Basic Sciences

Children are not small adults. Paediatric patients vary considerably and include the following groups:
- Neonates – a baby within 44 weeks of age from the date of conception
- Infants – a child of up to 12 months of age
- Child – 1 to 12 years
- Adolescent – 13 to 16 years
The differences between paediatric and adult anaesthetic practice are reduced as the patients become older.
The important anatomical and physiological differences will be considered below followed by a discussion of how these will affect anaesthetic practice.
a. Airway and Respiratory System
- They have a large head, short neck and a prominent occiput.
- The tongue is relatively large.
- The larynx is high and anterior, at the level of C3 – C4. The epiglottis is long, stiff and U-shaped. It flops posteriorly. The ‘sniffing the morning air’ position will not help bag mask ventilation or to visualise the glottis. The head needs to be in a neutral position.
- Neonates preferentially breathe through their nose. Their narrow nasal passages are easily blocked by secretions and may be damaged by a nasogastric tube or a nasally placed endotracheal tube. 50% of airway resistance is from the nasal passages.
- The airway is funnel shaped and narrowest at the level of the cricoid cartilage. Here, the epithelium is loosely bound to the underlying tissue. Trauma to the airway easily results in oedema. One millimetre of oedema can narrow a baby’s airway by 60% (Resistance ∝ 1/radius). It is suggested that a leak be present around the endotracheal tube to prevent trauma resulting in subglottic oedema and subsequent post-extubation stridor.
- An endotracheal tube must be inserted to the correct length to sit at least 1cm above the carina and be taped securely so as to prevent tube dislodgement with head movement, or an endobronchial intubation.
- The neonate and infant have limited respiratory reserve.
- Horizontal ribs prevent the ‘bucket handle’ action seen in adult breathing and limit an increase in tidal volume. Ventilation is primarily diaphragmatic. Bulky abdominal organs or a stomach filled with gases from poor bag mask ventilation can impinge on the contents of the chest and splint the diaphragm, reducing the ability to ventilate adequately.
- The chest wall is significantly more compliant than that of an adult. Subsequently, the functional residual capacity (FRC) is relatively low. FRC decreases with apnoea and anaesthesia causing lung collapse.
- Minute ventilation is rate dependant as there is little means to increase tidal volume.
- The closing volume is larger than the FRC until 6-8 years of age. This causes an increased tendency for airway closure at end expiration. Thus, neonates and infants generally need IPPV during anaesthesia and would benefit from a higher respiratory rate and the use of PEEP. CPAP during spontaneous ventilation improves oxygenation and decreases the work of breathing.
- Work of respiration may be 15% of oxygen consumption.
- Muscles of ventilation are easily subject to fatigue due to low percentage of Type I muscle fibres in the diaphragm. This number increases to the adult level over the first year of life.
- The alveoli are thick walled at birth. There is only 10% of the total number of alveoli found in adults. The alveoli clusters develop over the first 8 years of life.
- Apnoeas are common post operatively in premature infants. Apnoeas are significant if they last longer than 15 seconds and are associated with desaturation or bradycardia. Caffeine 10-20 mg/kg oral or IV given peri-operatively may be useful.
- RR = 24 – age/2
- Spontaneous ventilation TV = 6-8 ml/kg; IPPV TV = 7-10ml/kg
- Physiological dead space = 30% and is increased by anaesthetic equipment.
b. Cardiovascular System
- In neonates the myocardium is less contractile causing the ventricles to be less compliant and less able to generate tension during contraction. This limits the size of the stroke volume. Cardiac output is therefore rate dependent. The infant behaves as with a fixed cardiac output state. Vagal parasympathetic tone is the most dominant, which makes neonates and infants more prone to bradycardias.
- Bradycardia is associated with reduced cardiac output. Bradycardia associated with hypoxia should be treated with oxygen and ventilation initially. External cardiac compression will be required in the neonate with a heart rate of 60 beats per minute or less, or 60-80 beats per minute with adequate ventilation.
- Cardiac output is 300-400 ml/kg/min at birth and 200 ml/kg/min within a few months.
- Sinus arrhythmia is common in children and all other irregular rhythms are abnormal.
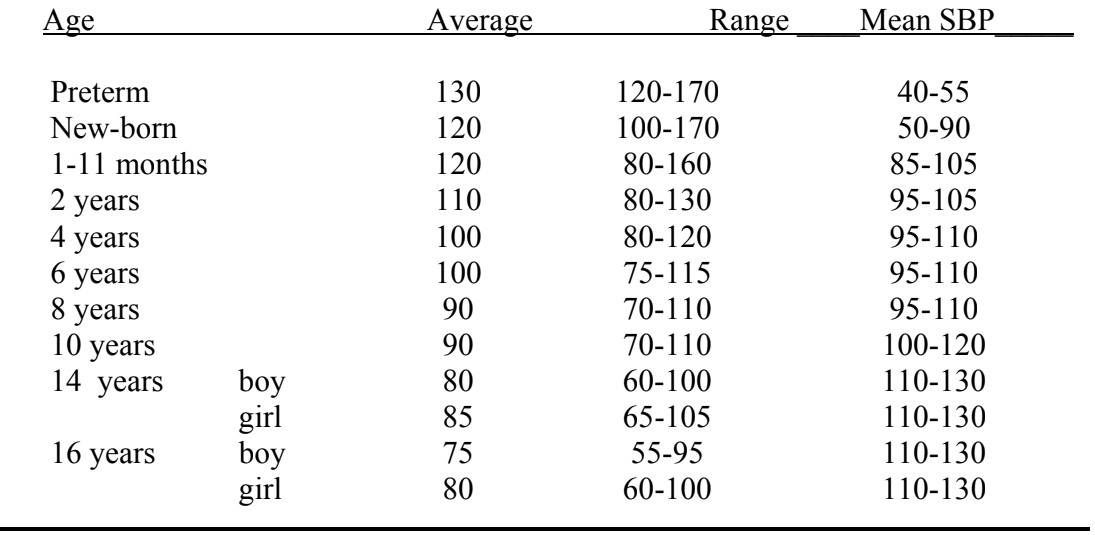
Normal Heart Rates (beats/min) and Systolic Blood Pressure (mmHg)
- The patent ductus contracts in the first few days of life and will fibrose within 2-4 weeks. Closure of the foramen ovale is pressure dependent and closes in the first day of life but it may reopen within the next 5 years. The neonatal pulmonary vasculature reacts to the rise in Pa02 and pH and the fall in PaCO2 at birth. However, with alterations in pressure and in response to hypoxia and acidosis, reversion to the transitional circulation may occur in the first few weeks after birth.
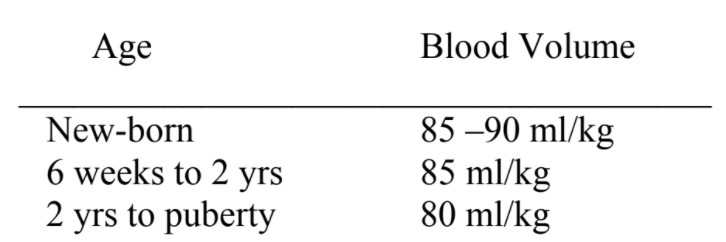
Normal Blood Volumes
c. Renal System
- Renal blood flow and glomerular filtration are low in the first 2 years of life due to high renal vascular resistance. Tubular function is immature until 8months, so infants are unable to excrete a large sodium load.
- Dehydration is poorly tolerated. Premature infants have increased insensible losses as that have a large surface area large surface area relative to weight. There is a larger proportion of extra cellular fluid in children (40% body weight as compared to 20% in the adult).
- Urine output 1-2 ml/kg/hr
d. Hepatic System
- Liver function is initially immature with decreased function of hepatic enzymes. Barbiturates and opioids for example have a longer duration of action due to the slower metabolism.
e. Glucose Metabolism
- Hypoglycaemia is common in the stressed neonate and glucose levels should be monitored regularly. Glycogen stores are located in the liver and myocardium. Neurological damage may result from hypoglycaemia so an infusion of 10% glucose may be used to prevent this. Infants and older children maintain blood glucose better and rarely need glucose infusions.
- Hyperglycaemia is usually iatrogenic
f. Haematology
- At birth, 70-90% of the haemoglobin molecules are HbF. Within 3 months the levels of HbF drop to around 5% and HbA predominates. A haemoglobin level in a newborn will be around 18-20 g/dl which is a haematocrit of about 0.6. The haemoglobin levels drop over 3-6 months to 9-12 g/dl as the increase in circulating volume increases more rapidly the bone marrow function.
- HbF combines more readily with oxygen but is then released less readily as there is less 2,3-DPG. HbF is protective against red cell sickling.
- The 02/Hb dissociation curve shifts to the right as levels of HbA and 2,3-DPG rise.
- The vitamin K dependent clotting factors (II, VII, IX, X) and platelet function are deficient in the first few months. Vitamin K is given at birth to prevent haemorrhagic disease of the newborn.
- Transfusion is generally recommended when 15% of the circulating blood volume has been lost.
g. Temperature Control
- Babies and infants have a large surface area to weight ratio with minimal subcutaneous fat. They have poorly developed shivering, sweating and vasoconstriction mechanisms.
- Brown fat (located in small amounts around the scapulae, the mediastinum, the kidneys and adrenal glands) metabolism is required for non-shivering thermogenesis. It comprises 2-6% of neonatal body weight. More oxygen is required for the metabolism of these brown fat stores.
- Heat lost during anaesthesia is mostly via radiation but may also be lost by conduction, convection and evaporation. The optimal ambient temperature to prevent heat loss is 34ºC for the premature infant, 32ºC for neonates and 28ºC in adolescents and adults.
- Low body temperature causes respiratory depression, acidosis, decreased cardiac output, increases the duration of action of drugs, decreases platelet function and increases the risk of infection.
h. Central Nervous System
- Neonates can appreciate pain and this is associated with increased heart rate, blood pressure and a neuro-endocrine response.
- Narcotics depress the ventilation response to a rise in PaC02.
- The blood brain barrier is poorly formed. Drugs such as barbiturates, opioids, antibiotics and bilirubin cross the blood brain barrier easily causing a prolonged and variable duration of action.
- The cerebral vessels in the preterm infant are thin walled, fragile. They are prone to intraventricular haemorrhages. The risk is increased with hypoxia, hypercarbia, hypernatraemia, low haematocrit, awake airway manipulations, rapid bicarbonate administration and fluctuations in blood pressure and cerebral blood flow. Cerebral autoregulation is present and functional from birth.
i. Psychology
- Infants less than 6 months of age are not usually upset by separation from their parents and will more readily accept a stranger.
- Children up to 4 years of age are upset by the separation from their parents and the unfamiliar people and surroundings. It is difficult to rationalise with a child of this age. The behaviour of this group is more unpredictable.
- School age children are more upset by the surgical procedure, its mutilating effects and the possibility of pain.
- Adolescents fear narcosis and pain, the loss of control and the possibility of not being able to cope with the illness. This is worsened by long periods of hospitalisation.
- Parental anxiety is readily perceived and reacted on by the child.
Practicalities for Anaesthetising Children
j. Pre-operative Visit
Use this time to develop rapport and trust with the child and parent. Address the child first and then include the parents in discussion. Address the queries and fears of the child as well as those of the parent. Explain the planned approach to induction so both parent and child know what to expect.
It is important to take a medical and anaesthetic history.
- Any previous problems with anaesthetics including family history
- Allergies
- Previous medical problems including congenital anomalies
- Recent respiratory illness
- Current medications
- Recent immunisations
- Fasting times
- Presence of loose teeth.
Conduct a physical examination as appropriate concentrating on the airway and cardiorespiratory systems.
Children must be weighed. All drug doses relate to body weight.
Weight (kg) can be estimated by: (age + 4) x 2. This is less accurate over 10 years.
Investigations may occasionally be necessary:
- Haemoglobin – large expected blood loss, premature infants, systemic disease, congenital heart disease
- Electrolytes – renal or metabolic disease, intravenous fluids, dehydration
- CXR – active respiratory disease, scoliosis, congenital heart disease
Discuss post-operative pain management. If suppository medications are to be used, consent should be obtained from the parent and the child if they are able to understand.
k. Pre-operative Fasting
- 6 hours for solids and milk if greater than 12 months of age
- 4 hours for breast milk and formula feeds if less than 12 months of age
- 2 hours for unlimited clear fluids (as this decreases gastric acidity and volume)
- There is an increased incidence of nausea and vomiting with long fasting periods.
l. Pre-medication
In our institution, sedative pre-medication is infrequently used. Psychological preparation and enlisting the help of the parents may decrease the need for sedative pre-medication.
Sedation has a significant failure rate, tastes bad, increases time spent in recovery and delays discharge for day stay procedures. However, an appropriately chosen drug, timed correctly can produce a calm or cooperative child.
We most commonly use analgesic pre-medication drugs such as paracetamol, ibuprofen or codeine phosphate given more than a half hour pre-operatively. EMLA or amethocaine cream is applied to identifiable veins on those children for whom an intravenous induction is planned. Allergy is possible to both these topical anaesthetic agents.
The following sedative medications may be useful:
- Midazolam 0.5 mg/kg with a maximum of 15 mg given orally 15-30 minutes preoperatively. It has a variable result and can produce a very unpleasant excitatory phase. Timing is important for best effect. A sweetener may be necessary.
- Chloral hydrate 50 mg/kg orally to a maximum of 1g. This also can produce an unpleasant excitatory phase and has a bitter taste. It is also used for sedation.
- Ketamine 3-8 mg/kg orally 30-60 minutes pre-operatively.
- Temazepam 0.5-1 mg/kg orally for older children 1 hour pre-operatively.
- Clonidine 2-4mcg/kg orally. It may cause hypotension.
Beware narcotics in infancy because of apnoea.
Sedation should be used cautiously in those children with airway problems and should be avoided altogether in neurosurgical patients especially if they have raised intracranial pressure.
m. Preparation for Anaesthesia
A parent may join their child at the time of induction. It is not compulsory but can be useful in many instances. There must be a member of staff available to accompany the parent from the anaesthetic room after induction. It must be remembered that being present at induction can be very stressful for the parent.
Warm the theatre and prepare any warming devices. Keeping children warm can be a simple thing to do to improve post-operative wellbeing and outcomes. Use bandages or cotton undercast padding to wrap the limbs and head. Plastic can also be useful to prevent radiant heat loss.
Prepare emergency drugs such as atropine and suxamethonium in a diluted concentration that you are familiar with to make dosing easy if an emergency should arise.
If you do not give anaesthetics to children regularly, calculate and write down the doses of the drugs you may use appropriate for the patient’s weight.
Have your equipment ready and checked.
- Oropharyngeal airway.
- Face masks
- Laryngeal mask
- Endotracheal tube
- Laryngoscope and blades
- Breathing circuit (T piece)
- Monitoring
n. Induction of Anaesthesia
An inhalational induction can be an excellent technique for the child that fears needles or has difficult venous access. However, it is a two person technique. A skilled assistant will need to maintain the airway in the asleep child while intravenous access is obtained. If this help is unavailable, intravenous inductions should be carried out. A correctly sized oropharyngeal airway may be used. Choose one that is the same length as that from the corner of the mouth to the angle of the jaw.
Halothane and sevoflurane are the agents of choice for gaseous induction.
Halothane has a slightly sweet smell and is well tolerated. Induction is moderately slow but the rate is increased with the addition of 50-65% nitrous oxide. Halothane has a slower offset and longer duration of action as it is more soluble. Arrhythmias are more likely to occur. Halothane production is gradually being discontinued in many places.
Sevoflurane is non-irritant and has a more rapid onset and offset of action as it is less soluble. A concentration of 8% can be used initially or it can be wound up gradually. Nitrous oxide use increases the rate and depth of anaesthesia obtained. It has improved haemodynamic stability. MAC values are 3.3 in infants, 2.5 in children and 1.7 in adults. Use is associated with emergence delirium.
The best sites for intravenous access are:
- Back of the hand
- Inner wrist
- Long saphenous vein
- Other veins on the dorsum of the foot
- Cubital fossa veins are difficult to find in infants and tissue easily at this site
Elastoplast, although not sterile, provides a secure means of fixation.
Intravenous induction can be undertaken with propofol, thiopentone or ketamine. Preoxygenation for a rapid sequence induction can be difficult in small children and should be undertaken if able.
o. Intubation
- Straight Magill blades are useful in neonates and infants. A size 0 blade is best in babies less than 4 kg. A curved blade is usually easier once the child is 6-10 kg.
- Uncuffed tubes are used until 8-10 years of age.
- A small leak should be present. The leak is too large if it compromises ventilation.
- Tube size = age/4 + 4.5 is generally a better fit than age/4 + 4 up to 10 years
- Tube length in cm = age/2 +12 (or ID x 3 for an oral ETT and add 2cm for a nasal tube is easier to remember). This is only a guide and the tube length will always need to be checked clinically.
- 1 LMA up to 5 kg; 1.5 LMA 5-10 kg; 2 LMA 10-20 kg; LMA 2.5 20 – 30 kg; LMA 3 for over 30 kg
- Preformed RAE tubes may be too long.
- Secure the endotracheal tube with 1cm wide elastoplast, ensuring that the tape wraps about the tube and at least one tape is fixed to the less mobile maxilla. Re-check tube length at the time of taping.
p. Maintenance
- Add regional analgesia where necessary
- Beware intravenous narcotics in infancy especially ex-premature infants and neonates.
- Use intravenous fluids for cases with expected blood loss, intra-abdominal, or those taking longer than 30 minutes.
- Extubation laryngospasm tends to occur less frequently if the child is fully awake at the time of extubation.
- You may need to be with a child in recovery until fully awake if the recovery staff are inexperienced with children.
Suggested Reading
- Steward DJ: Manual of Pediatric Anesthesia. Churchill Livingston. (5th Ed.)
- Allman KG, Wilson IH: Oxford Handbook of Anaesthesia. Oxford University Press. (2nd Ed.) 758-785
- Newstead B. Premedication drugs useful in children. Update in Anaesthesia 2005; 19 Article 4
- Mellor J. Induction of anaesthesia in paediatric patients. Update in Anaesthesia 2004; 18 Article 8
- Brown K. The application of basic science to practical paediatric anaesthesia. Update in Anaesthesia 2000; 11 Article 14
Answers to questions on TOTW:
Paediatric anatomy, physiology and the basics of paediatric anaesthesia.
- List as many differences as you can between the anatomy and physiology of babies, children and adults.
- See sections a-h
- If you have difficulty maintaining an airway in a baby what factors may be causing the problem and what can you do about it?
- See section a: large head and high larynx means airway may become obstructed if child is not positioned optimally, eg with head on a pillow, or with head and neck extended. The head needs to be in a neutral position. A large tongue may cause obstruction, a guedel airway may help. An incorrect mask size may result in leaks, have a range available.
- Why should babies and small children be ventilated rather than breathing spontaneously through an endotracheal tube?
- See section a: Endotracheal tubes have a higher resistance than the normal airway as they are long and narrow in diameter. This increases work of breathing.
- How can you tell that a spontaneously breathing child is getting fatigued?
- Respiratory rate will rise initially then fall. Tidal volume will decrease, end tidal CO2 will rise. Eventually they will desaturate, but this is a late sign.
- Why is it important to maintain a normal heart rate in a child?
- See section b: The stroke volume is relatively fixed and cardiac output is rate dependent. Bradycardia will reduce cardiac output. Excessive tachycardia will prevent adequate ventricular filling in diastole.
- How is heat lost? Why does this happen more in smaller children? Why does this matter and how may you prevent hypothermia from happening?
- See sections g and m:
- What should you be looking for on the pre-operative visit to a child?
- See section j.
- What upsets children going for surgery?
- What can you do to help? See sections i, j and l.
- What premedication agents can you use in children?
- See section l.
- What equipment do you have in your hospital for paediatric patients? In what way is it different to that used for adults and why?
- See section o: Equipment comes in different sizes to fit the range of patients you may encounter. Some is just scaled down eg guedel airways or BP cuffs.
- Masks are round for babies as this reduces deadspace.
- Endotracheal tubes are uncuffed to fit at the cricoid ring (the narrowest point). A cuff is unnecessary and may damage the delicate tracheal mucosa.
- Laryngoscopes blades are straight for smaller children as this allows better visualisation of the high anterior larynx than a curved blade.
- The T-piece circuit is used in children less than 20kg as it is lighter and has less deadspace.
- What preparations should you make prior to a child arriving in theatre?
- See section m.
- For what reasons might you choose an intravenous induction rather than inhalation?
- For a rapid sequence induction.
- When a suitable inhalation agent (halothane or sevoflurane) is not available.
- If the patient has malignant hyperpyrexia.
- Patient choice.
- For what reasons might you choose an inhalation induction rather than intravenous?
- Lack of visible veins or failure to cannulate a vein.
- Lack of suitable drugs (including contra-indication or allergy to those you do have).
- Anticipated difficult airway.
- Patient choice.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/