movement becomes malpositioned. The tubes, usually made of plastic, become softer as they warm to the patient’s body temperature, and, combined with the fact that the patient may need to be moved to a lateral position and the surgeon may manipulate the mediastinal structures during surgery, the tube often becomes dislodged. Using the bronchoscope habitually will make it easier to recognise the anatomy and therefore fix problems when they arise. All that is necessary is a check to see that the tracheal lumen is above the carina, the bronchial lumen is in the correct bronchus and that it’s cuff is not blocking the other (tracheal) lumen by herniating over it, and that the bronchial lumen is clear and not abutting an airway wall. If right sided, the right upper lobe entrance needs to be seen.
A bronchial blocker (fig 3) is a device that is inserted into a conventially placed single lumen tube. It is useful when it is not possible to place a DLT or in situations where the patient has already been intubated with a single lumen tube. It has the appearance of a hollow bougie with a cuff. There is a type that has a steerable tip (Cohen by Cook) as well as the basic type that cannot be steered (Arndt). The blocker has a guidewire in its lumen, the end of which can be hooked over a bronchoscope so the blocker can be inserted under direct vision into the lung that is to be collapsed. This guidewire needs to be removed before air can be withdrawn from the blocker and hence collapse the lung. A disadvantage is that once the guidewire on the device has been withdrawn, it cannot be reinserted so the blocker cannot be reused or repositioned in the patient. Also, because a bronchoscope needs to be used both to guide the blocker into place and to verify its position, this means that if there is blood or secretions in the airway, this technique may not be possible.
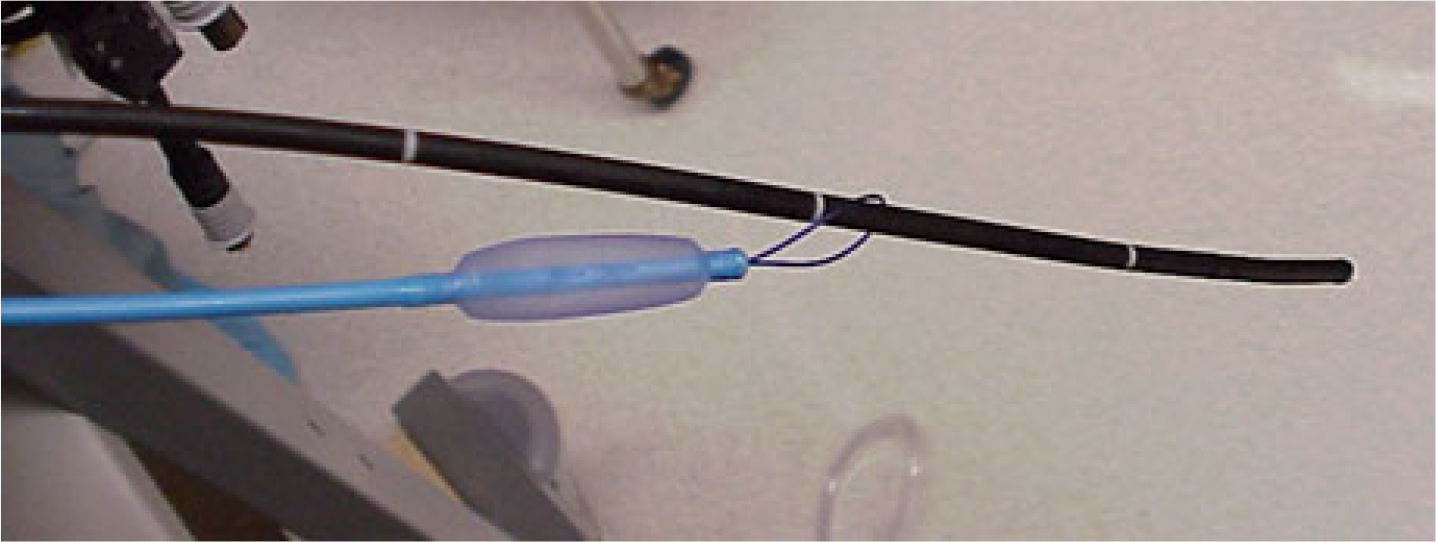
Figure 3: Bronchial blocker
The third way of achieving OLV is by use of a single lumen tube intentionally inserted ‘too far’ into a bronchus. This may be a good option in an emergency such as a leftsided chest stabbing if you fail to insert a DLT, and blood in the airway makes it impossible to use a bronchoscope.
Physiology of OLV
As a simple view of lung physiology, when a patient is awake, the dependent part of a lung (regardless of the patient’s position) has a greater blood supply than the nondependant part due to gravity. The dependent part is also preferentially ventilated compared with the non-dependent lung due to it being slightly more compressed than the non-dependant lung and therefore having a greater compliance once the atelectatic airways at the base have been opened. This can be thought of like blowing up a balloon. Initially, the pressure required is large to start blowing up the balloon (atelectatic bits), it then becomes easier and a small change in pressure will give a big change in volume(dependent lung). As the balloon gets bigger and the material gets more stretched, a larger pressure is needed to give a change in volume( the non-dependent lung). Ventilation (V) and perfusion (Q) are relatively well matched and shunt (lung that is perfused but not ventilated) is only 1-2% in a healthy person.
Simply anaesthetising a patient alters lung physiology before you even consider the effect of collapsing a lung. The functional residual capacity (FRC) decreases as the diaphragm and chest muscles are paralysed. Mediastinal weight becomes unsupported by the surrounding structures becoming relaxed. Figure 4 shows the compliance of the lungs in both the awake and the anaesthetised patient.
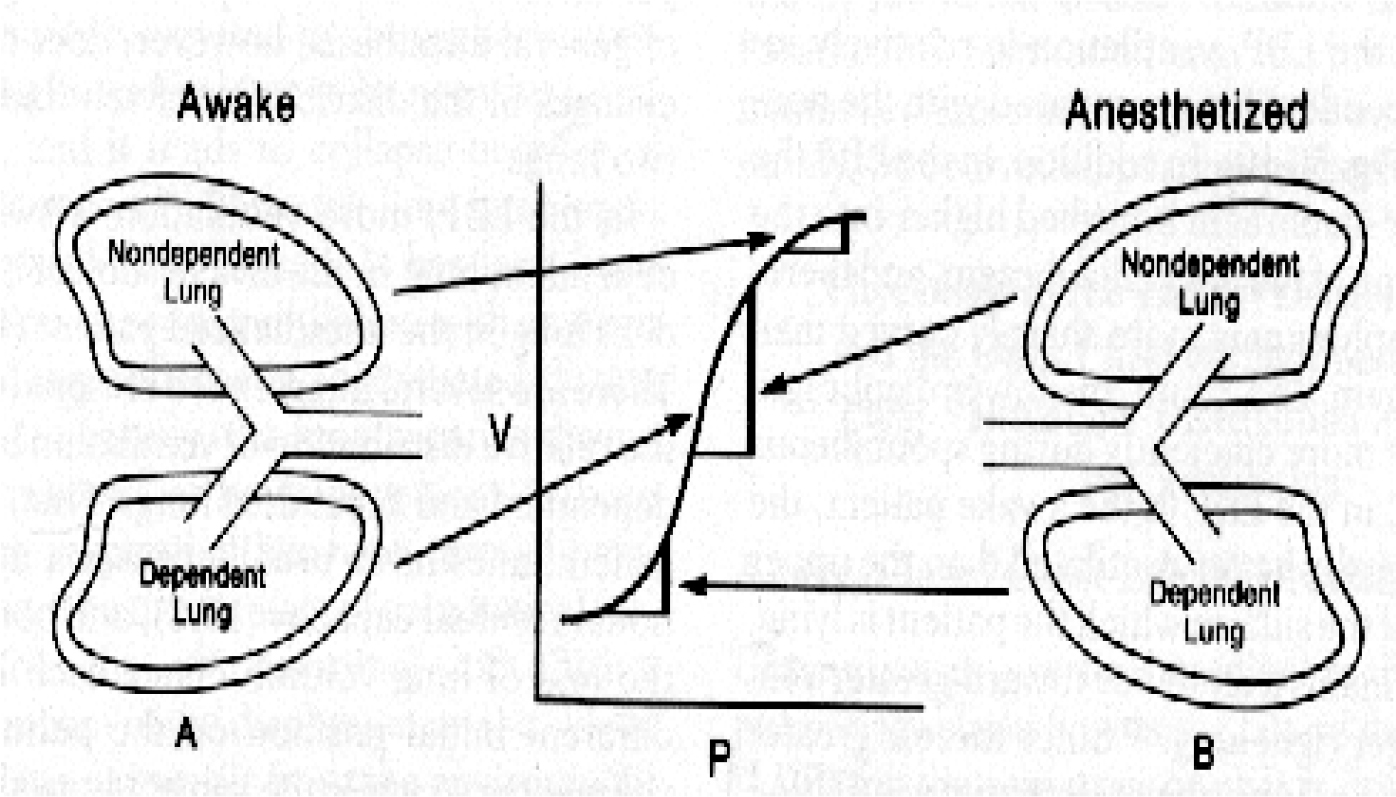
Figure 4: lung compliance curve
When the patient is anaesthetised, the upper lung moves to the position where the lower lung sits on the curve in the awake patient, and the lower lung moves down the curve past the inflection point. The lungs have shifted down the compliance curve (fig 4) and the non-dependent lung becomes easier to ventilate than the dependent lung. When the chest is opened, the top lung becomes even easier to ventilate as there is no restriction by the chest wall. Blood supply is still determined greatly by gravity. V/Q mismatch now occurs. This is even worse when the top lung is collapsed as there is then no ventilation to that lung, but there is still perfusion.
By simple maths, you would expect the shunt to now be 50%, however this is not the case. Mechanical collapse of the lung diverts the blood flow towards the ventilated lung. Lack of ventilation and therefore hypoxia in the collapsed lung causes a phenomenon called hypoxic pulmonary vasoconstriction (HPV), which further diverts blood flow away from the collapsed lung. This protective mechanism, which occurs when alveolar pO2 levels are 4-8 kPa, is inhibited to some extent by vasodilators, including all anaesthetic gases and induction agents. There was a vogue for using propofol total intravenous anaesthesia in preference to volatile agents in an attempt to reduce HPV, however it has been shown that HPV is not inhibited by MAC values less than 1%. 1 MAC of isoflurane only inhibits HPV by 20% so it is not clinically a big problem and there is no reason to avoid volatile agents.
The disease itself may have altered the lung physiology. A large tumour may already be obstructing ventilation and so collapse of this lung may not alter the patient’s oxygenation.
You will have been taught that a patient needs a tidal volume of 7-10 mls/kg during ventilation. During one lung anaesthesia, a balance has to be struck between having enough tidal volume for gas exchange and not too high a peak inspiratory pressure i.e. greater than about 30 cm H2O to avoid barotrauma. A higher than normal level of carbon dioxide, known as ‘permissive hypercapnia’ may need to be tolerated.
Overcoming hypoxia during OLV
Because of the above changes in lung physiology, it is not uncommon for a patient to desaturate during OLV. If this happens, tell the surgeon early rather than waiting for the saturations to plummet. It may be that you have to reinflate the lung temporarily, and the surgeon may have to, for example, finish tying off a blood vessel before his vision is obscured. Turn the inspired oxygen up to 100%. Make sure that the patient’s blood pressure has not dropped as this may be the cause of desaturation. Sometimes hypotension is mechanical due to pressure on the mediastinum by the surgeon.
Tube patency and position should be checked. Secretions may be blocking the tube lumen. Look at the capnograph trace. If it has changed, as a general rule the tube has moved. Even if you have carefully tied it in place, movement may occur from within the chest during manipulation of the mediastinum. Bronchoscopy will confirm this and allow the tube to be repositioned.
Now that you have confirmed the tube is patent and in the correct position, and that the patient has a normal cardiac output, there are other actions that can improve oxygenation. Sometimes switching from machine ventilation to manual ventilation can be helpful. By giving the patient a larger breath by hand with sustained pressure at the end of the breath, you may recruit collapsed alveoli. If this works, then applying positive end expiratory pressure (PEEP) to the ventilated lung, in the form of a valve attached to the expiratory limb of the breathing circuit, may help to prevent these small airways from closing. Usually 5cm H2O is enough to keep the saturation up without pushing the peak inspiratory pressure too high (above about 30 cm H2O) and causing barotrauma. Also, if PEEP is too high, blood is diverted to the non-ventilated lung and shunt is increased, worsening the hypoxia.
Oxygen can be insufflated down the collapsed lung by using a small suction catheter attached to an oxygen flowmeter. The catheter needs to be small enough not to occlude the tube lumen or the lung will merely inflate. Similarly , the flow of oxygen must be low, in the region of 2 litres/minute, or the lung will inflate. The theory is that this oxygen will diffuse into blood vessels that have not collapsed due to hypoxic pulmonary vasoconstriction. In practice, it is not terribly effective.
Application of continuous positive pressure (CPAP) to the non-ventilated lung may help to reduce shunt by diverting blood to the ventilated lung. Purpose made valves exist for this.
It may be that you have to compromise and settle for saturations in the low 90s.
If these methods all fail, the collapsed lung must be reinflated and the patient ventilated with 100% oxygen. If a pneumonectomy is being carried out, the surgeon may decide at this point to clamp the pulmonary artery. This will improve shunting when the lung is recollapsed as the lung will have no blood supply. It may be that surgery has to be abandonned as the patient will not tolerate one lung anaesthesia.
Further reading
- Gosh S, Latimer R.D. Thoracic anaesthesia :principles and practice. Oxford: Butterworth Heinemann; 1999
- Gothard J, Kelleher A, Haxby E. Cardiovascular and thoracic anaesthesia in a nutshell. Butterworth Heinemann 2003.
- West JB. Respiratory Physiology-the essentials. Williams & Wilkins, USA.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/