Basic Sciences

SELF ASSESSMENT QUESTIONS
We would recommend that you attempt these stems before reading the tutorial
- Regarding parathyroid glands
a. The chief cells secrete parathyroid hormone
b. They develop from the third and fourth pharyngeal pouches
c. The normal plasma level of intact parathyroid hormone is 10-55pg/mL
d. The most common abnormality is multiple gland hyperplasia
e. Hyperparathyroidism is associated with both MEN type I and II - With regards to calcium metabolism
a. It is the ionised calcium concentration which influences the physiological effects
b. The normal value of ionised calcium is 2.12-2.65mmol/l
c. Calcitonin plays a major role in calcium homeostasis in humans
d. Absorption of Ca2+ from the GI tract is regulated by parathyroid hormone
e. 98-99% of filtered calcium is reabsorbed in the kidney - Regarding hyperparathyroidism
a. The most common cause of primary hyperparathyroidism is a solitary adenoma
b. The majority of patients with hyperparathyroidism are symptomatic at diagnosis
c. The incidence of primary hyperparathyroidism in the UK is thought to be 25 per 100,000
d. The commonest cause of secondary hyperparathyroidism is chronic renal failure
e. Technetium -99 m sestamibi scanning is the most accurate method for the preoperative localization of the parathyroid glands - Regarding anaesthesia for parathyroid surgery
a. An acceptable preoperative calcium level is <3mmol/l
b. The usual indication for surgery is primary hyperparathyroidism from a parathyroid adenoma
c. The intraoperative use of methylene blue can cause a false low SpO2 reading.
d. Minimally invasive parathyroidectomy can be done under superficial cervical plexus block and sedation
e. From an airway obstruction point of view a partial lesion of the recurrent laryngeal nerve is more serious than a complete lesion - With regard to the perioperative management of hyperparathyroidism
a. Intravenous Bisphosphonate is the first line drug therapy in the treatment of life threatening hypercalcaemia
b. Serum calcium should be checked at 6 and 24 hrs after parathyroidectomy
c. Postoperative hypocalcaemia and hypomagnesaemia from “hungry bones” is seen more often after surgery for secondary hyperparathyroidism.
d. Positive Chvostek’s sign refers to carpopedal spasm elicited by cuff inflation.
e. Airway encroachment is common with parathyroid tumours
INTRODUCTION
Endocrine disorders can have a profound influence on human physiological mechanisms and may often affect the management of anaesthesia. Their understanding is important in ensuring a good perioperative outcome. This tutorial intends to briefly review the normal physiology of the parathyroid gland, parathyroid dysfunction and the anaesthetic management of patients presenting for parathyroid surgery.
ANATOMY
The parathyroids normally consist of two pairs of small endocrine glands, two embedded in the superior poles of the thyroid and two in the inferior poles. There can, however, be considerable variations in the location of the individual parathyroid glands and the numbers may also vary. Although commonly seen in close relation to the thyroid glands, they may descend with the thymus into the thorax. Each gland weighs about 50 grams, measures about 3×6 ×2mm, and contains two distinct types of cells, (Chief cells and Oxyphil cells). Chief cells are the more abundant of the two and secrete parathyroid hormone (PTH). The blood supply is derived from the inferior thyroid artery and the veins and lymphatics are shared with the thyroid gland. The vasomotor nerve supply is from the cervical ganglia though the inferior thyroid plexus.
PHYSIOLOGY
Human PTH is a linear polypeptide, with a molecular weight of 9500, containing 84 amino acid residues. PTH plays a central role in maintaining normal calcium homeostasis. The other hormones important in calcium metabolism are vitamin D and calcitonin (not proven to have a dominant effect in humans). The main effector sites responding directly or indirectly to PTH are the intestines, kidneys and bone.
Effects of PTH on kidney
- Increased Ca2+ reabsoprtion due to its effect on the thick ascending loop of Henle, the distal convoluted tubule and the collecting tubule
- Increased phosphate excretion due to a decrease in the reabsorption of phosphate in the proximal tubules.
- Increased bicarbonate and free water clearance
- Potentiation of the formation of vitamin D3 by increasing the activity of vitamin D 1α hydroxylase which converts 25 hydroxycholecalciferol into 1, 25 dihydroxycholecalciferol (vitamin D3) in the renal tubules.
Effects of PTH on bone
PTH acts directly on bone to increase its resorption and mobilises Ca2+ by a complex mechanism that includes both fast and slow components. It also inhibits osteoblasts and stimulates osteoclast activity leading to further absorption.
Effects on intestine
This is an indirect effect caused by an increase in the formation of 1,25–dihydroxycholecalciferol (Vitamin D3) which stimulates Ca2+ absorption from the intestine.
REGULATION OF PTH SECRETION
Serum calcium
Circulating ionised calcium is the main determinant of PTH secretion. Ca2+ acts directly on the parathyroid glands in a negative feedback fashion to regulate PTH secretion by acting though a G protein coupled cell membrane Ca2+ receptor. When the ionised calcium level is high, PTH secretion is inhibited and Ca2+ is deposited in the bone -when low, secretion is increased and Ca2+ is mobilised from the bone.
Vitamin D3 (1, 25 –dihydroxycholecalciferol):
Vitamin D3 acts directly on the parathyroids to decrease PTH gene transcription. It also suppresses the secretory process at low Ca2+ concentrations and increases the intracellular degradation of PTH.
Serum Phosphate
Increased plasma phosphate stimulates PTH secretion by lowering the plasma Ca2+ concentration and inhibiting the formation of 1, 25 –dihydroxycholecalciferol
Magnesium
Magnesium has similar effects on the parathyroids to calcium but has a lesser effect on PTH secretion probably due to the lower overall concentration of Mg2+ relative to Ca2+. Magnesium deficiency can cause impaired PTH release and diminished target organ responses to PTH.
REGULATION OF CALCIUM METABOLISM
There are three principal hormones which regulate Ca levels (ionised Ca2+:`1.0-1.25mmol/l, total Ca2+: 2.12- 2.65mmol/l) are PTH, 1, 25 –dihydroxycholecalciferol and calcitonin.
PTH increases plasma Ca2+ by mobilising it from bone and increasing its resorption in the kidney. It also promotes the conversion of 25 –hydroxycholecalciferol to 1, 25 –dihydroxycholecalciferol in the kidney.
1, 25 –dihydroxycholecalciferol (the active form of vitamin D) increases Ca2+ absorption from the intestine and its resorption in the kidney.
Calcitonin is a hormone secreted by the parafollicular C-cells of the thyroid gland in response to a high plasma Ca2+ concentration. It counters the actions of PTH by inhibiting bone resorption and promoting calcium excretion in the urine. This physiological effect of calcitonin is not demonstrated as strongly in humans as it is in lower animals.
PARATHYROID GLAND DYSFUNCTION
Hyperparathyroidism occurs when excessive secretion of PTH occurs. It is classified as primary, secondary, tertiary or ectopic
PRIMARY HYPERPARATHYROIDISM
The incidence in the UK is estimated to be 25 per 100,000 general population but the increasing use of automated biochemical analysers to measure serum calcium concentrations has influenced the number of cases of primary hyperparathyroidism diagnosed. Primary hyperparathyroidism (PHPT) is usually caused by a single parathyroid adenoma (90%), rarely by multiple adenomas or hyperplasia (10%) and in 1-2% cases by carcinoma. Hyperparathyroidism due to adenoma or hyperplasia is the most common presenting symptom of MEN 1 syndrome (which itself is very rare).
Hypercalcaemia is the hallmark of PHPT which is the most common cause of hypercalcaemia in the general population, whereas malignancy is the commonest cause in hospitalized patients.
Hypercalcemia is responsible for the broad spectrum of signs and symptoms that affect multiple organs systems. Symptoms correlate with changes in the ionised calcium concentration which is the physiologically active form. Ionised calcium is best measured directly using an ion specific electrode.
Clinical features
The majority of patients have minimal symptoms and the classical description of “moans, groans and stones” is seldom seen in clinical practice. This asymptomatic hypercalcaemia is usually discovered as a result of routine biochemistry assay. However, nonspecific symptoms are often encountered.
Renal
Renal dysfunction is more often seen in chronic untreated cases. Nephrolithiasis and proximal tubular dysfunction can occur resulting in a decreased GFR. Persistent hypercalcaemia impairs the urine concentrating ability of the kidney, resulting in polyuria. Advanced cases often result in renal failure.
Skeletal
The classical skeletal abnormality described is Osteitis Fibrosa Cystica. This is less frequently seen nowadays due to early detection and treatment. Radiographic features include osteopenia, subcortical bone resorption in the phalanges and bone cysts. Bone pain and pathological fractures can occur.
Nervous system
Patients may present with nonspecific symptoms which are difficult to quantify. Fatigue, loss of skeletal muscle strength and mass of proximal musculature can be seen. The weakness usually improves following the surgical removal of hypersecreting glands. There may be deficits of memory and cerebration, with or without personality changes or mood disturbances, and the patient may experience hallucinations.
Gastrointestinal
Peptic ulcer disease may occur due to calcium induced gastric hypersecretion and acute and chronic pancreatitis is also associated Non specific abdominal pain can also result which may mimic an acute abdomen.
Cardiovascular
Hypertension is commonly associated with hypercalcaemia as are ECG changes (shortened QT interval and ST segment) and cardiac conduction defects.
Differential diagnosis of hypercalcaemia
- Malignancy (multiple myeloma, lymphoma, bone metastasis, renal cell carcinoma),
- Sarcoidosis,
- Tuberculosis,
- Drug induced (Thiazides, lithium, vitamin D intoxication)
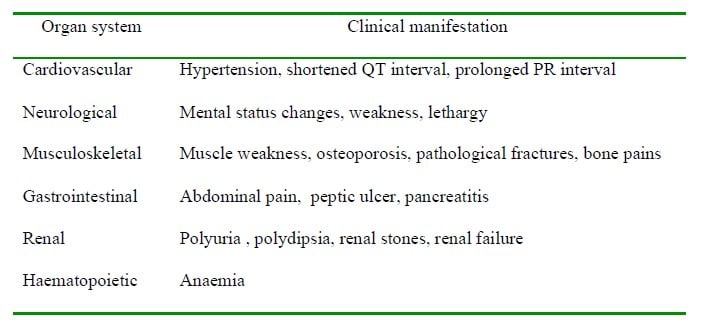
Table1. Clinical features of hyperparathyroidism
Investigations and diagnosis
Biochemical
Hypercalcaemia (corrected for albumin concentration: add 0.1mmol/l for every 5g/l below an albumin concentration of 40g/L), hypophosphatemia, hyperchloraemia, hypercaluria, increased serum parathyroid hormone levels, increased alkaline phosphatase and increased urinary excretion of cyclic amp. may all occur.
Radiological
Parathyroid imaging: Thallium technetium scan, Sestamibi Scintigraphy to locate hyper functioning gland. Preoperative imaging facilitates surgeons in performing minimally invasive parathyroidectomies instead of bilateral neck explorations.
Skeletal imaging:
X- ray of hands to identify periosteal erosions and cystic lesions. DEXA scans for bone density
Treatment
Primary hyperparathyroidism is treated initially by medical management followed by the surgical removal of the affected glands. Although there is an argument in favour of conservative management with follow up bone scans and renal function monitoring for asymptomatic patients, the current trend is to offer surgical treatment for this group of patients. The risks of surgery are outweighed by the logistics involved in the rigorous follow up. Asymptomatic patients are also at risk of renal damage, bone loss, hypercalcaemic crises, and a long term increase in cardiovascular mortality particularly in elderly patients. Symptomatic patients benefit from surgery , their prior medical optimization being dependent on the severity of the hypercalcaemia.
Medical management of hypercalcaemic crisis
A particularly high risk group of patients includes the elderly with undiagnosed disease or advanced malignancy. Severe hypercalcaemia is a medical emergency and treatment should often be initiated before the final diagnosis is complete. Patients may present with dehydration, polyuria, tachycardia, and even psychosis. Dehydration results in anorexia and vomiting which, in turn, worsens the dehydration. Weakness, lethargy and mental changes are common. Extreme cases can lead to coma and collapse.
- Rehydrate: infusion of normal saline (150ml/hr) is the basic treatment. 4-6 litres may be needed.
- Bisphosphonates: Pamidronate 60mg in 500 ml saline over 4 hrs. This is the drug of choice for life threatening hypercalcaemia. They are potent inhibitors of osteoclastic bone reabsorption.
- Calcitonin 3-4U/kg IV then 4U/kg SC bd. This rapidly decreases the skeletal release of calcium and phosphorous but its effects are only temporary
- Life threatening levels of calcium >4.5 mmol/l can be rapidly lowered with phosphate (500ml of 0.1M neutral solution over 6-8 hrs). Again, this effect is transient.
- Forced saline diuresis: is a second line treatment once the dehydration is corrected. Loop diuretics such as furosemide are used (40mg IV every 4hrs.). Frusemide inhibits the proximal tubular reabsorption of calcium. Forced saline diuresis, however, presents a significant risk of fluid overload, electrolyte disturbances and LVF in the elderly, so CVP monitoring should be considered.
- Consider hydrocortisone 200-400mg IV in malignancy induced hypercalcaemia although this is ineffective in primary hyperparathyroidism.
- Haemodialysis in patients with coexisting renal failure.
Surgical management
There are currently two surgical options. The standard procedure involves a bilateral neck exploration and identification of all four parathyroids and subsequent removal of the abnormal or diseased glands. Results would appear to be operator dependent with higher success rates quoted by specialist parathyroid surgeons. Intraoperative localization may be aided by methylene blue injection which is taken up by the glands. This technique is losing popularity due to the incidence of adverse reactions associated with its use. Bilateral neck exploration is preferred in diffuse hyperplasia.
Preoperative localization combined with intraoperative monitoring of PTH levels produces similar success rates during unilateral, minimally invasive parathyroidectomies, while decreasing operating and recovery times. Preoperative imaging using technetium-99 sestamibi scintigraphy and neck ultrasonography helps to identify the size and site of the tumour. Minimal access surgery is undertaken through a 2 cm skin incision over the localized gland. Intraoperative localization can be carried out by using low dose intravenous sestamibi and locating the tumour with a gamma probe. (Minimally invasive radio guided parathyroidectomy). Completeness of resection can be increased by providing real time feed back to the surgeon by rapid PTH assay. Intraoperative PTH monitoring facilitates the use of local anaesthetic techniques and decreases the duration of surgery, thereby allowing ambulatory surgery in the majority of patients.
SECONDARY HYPERPARATHYROIDISM
This condition results from compensatory parathyroid hypertrophy due to a chronic low serum calcium concentration and is most commonly seen in patients with chronic renal failure. (There is no intrinsic abnormality of the parathyroid itself.) Other causes include rickets, osteomalacia, and malabsorption and pseudo hyperparathyroidism. Fewer than 5% of patients with secondary hyperparathyroidism require surgery. The usual presentation is seen in patients suffering from excessive bone reabsorption following long term haemodialysis. Early radiographic lesions include irregularities of the radial aspect of the middle phalanx of the index finger. Other clinical features include vascular and soft tissue calcification involving the kidneys, lungs, heart and skin, and pruritus, proximal myopathies and peptic ulceration may also occur. Radiographic evidence of bone disease in a dialysis dependent patient maximized on medical therapy is an indication to proceed to surgery.
Diagnosis: Hyperphosphataemia with low or normal calcium levels and increased levels of PTH. Alkaline phosphatase levels correlate with the severity of the bone disease.
Medical management
The basic management goals are to maintain calcium and phosphate levels so as to suppress PTH secretion. This is achieved by dietary phosphate restriction, phosphate binding agents, calcium and vitamin D supplements.
Surgical treatment
Medical treatment fails in 5- 10 % of patients with secondary hyperparathyroidism who then require surgery. Preoperative dialysis is indicated within a day of surgery. The bleeding risk is increased due to platelet dysfunction and the use of heparin during haemodialysis. Severe postoperative hypocalcaemia and hypomagnesaemia can occur due to the “hungry bone syndrome”. Surgical options include subtotal parathyroidectomy (with the risk of persistent or recurrent hyperparathyroidism) or total parathyroidectomy plus auto transplantation in the forearm.
TERTIARY HYPERPARATHYROIDISM
Tertiary hyperparathyroidism is characterised by the development of autonomous hypersecretion of parathyroid hormone causing hypercalcaemia.The excessive PTH secretion continues despite correction of the underlying renal disease. Tertiary hyperparathyroidism is observed most commonly in patients with chronic secondary hyperparathyroidism and often after renal transplantation. The hypertrophied parathyroid glands fail to return to normal and continue to oversecrete parathyroid hormone. The clinical manifestations of tertiary hyperparathyroidism include persistent hyperparathyroidism after renal transplantation or new hypercalcemia associated with chronic secondary hyperparathyroidism. Very few patients require surgical intervention (total parathyroidectomy with autotransplantation or subtotal parathyroidectomy ) and the majority become normocalcaemic within a year of successful renal transplantation.
ECTOPIC HYPERPARATHYROIDISM
This condition is due to secretion of a parathyroid hormone like peptide by tissues other than the parathyroid glands. The most likely tissues are carcinomata of the lung, breast, pancreas, or kidney.
ANAESTHETIC CONSIDERATIONS FOR PARATHYROID SURGERY
- The usual indication for surgery is a parathyroid adenoma. Hyperplasia may require all four glands to be taken out. Carcinoma warrants en bloc dissection. Total parathyroidectomy is performed for secondary hyperparathyroidism
- There is no evidence that any specific anaesthetic drug or technique has an obvious advantage over any other. General principles and potential problems are discussed below.
- Traditional bilateral neck explorations require a general anaesthetic. Minimally invasive parathyroidectomy for localized adenomas can be done under local anaesthesia and sedation or a cervical plexus block with sedation. Studies have proven that superficial cervical plexus block with local infiltration is as effective as a combined superficial and deep cervical plexus block with fewer complications.
- Preoperative optimization involves stabilization of the plasma calcium concentration. Levels above 3mmol/l should be corrected using saline infusions and intravenous Pamidronate. Severe hypercalcaemia, however, should be managed as a medical emergency (discussed previously)
- Patients with moderate hypercalcaemia who have normal renal and cardiovascular function present no special preoperative problems.
- Maintenance of hydration and urine output is important in the perioperative management and intravascular volume should be restored and maintained with normal saline. An acceptable preoperative calcium level is <3mmol/l. but if a serum calcium concentration in excess of 3 mmol/l. persists, with ECG abnormalities or if the patient has renal or cardiovascular impairment , surgery should be deferred for optimization.
- Bilateral neck exploration requires a general anaesthetic preferably using a reinforced endotracheal tube or LMA. Airway encroachment by the tumour is rarely seen.
- The patient is positioned in the supine position with a head up tilt and extension of the neck is achieved by placing bolsters under the shoulders. The head is stabilized by a head ring and special care must be taken to protect eyes because of the proximity of surgical retractors.
- Operation times are unpredictable because of the possible difficulty in locating the gland and also any delays caused by the examination of frozen sections. Warming devices may help prevent inadvertent hypothermia. Blood loss is usually minimal.
- If intraoperative methylene blue is used the dose should be restricted to 5mg/kg. and any possible complications anticipated (see above). Rapid infusions can interfere with pulse oximetry readings.
- Anaesthetic requirements may be reduced in patients who exhibit somnolence before induction. The possibility of coexisting renal dysfunction may preclude the use of sevoflurane, although the risk is minimal. If parathyroidectomy is carried out for secondary hyperparathyroidism dialysis must be performed prior to surgery and alfacalcidol started preoperatively and continued through to the post operative period. One should be aware of the possibility of bleeding due to platelet dysfunction.
- Coexisting skeletal muscle weakness suggests the possibility of a decreased requirement for muscle relaxants although hypercalcaemia may be expected to antagonize the action of NDMRs. In view of the unpredictable response to muscle relaxants it is advisable to use a peripheral nerve stimulator in order to titrate an appropriate dose
- Intraoperative ECG monitoring may detect adverse effects of hypercalcaemia.
- The careful positioning of patients is necessary as the presence of osteoporosis is likely and the risk of pathological fractures high
- One should be aware of the various complications which may occur, including bleeding, metabolic abnormalities, recurrent laryngeal nerve trauma, oedema of the glottis and hypocalcaemic tetany.
- Bilateral recurrent laryngeal nerve injury induced by trauma or oedema will cause stridor and laryngeal obstruction due to unopposed adduction of cords but, fortunately, is extremely rare. Management of this complication consists of intubation followed by surgical tracheostomy. Unilateral nerve injury is characterized by hoarseness. It is good practice to check the position of the vocal cords during extubation to exclude recurrent laryngeal nerve damage.
- Electrolyte imbalances: after parathyroidectomy magnesium or calcium may be redistributed internally into ‘’hungry bones’’ causing hypomagnesaemia, hypocalcaemia or both.
Postoperative care
Serum calcium levels should be checked at 6 and 24 hrs post operatively. The continued use of alfacalcidol lowers the risk of postoperative hypocalcaemia. If recurrent laryngeal nerve injury is suspected nasendoscopy should be performed. Post operative pain relief can normally be managed by oral analgesia especially if a technique involving the infiltration of a local anaesthetic has been used.
HYPOPARATHYROIDISM
The condition results from a deficiency of PTH. The commonest cause is the inadvertent removal of the parathyroid glands during surgical thyroidectomy but other causes include conditions where there is a resistance of peripheral tissues to the effects of PTH. e.g.: congenital pseudohypoparathyroidism
The clinical features are due to low ionised calcium levels and the signs and symptoms depend on the speed of development of the hypocalcaemia. Acute hypocalcaemia manifests as perioral paraesthesia, restlessness, neuromuscular irritability and stridor. Chronic hypocalcaemia causes fatigue, muscle cramps, lethargy, personality changes, and cerebration defects.
The treatment of acute hypocalcaemia is the intravenous infusion of 10% calcium gluconate 10mls until the neuromuscular irritability resolves. Oral calcium and vitamin D supplements help.
Anaesthetic considerations
Serum calcium should be normalized in any patient with cardiac manifestations. Hyperventilation which will aggravate the clinical situation should be avoided as should rapid transfusions of citrate containing blood products and 5% albumin which might bind and lower the ionised calcium concentration.
ANSWERS TO SELF ASSESSMENT
1. TTTFT 2. TFFFT 3.TFTTT 4. TTTTT 5. TTTFF
Explanations for select questions
1.D False: Most common abnormality is solitary adenoma
1.E True: Multiple Endocrine Neoplasia type 1 characterised by tumours of parathyroid, pancreas and anterior
pituitary (the three P’s in the midline). Hyperparathyroidism is the most common lesion in MEN 1
2.B False: Ionised calcium 1.0-1.25mmol/l, total calcium 2.12-2.65mmol/l
2.C False: Calcitonin is not proven to be of major significance in humans. Calcitonin is secreted by parafollicular c cells of the thyroid in response to high serum calcium. It induces a decrease in serum calcium by inhibiting osteoclastic activity and increasing urinary excretion of calcium. Absolute absence of calcitonin (after thyroidectomy) or absolute excess (medullary carcinoma thyroid) has no major effect on calcium metabolism.
2 D False: Absorption of calcium from the intestine is regulated by 1, 25 –Dihydroxycholecalciferol (active form of vitamin D). PTH by facilitating synthesis of vitamin D3 indirectly promotes calcium absorption.
3 B False: Most patients present with minimal symptoms. Mostly a biochemical diagnosis picked up on routine blood tests. Subtle symptoms can be elicited on detailed history.
5 D false: Carpopedal spasm on inflating the cuff is Trousseau’s sign. Chvostek’s sign is facial twitching on tapping over the facial nerve at the parotid gland.
5 E false: Airway is not a problem preoperatively although complications like glottal oedema, recurrent laryngeal nerve damage, hypocalcaemic tetany/stridor and neck haematoma can cause problems in the post operative period
FURTHER READING
http://courses.washington.edu/conj/bess/calcium/calcium.html
REFERENCES
- R. Mihai and J. R. Farndon. Parathyroid disease and calcium metabolism. British Journal of Anaesthesia (2000);85:29-43
- Hannah Blanshard. Oxford handbook of Anaesthesia. Oxford University Press, UK, 2006;162
- Anna Batchelor. Oxford handbook of Anaesthesia. Oxford University Press, UK, 2006;558
- Review of Medical Physiology,:Hormonal control of calcium metabolism and physiology of bone; Ganong . 22nd Edition, Chapter 21;USA ; 2005,382-395
- Russell T Wall.398-402. Stoelting’s Anesthesia and Co-existing disease, fifth edition, Churchill Livingstone, Philadelphia, 2008; 398-402.
- Michael F. Roizen and Nader M. Enany. Diseases of the endocrine system, Chapter 13, Anesthesia and uncommon disease; Edition: 5,USA, 2005;413-420
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/