General Topics

KEY POINTS
- Pancreatic cancer should be considered in the differential diagnosis of an elderly patient presenting for the first time with pancreatitis.
- Pancreatic cancer is a notorious disease with late presentation, early metastasis, and poor survival rates.
- Resection of pancreas is the most effective treatment for early-stage cancers.
- The role of the multidisciplinary team is crucial in patient selection for surgery, optimization, and postoperative care as pancreatic resection surgery is a complex procedure.
- Adapting an enhanced recovery programme for pancreatic cancer surgery may accelerate recovery by reducing the stress response and improving immune function.
INTRODUCTION
Every year, 8000 new cases of pancreatic cancer (PC) are reported in the United Kingdom, and it is the fifth most common cause of cancer death in both sexes, despite being only the 11th most common cancer overall. This is often due to symptoms appearing once the disease has advanced beyond curative intervention. As a result, only 10% to 20% of patients will have resectable cancer at the time of presentation.1 This article will discuss the perioperative management of patients undergoing treatment for PC.
Anatomy and Physiology of the Pancreas
The pancreas is divided into the head, neck, body, and tail anatomically. It is a secretory organ with both endocrine and exocrine functions, and the parenchyma of the gland is made up of acinar cells. Exocrine products from acinar cells are secreted into a tubular system, which eventually forms the main pancreatic duct. The pancreatic juice (about 1500 mL is secreted daily) contains digestive proteolytic enzymes. The endocrine cells form the Islets of Langerhans, consisting of B (β) cells secreting insulin, A (∝) cells secreting glucagon, and D (δ) cells and F cells secreting pancreatic polypeptide (PP).2 The main function of the pancreas is to aid digestion and blood glucose control. The pathology of the pancreas is summarized in the Table.3
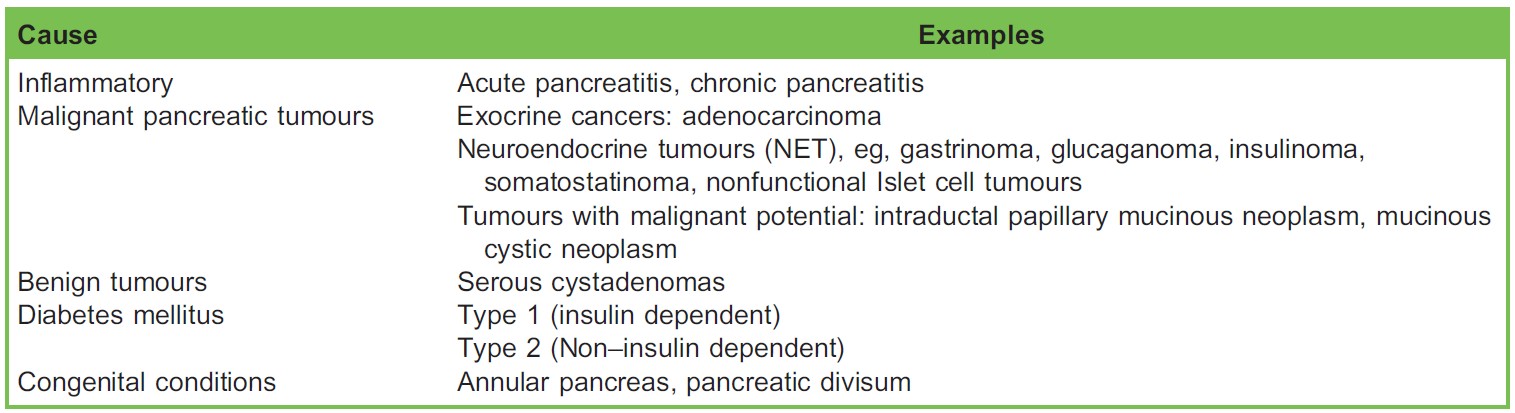
Table. Pancreatic Pathology Classification
Clinical Features of Pancreatic Adenocarcinoma
These tumours are commonly diagnosed in the emergency department, presenting with nonspecific abdominal pain and jaundice or both. Courvoisier sign, described as a palpable gallbladder in the presence of painless jaundice, occurs in less than 25% of patients.3 Unexplained weight loss, steatorrhea, and gastric outlet obstruction due to tumour compressing the duodenum or stomach may result in nausea and satiety.
Risk factors for developing PC include age, smoking, alcohol, raised body mass index, diabetes mellitus, chronic pancreatitis, and family history. It is also associated with familial cancer syndromes, inflammatory bowel disease, peptic ulcer, and periodontal disease.
Diagnosis of PC
Full blood count may reveal normochromic anaemia, thrombocytosis, or both. Patients presenting with obstructive jaundice have significant elevations in serum bilirubin (conjugated and total), alkaline phosphatase, and G-glutamyl transferase. The tumour marker CA19-9 has a sensitivity of 80% and a specificity of 73% for PC.4 Imaging is the most important diagnostic tool in the detection of pancreatic tumours. Ultrasound, computed tomography (CT) scans, and endoscopic ultrasound (EUS) are used in the diagnosis and prognostication of PC. Positron emission tomography scanning can image primary tumours and also detect metastatic disease and is increasingly used in the context of staging of the condition.
TREATMENT MODALITIES
Surgical resection is the only treatment with curative potential for pancreatic adenocarcinoma and is aimed to increase life expectancy.5 Alternative therapy for patients unwilling or medically unfit to undergo major pancreatic resection includes systemic chemotherapy, chemoradiotherapy, surgical bypass, ablative therapies, and gastrointestinal and biliary stenting. Absolute contraindications for pancreatic resection are distant metastases or patient deemed unfit for surgery.3
Pancreatic tumours can involve major blood vessels with associated increased perioperative risk. Evaluation of patients scheduled to undergo vascular reconstruction requires recognition of anatomical variability, extensive preoperative planning, and counselling.
Pancreaticoduodenectomy (Whipple’s procedure)
Most tumours that are associated with the pancreatic head, neck, and uncinate process of the pancreas require pancreaticoduodenectomy (PD). This procedure involves resection of the proximal pancreas, along with the distal stomach, duodenum, distal bile duct, and gall bladder, as an en bloc specimen. Intestinal continuity is restored via a gastrojejunostomy, hepaticojejunostomy, pancreaticojejunostomy, or pancreaticogastrostomy (Figure).
Pylorus-Preserving Pancreaticoduodenectomy (PPPD)
The PPPD is similar to a Whipple’s procedure; however, the pylorus is not resected. The choice depends on the surgeon’s preference and on oncological factors, such as the proximity of the tumour to the duodenum.
Distal Pancreatectomy
This procedure is performed for tumours of the body and tail of the pancreas. The spleen is removed along with the tail of the pancreas, because it lies in close proximity to the tail. After splenectomy, patients will require lifelong antibiotics alongside vaccinations for encapsulated bacteria.
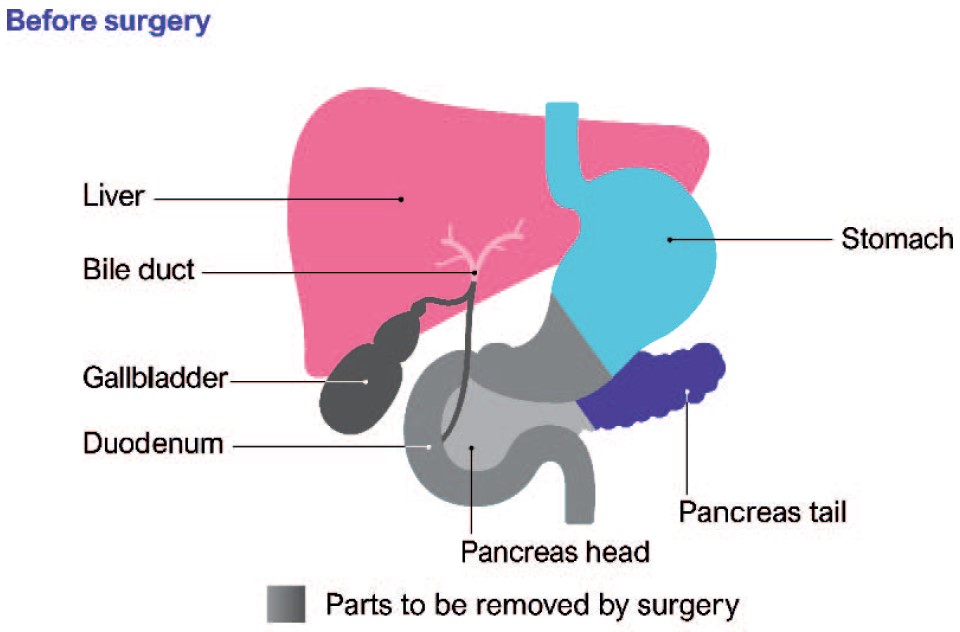
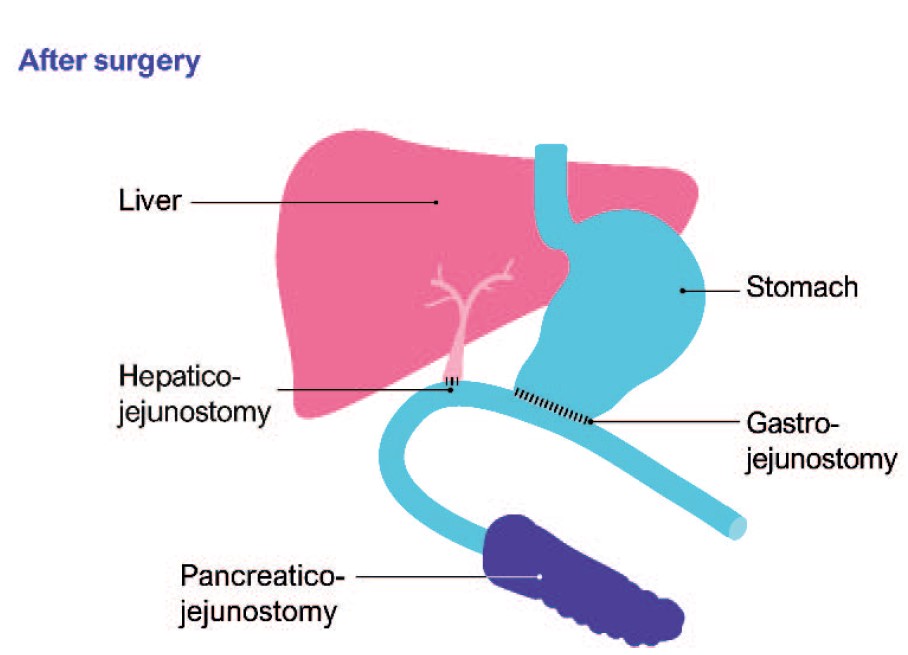
Figure. Before and after pancreaticoduodenectomy. Permission obtained from Pancreatic Cancer UK (https://www.pancreaticcancer.org.uk/).
Total Pancreatectomy
This is not routinely performed in the United Kingdom, as there is no evidence to show better cancer control in comparison to Whipple’s procedure or PPPD.
Laparoscopic Surgery
Pancreatic resection can be approached laparoscopically and is usually carried out for small tumours and tumours of the distal pancreas. Laparoscopic distal pancreatectomy can be safely performed in high-volume centres and results in a shorter time to oral intake and shorter hospital stay.6
Chemotherapy in PC
Agents are used as an adjuvant to surgery before (neoadjuvant) and after (adjuvant) to increase the incidence of disease-free resections and reduce local recurrence. In metastatic PC, the aim is to slow down tumour growth and offer symptomatic benefit, along with radiotherapy. The most commonly used regimen is a combination of gemcitabine with platinum; however, newer combinations including Folfirinox and Abraxane are also in clinical use.
Palliative Treatment for Unresectable Disease
Relieving the biliary tract or duodenal obstruction is a priority in cases of advanced PC and in those cases unfit for major surgery. The aim is to improve symptoms and provide the best possible quality of life. The specific procedures include stent insertion, bypass surgery, or coeliac plexus block to help with pain relief. The stents used to relieve biliary obstruction can be temporary and are inserted to relieve jaundice prior to assessment for surgery. Permanent metal stents are inserted principally for symptom control for those individuals who are not surgical candidates. The biliary stent is inserted via endoscopic retrograde cholangiopancreatography (ERCP) or percutaneous transhepatic cholangiography (PTC). Duodenal stents are inserted by gastroscopy, and these procedures are carried out under sedation or general anaesthesia. The complications associated with stent insertion include blockage by tumour and infection. Bypass surgery is performed when advanced inoperable tumour is detected during exploration, and it involves performing gastro-jejunostomy to relieve duodenal obstruction and hepatico-jejunostomy to relieve biliary obstruction.
Pancreatic Neuroendocrine Tumours
These are a group of hormone-secreting tumours of the pancreas, including insulinoma, glucagonoma, gastrinoma, VIPoma, phaeochromocytoma, and carcinoid. Nonfunctioning pancreatic neuroendocrine tumours do not produce hormones. The principle intent of surgery for pancreatic neuroendocrine tumours is curative, palliative, preemptive (to relieve obstruction), or cytoreductive.7 Somatostatin analogues such as octreotide as a perioperative infusion are used for symptom control.
Chronic Pancreatitis
Chronic pancreatitis is a morbid, debilitating condition often associated with chronic abdominal pain, opioid addiction, multiple hospitalizations, and decreased quality of life. Patients with chronic pancreatitis often develop diabetes or pancreatic exocrine insufficiency and are 10 to 20 times more likely to develop PC than the general population. Chronic pancreatitis often leads to multiple diagnostic and therapeutic procedures, including surgery.
PERIOPERATIVE MANAGEMENT
Pancreatic adenocarcinoma is a highly aggressive cancer, so additional investigations should not unduly delay surgery, as this may potentially reduce the benefits of operative intervention. However, in certain cases, less invasive treatment should be considered for patients unwilling or not medically fit enough to undergo major pancreatic surgery. Surgery for pancreatic adenocarcinoma with curative intent has a 5-year survival of 10% to 15% and a median survival of 11 to 18 months.3
Risk Stratification
Pancreatic surgery, especially Whipple’s, has a unique set of conditions, including three different anastomoses, giving rise to complications such as ileus, anastomotic leak, and pancreatic fistula formation. Even though recent developments in surgical management have reduced mortality to less than 5%, pancreatic resection is still accompanied by high morbidity rates (15%- 20%).8 Enhanced recovery programmes have demonstrated benefits for these patients, and the role of the multidisciplinary team is crucial to determine suitability for surgery. The patient should be well informed about the therapeutic procedure and potential complications and be involved in the decision-making process. Although a variety of scoring systems are used to predict morbidity and mortality in the general surgery setting (ie, P-POSSUM), none has been successfully validated in pancreatic surgery. Nevertheless, they provide for a useful adjunct when assessing patients.
Static Testing
Preoperative N-terminal pro b-type natriuretic peptide (NT-pro-BNP) is a useful screening test to identify patients at risk of developing functional heart failure. Raised NT-pro-BNP levels are associated with increased risk of myocardial injury after noncardiac surgery and can be used to guide further investigations, such as echocardiography and postoperative troponin. Guidelines suggest measuring NT-pro-BNP in patients who are 65 years of age or older, who are 45 to 64 years of age with significant cardiovascular disease, or who have a Revised Cardiac Risk Index ≥1.9
A resting echocardiogram should be considered if the patient has a heart murmur and cardiac symptoms (including breathlessness, presyncope, syncope, or chest pain) or signs or symptoms of heart failure. A resting electrocardiogram should be performed first and abnormal findings discussed with the anaesthetist.10
Dynamic Testing
Cardiopulmonary exercise testing has been shown to be a well-tolerated, noninvasive, and cost-effective way to provide a global assessment of cardiovascular, respiratory, and skeletal muscle systems.11 Selected cardiopulmonary exercise testing variables have a predictive value in determining postoperative complications and length of hospital stay in intra-abdominal surgery. Dobutamine stress echocardiography may be indicated in patients unable to exercise due to musculoskeletal impairment. A positive test indicates urgent referral for cardiology review.
Role of Enhanced Recovery After Surgery in the Perioperative Care of Patients for PD
Enhanced recovery programmes are multimodal strategies that aim to attenuate the loss of functional capacity after surgery and improve its restoration. Morbidity is reduced and recovery enhanced by reducing surgical stress, optimal control of pain, early oral diet, and early mobilisation. Overall, pathway adherence is paramount in achieving successful outcomes.12
Preoperative strategies
- Preoperative counselling may diminish anxiety and help to enhance postoperative recovery and discharge. Information leaflets or multimedia information may contribute to early mobilisation, feeding, and pain management.
- Smoking and alcohol cessation for at least 1 month prior to PD is beneficial.
- There is increasing evidence that improving or maintaining fitness in the perioperative period leads to improved outcomes. Even though there is some controversy regarding the length and intensity of exercise, the evidence trend suggests exercise to be of benefit.
- Preoperative carbohydrate drinks are recommended in patients without diabetes.
- Adequate thromboprophylaxis should be considered for 4 weeks after hospital discharge.12
Management of Preoperative Anaemia
Anaemia is common in patients undergoing hepato-pancreatico-biliary (HPB) surgery and can be related to nutritional deficiency and/or anaemia of chronic disease. If anaemia is detected on preoperative full blood count, haematinics should be performed (B12, folate, ferritin, and transferrin saturation [TSAT]). If ferritin is <100 μg L–1 and/or TSAT is less than 20%, iron supplementation should be considered. Intravenous iron (ie, ferric carboxymaltose) is usually indicated in view of the urgency of surgery and need to increment haemoglobin rapidly. Folic acid and vitamin B12 can be supplemented if patients are found to be deficient. Further referral to haematology may be indicated.
Preoperative Nutrition
Patients with PC are universally malnourished, and nutritional status should be assessed using a systematic screening tool. The malnutrition universal screening tool for adults has been validated by several studies and is easy and rapid to use. This tool can prompt implementation of effective nutritional interventions, and significantly malnourished patients should be optimised with oral supplements or enteral nutrition preoperatively.
Intraoperative Strategies
- Effective analgesia in PD surgery is important for postoperative respiratory function, compliance with physiotherapy, mobilisation, and prevention of complications.
- Different analgesic strategies are needed for open and laparoscopic surgery.
- The use of midthoracic epidurals is widespread for intraoperative and postoperative analgesia in open pancreatic surgery. Thoracic epidural is associated with superior postoperative analgesia, reduced stress response, decreased incidence of pulmonary or cardiac morbidity, earlier return of intestinal function, and reduced thromboembolic complications.13 For upper transverse incisions, epidural catheters should be inserted between T5 and T8 root levels.
- Patient-controlled analgesia with opioids is the most common modality used as an alternative and is often used for step-down analgesia and in the event of failed regional anaesthesia.
- There is evidence supporting the use of wound catheters or transversus abdominus plane blocks. The POP-UP study demonstrated that continuous wound infiltration is noninferior to epidural analgesia in HPB surgery.14
- Single-shot spinal opioid administration may provide adequate analgesia for both laparoscopic and open pancreatic surgery. Intrathecal morphine and patient-controlled analgesia have been shown to provide acceptable postoperative outcomes in patients undergoing open liver resection.15
- Intravenous bolus ketamine and lignocaine infusion may also have useful roles as analgesic adjuncts.
- Neutral fluid balance should be maintained to avoid salt and water overload, and restrictive fluid administration may improve postoperative outcomes after Whipple’s surgery.16
- Haemo concentration and raised lactate levels are a useful guide to fluid resuscitation, and balanced salt solutions should be used. Mixed venous saturations can be used for determining adequacy of perfusion. Fluid management can be complicated by epidural analgesia, as the resultant hypotension can be interpreted as fluid depletion, and losses during formation of pancreatic and biliary anastomoses may go unnoticed.
- Central venous pressure may help to guide fluid therapy, although it should not be interpreted in isolation of other haemodynamic variables.
- Avoidance of hypothermia and treatment of hyperglycaemia improves outcome.12
- Antibiotic prophylaxis should be used, including repeat dosing during prolonged surgery.
- Depth of anaesthesia monitoring should be considered.
Postoperative Strategies
Early mobilisation should be encouraged from the first postoperative day to meet daily targets as a part of enhanced recovery after surgery. Enteral feeding should be commenced as soon as 12 hours following surgery. Chest physiotherapy and deepbreathing exercises help to prevent pulmonary complications. Maintenance of the patient diary helps to monitor progress and accomplish individual goals.
Postoperative Complications and Management
Pancreatic resection is associated with the general risks that accompany major surgery, including bleeding, chest infection, wound infection, and thromboembolic complications. Mortality from pancreatic surgery is related to systemic complications (including sepsis) and is mostly driven by complications related to the procedure itself (such as leaks from pancreatic anastomosis).17
Pancreatic fistula can result from anastomotic leak and can be a difficult problem to resolve. If there is any suspicion of a pancreatic leak, the amylase concentration of the drain output is measured to confirm the diagnosis (if greater than 100 IU L–1), and the drain should be kept in place until the drainage stops. Patients who have developed pancreatic fistula should be treated for sepsis and malnutrition. Active monitoring of the development of pseudo-aneurysm should be adopted with regular CT scanning, a high level of suspicion, monitoring for haemoglobin drop, or gastrointestinal tract haemorrhage. Postpancreatectomy haemorrhage is best managed nonoperatively via interventional radiology or endoscopy.
Delayed gastric emptying causes discomfort and prolongs hospital stay. Once diagnosed, imaging should be employed to exclude an underlying cause such as intra-abdominal collection or leak. Management options include long-term nasogastric drainage, correction of fluid and electrolyte imbalances, commencement of proton pump inhibitors, and nutritional supplementation.
Pancreatic exocrine insufficiency can occur postpancreatic resection, causing fat malabsorption with a requirement for supplemental pancreatic enzymes (pancreatin).3
Management of Diabetes
Diabetes after pancreatic resection surgery is different from type 1 and type 2 diabetes. It rarely produces ketoacidosis as in type 1, and patients are sensitive to exogenous insulin in comparison with type 2 diabetes. It is more common in patients with total pancreatectomy unless an islet cell transplant has been performed simultaneously.
SUMMARY
Pancreatic surgery is often long and complex. The role of a multidisciplinary professional team is crucial to reduce mortality and morbidity. The anaesthetist plays a key role in the perioperative management of these patients, and close cooperation between surgeons and anaesthetists is vital for reducing complications, enhancing recovery, and ensuring a positive patient experience.
ACKNOWLEDGEMENT
We would like to thank Mr Andreas Prachalias, Consultant Surgeon, Liver Transplantation, Hepato-Biliary & Pancreatic Surgery, King’s College Hospital, for providing assistance with this article.
REFERENCES
- Cancer Research UK. Pancreatic cancer mortality: UK incidence statistics. 2011. http://www.cancerresearchuk.org/ health-professional/cancer-statistics-for-the-uk. Accessed March 30, 2018.
- Young SP, Thompson JP. Severe acute pancreatitis. Contin Educ Anaesth Crit Care Pain. 2008;4:125-128.
- Bond-Smith G, Banga N, Hammond TM, Imber CJ. Pancreatic adenocarcinoma. BMJ. 2012;344:e2476.
- Vallas C, Andia E, Sanchez A, et al. Dual phase helical CT of pancreatic adenocarcinoma: assessment of resectability before surgery. AJR Am K Roentgenol. 2002;178:821-826.
- Kosuri K, Muscarella P, Bekaii-Saab TS. Updates and controversies in the treatment of pancreatic cancer. Clin Adv Hematol Oncol. 2006;4:47-54.
- Briggs CD, Mann CD, Irving GR et al. Systematic review of minimally invasive pancreatic resection. J Gastrointest Surg. 2009;13:1129-1137.
- NET Patient Foundation. Surgery in gastrointestinal and pancreatic neuroendocrine tumours. http://www.netpatientfoundation.org. Accessed March 30, 2018.
- Ho CK, Kleeff J, Friess H, Buchler MW. Complications of pancreatic surgery. HPB (Oxford). 2005;7:99-108.
- Duceppe E, Parlow J, MacDonald P, et al. Canadian Cardiovascular Society guidelines on perioperative cardiac risk assessment and management for patients who undergo noncardiac surgery. Can J Cardiol. 2017;33:17-32.
- National Institute of Health and Care Excellence. Routine preoperative tests for elective surgery. NICE guidelines 2016. nice.org.uk/guidance/ng45. Accessed August 27, 2018.
- Ridgway ZA, Howell SJ. Cardiopulmonary exercise testing: a review of methods and applications in surgical patients. Eur J Anaesthesiol. 2010;27:858-865.
- Lassen K, Coolsen MME, Slim K, et al. Guidelines for perioperative care for pancreaticoduodenctomy: Enhanced Recovery after Surgery (ERASt) society recommendations. Clin Nutr 2012;31:817-830.
- Popping DM, Elia N, Van Aken HK, et al. Impact of epidural analgesia on mortality and morbidity after surgery: systematic review and meta-analysis of randomized controlled trials. Ann Surg. 2014;259:1056-1067.
- Mungroop T, Veelo D, Besselink M, et al. Continuous wound infiltration versus ep idural analgesia after hepato-pancreatobiliary surgery (POP-UP): a randomised controlled, open-label, non-inferiority trial. Lancet Gastroenterol Hepatol. 2016;1:105-113.
- Kasivisvanathan R, Abbassi-Ghadi N, Mallett S, et al. A prospective cohort study of intrathecal versus epidural analgesia for patients undergoing hepatic resection. HPB (Oxford). 2014;16(8):768-775.
- Behman R, Hanna S, Karanicolas P, et al. Impact of fluid resuscitation on major adverse events following pancreaticoduodenectomy. Am J Surg. 2015;210:896-903.
- Pietri LD, Montali R, Begliomini B. Anaesthetic perioperative management of patients with pancreatic cancer. World J Gastroenterol. 2014;20:2304-2320.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/