Covid-19

KEY POINTS
- Coronavirus disease 2019 (COVID-19) mainly transmits via droplets and contact
- Airborne precautions are required for aerosol-generating procedures such as manual ventilation, intubation, extubation, non-invasive ventilation (NIV) and cardiopulmonary resuscitation (CPR)
- Modifications in airway management are required to minimise aerosol generation
- Regional anaesthesia should be considered where possible
- Disease transmission can be minimised when perioperative care is thoroughly planned
INTRODUCTION
The Coronavirus disease 2019 (COVID-19) pandemic is an infection caused by SARS-CoV-2. As of 19 March 2020, there are >200,000 confirmed cases worldwide, claiming nearly 9500 lives.1
The pandemic poses many challenges to the healthcare system particularly in infection control and disease treatment. Healthcare workers accounted for 3.8% of diagnosed cases in China.2 Anaesthesiologists play an important role in the epidemic, as suspected or confirmed cases may require anaesthesia for surgical interventions, as well as airway management expertise in critically ill cases.
In this review we will address current recommendations on infection control and work to identify anaesthetic-specific concerns in managing confirmed / suspected patients perioperatively.
BACKGROUND
The Virus
SARS-CoV-2 is an enveloped, single stranded RNA virus that is 50-200nm in diameter.3 Though genetically 85% similar to SARS-CoV, which was the culprit of the SARS epidemic in 2003, SARS-CoV-2 is a distinctly new coronavirus (see Table 1).
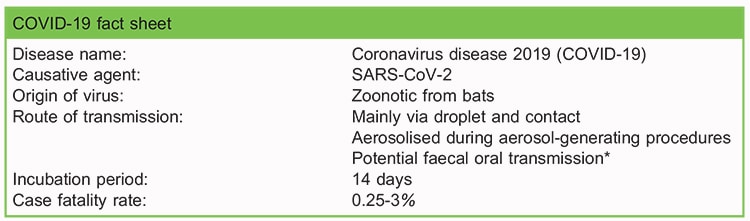
Table 1. Fact sheet on COVID-19 (6, 9). *SARS-CoV-2 is found in faecal material but no known cases of faecal transmission are yet identified. *Case fatality rate is the ratio of deaths to the total number of people diagnosed.
Transmission
The virus first acquired animal-to-human transmission in the wet market in WuHan China in Dec 2019 and eventually sustained human-to-human transmission.3 The major mode of human-to human transmission has been identified as via droplets and direct contact or indirectly from touching shared objects.3 There is currently no known case of established faecal-oral transmission but viral shedding has been found in faecal material.4
Considerable transmission occurs among close contacts particularly within familial households.2 The basic reproductive ratio (R0) is the number of people infected by one confirmed patient, and is used to reflect how contagious a disease is. A R0 > 1 indicates the disease has a greater propensity to spread throughout the community and a R0 < 1 signify a declining epidemic. The R0 for COVID-19 is currently estimated to be 2-3.5 suggesting a growing epidemic (see Table 2).5,6
Clinical Course
Patients present with fever, malaise, respiratory symptoms and occasionally gastrointestinal symptoms (see Table 3). 1% of patients with COVID-19 remain asymptomatic.2,3 In the prodrome period, patients are able to produce virus in the upper respiratory tract despite minimal symptoms, and unknowingly spread the disease.6 The incubation period can last 14 days.7
While 81% of patients have a mild clinical course, 14% have developed severe illness requiring hospitalization and oxygen therapy, and 5% require ICU admission.8 Complications of COVID-19 includes pneumonia, pulmonary oedema, ARDS, multiple organ failure, septic shock requiring hospitalization and death.3 The case fatality ratio, which is the proportion of deaths from the disease, is currently estimated to be 0.25-3%, higher in elderly patients and those who are critically ill.9
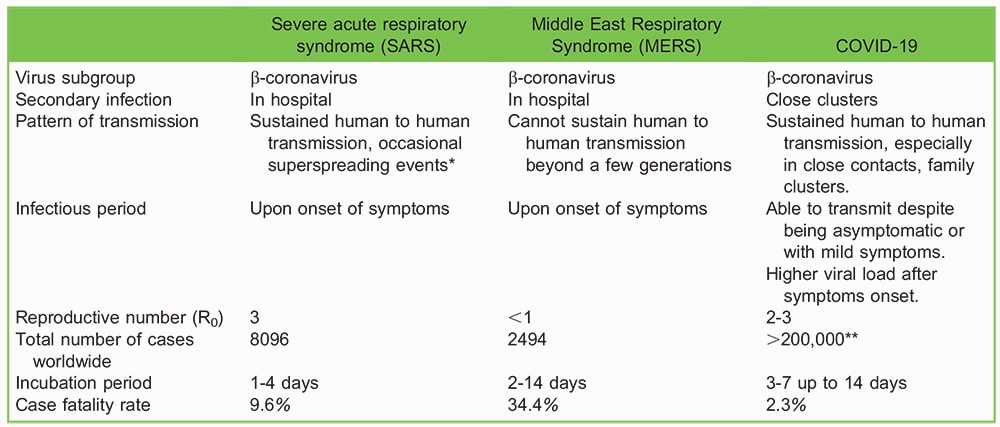
Table 2. Comparison of b-coronaviruses: COVID-19, SARS and MERS (5). *Superspreading events occurs when an exceptionally contagious patient infect more people than would be expected. Mechanism remains unknown. **number of COVID-19 infections as of 19 March 2020, continues to increase
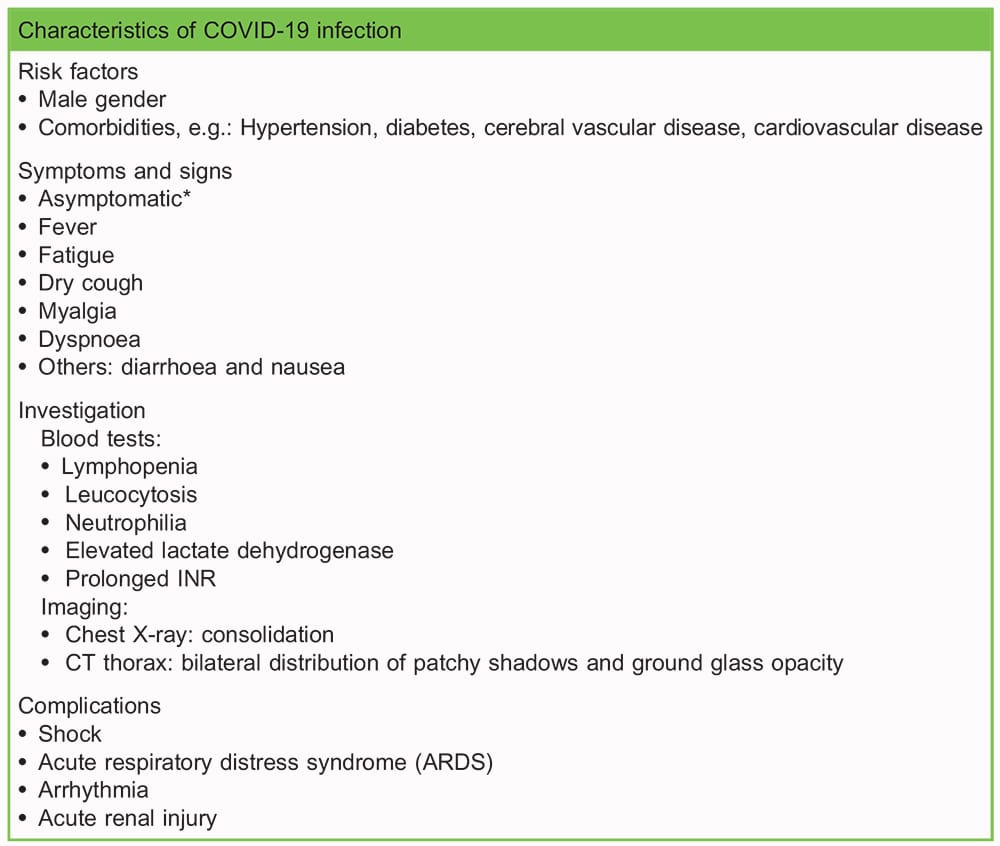
Table 3. Patient characteristics of those infected with COVID-19 (3). *In the incubation period patients may be asymptomatic, but are able to transmit the virus. ~1% patients remain asymptomatic throughout the course of disease. These patients were identified from screening close contacts of confirmed cases.
Diagnosis
Diagnosis is made via two methods. The first is real time reverse-transcriptase polymerase chain reaction (rRT-PCR) of nasal swab and sputum.6 Currently rapid RT PCR test requires 2-4 hours turnover which indicates active infection. The second method of diagnosis is made based on contact history, clinical symptoms, and characteristic CT thorax finding (see Table 3)10, which is particularly useful when rRT-PCR is not available. Serological tests are not the mainstay of initial diagnosis as immunological responses could be delayed. They are primarily used for retrospective assessment of attack rate.11
Potential Treatment
Isolation remains the mainstay of containing COVID-19. Other than supportive treatment with oxygen therapy, anti-viral medications are being tested for their effectiveness against COVID-19. Current experimental treatment may include combinations of Kelatra, Remidesivir, Ribavirin, interferon-1beta and chloroquine.6 Effective treatment regime is yet to be developed and vaccine development is under way.6
The Centers for Disease Control and Prevention (CDC) currently recommends that discharge from hospital/isolation requires negative rRT PCR results from at least 2 consecutive sets of nasopharyngeal and throat swabs collected at least 24 hours apart from a patient with COVID-19.12
INFECTION CONTROL
In addition to standard precautions, droplet precaution and contact precaution should be applied to patients who are highly suspected or confirmed to have COVID-19.13,14 Aerosol-generating procedures (AGP) induce tiny droplets ,5 lm which can travel further and stay suspended in air longer compared to larger droplets. When these procedures are involved, airborne precautions should also be employed (See figure 1).14
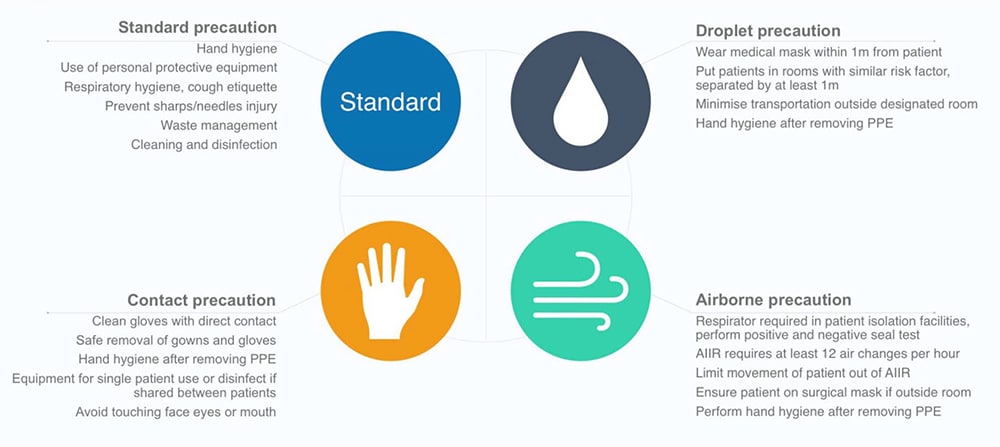
Figure 1. Different standards of infection control precautions as recommended by World Health Organisation (18)Droplet precaution and contact precaution should be applied to patients who are highly suspected or have confirmed to have COVID-19. Airborne precaution also applied for AGP which requires fit-tested N95 (P2) respirators, eye protection, gown, gloves and caps. AIIR = Airborne Infection Isolation Room
Procedures that are classified as aerosol-generating include: tracheal intubation, non-invasive ventilation (NIV), cardiopul- monary resuscitation (CPR), manual ventilation before intubation, tracheostomy, airway suctioning and bronchoscopy. Anaesthesiologists actively participate in AGP within a close distance and are thus exposed to increased risks.
ROLE OF HOSPITAL AND DEPARTMENT
Caring for suspected and confirmed cases requires concerted efforts from hospital administration and frontline health care workers across all disciplines. The following measures are recommended:
Develop a Diagnosis, Management and Precaution Protocol and Workflow Guidelines
- Facilitate triage and prompt diagnosis
- Develop clear work flow guidelines help to facilitate multi-disciplinary communication among the managing team, medical team, infection control team, and intensive care unit to implement isolation practices.
- Systems integration testing of workflow guidelines using medical simulation helps to ensure robustness.
Training/Education
- Information on disease transmission and prevention to be relayed to all theatre staff to encourage adherence to infection control protocols, possibly via hospital publications and online tutorials.
- Organise training on proper donning and doffing of personal protective equipment (PPE) including N95 respirator, goggles, face shield, gowns and gloves.
- Familiarise theatre staff with the location of gown up (usually outside isolation room) and gown down PPE protocols to avoid cross contamination.
- Conduct simulations involving anaesthesiologists, anaesthetic nurses or assistants to familiarise with modifications in workflow, particularly on induction, extubation, airway crises and cardiopulmonary resuscitation.
- Design cognitive aids to facilitate information consolidation (see Figure 2).
Personal Protective Equipment (PPE)
According to the World Health Organisation(WHO) and CDC recommendations, fit-tested N95 (P2) respirators, eye protection, gown, gloves and caps are necessary for AGP(13). Powered air purifying respirators (PAPRs) have a higher protective factor compared with N95 respirators, but there is no definitive evidence that PAPRs reduce the likelihood of viral transmission.15
When aerosol generating procedures are not involved, PPE requirements may change according to the situation. Risk assessment of the procedure involved, prevalence of disease in locality and availability of resources should be taken into account.
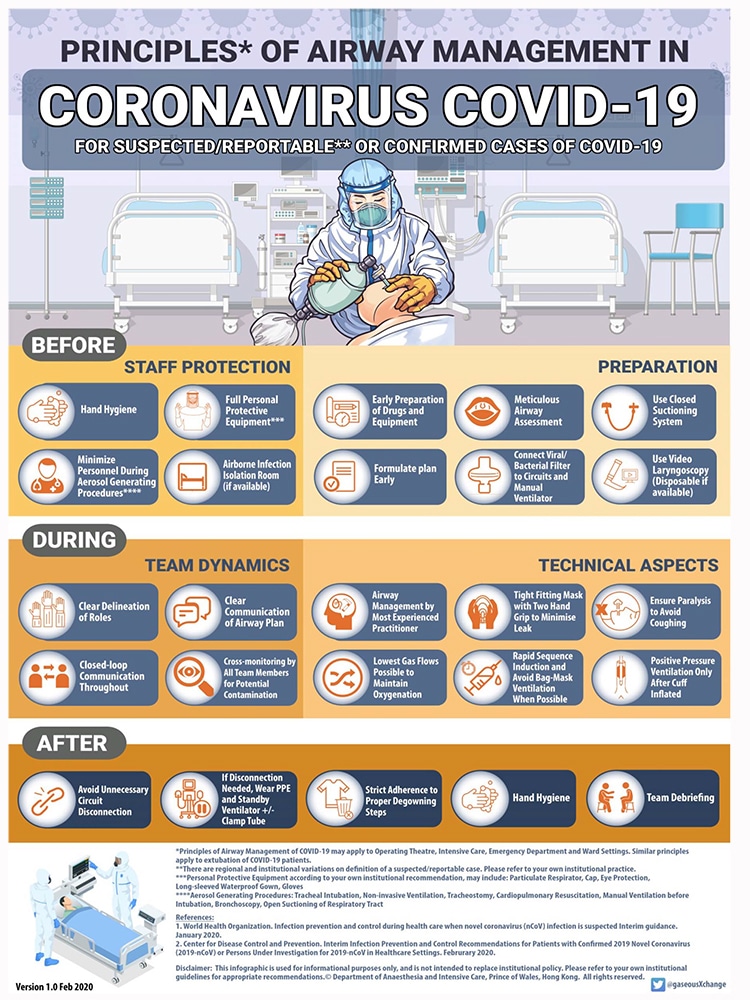
Figure 2. Example of cognitive aid on airway management for patients with COVID-19 reproduced with permission from Prince of Wales Hospital, Hong Kong
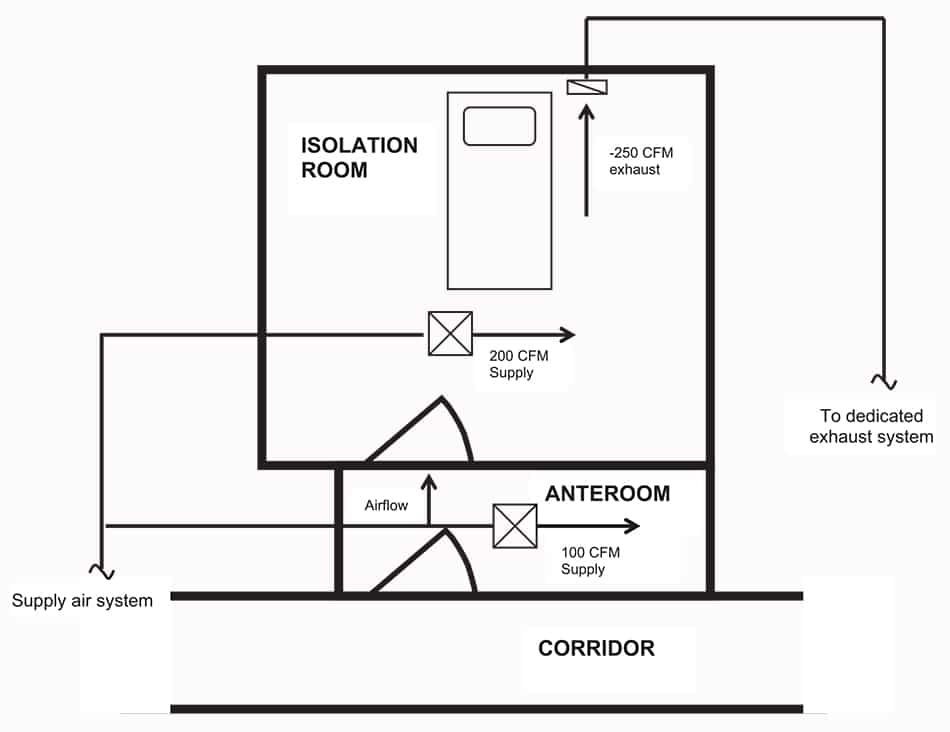
Figure 3. Airborne infection isolation (AIIR) requirement Ventilation: ensure more than 12 air changes per hourGood air mixing and directional airflow: clear air introduced near a health care worker while exhaust air removed near the patient Negative pressure: generated when exhaust air exceeds supply air, and room is well-sealed except for a gap under door. Integrity tested by smoker test. Exhaust ductwork integrity: rule out leaks, if recirculating air system is used, high-efficiency particulate air (HEPA) filter should be installed Anteroom: provide ‘‘air lock’’ between the AIIR and the corridor, preventing infectious particles from escaping, should be at positive pressure with respect to AIIR and negative or neutral with respect to the corridor Cubic feet per minute (CFM) is a measurement of the velocity at which air flows into or out of a space. (Figure reproduced with reference to Tuberculosis Infection Control: A Practical Manual for Preventing TB).17
Hospital and individual departments should ensure provision of appropriate PPE. Supplies of masks, goggles, and other personal protective equipment may be limited during epidemic conditions, requiring more controlled access to ensure PPE is utilised only in appropriate situations.13 Efforts must also be made to facilitate timely performance of N95 fit testing for at risk staff, as non-fit tested application of N95 may be a contributing factor of transmission in health-care workers.16
Airborne Infection Isolation Operating Theatre
Operations on confirmed cases involving AGP should be performed in an airborne infection isolation room (AIIR). Existing operating theatre may be converted to AIIR after modifying a room’s ventilation to maintain negative pressure and an adequate seal (see Figure 3).17 Architectural design and mechanical elements should meet with local code requirements.17 Regular inspection by engineers is required to maintain the integrity of an isolation theatre.
Clear guidelines on the usage of isolation theatres are necessary, and may include the following:
- Designate an infection control team for development of guidelines, monitoring staff adherence, and revising protocols as the situation is updated
- Set criteria for the use of isolation theatre and workflow on how to initiate
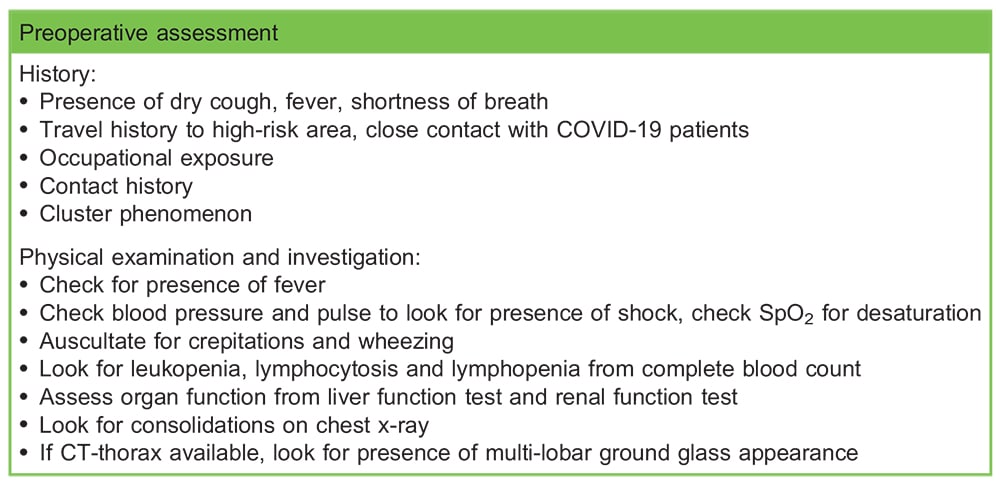
Table 4. Preoperative assessment of patients at risk of COVID-19.
- Dedicate staff to ensuring pressure of the isolation room meets criteria for airborne infection control
- Ensure timely notification of all anaesthesiologists, nurses, assistants, and surgeons involved in the operation
- Specify personal protection equipment required in the theatre
- Specify designated equipment, including disposable ones, for confirmed cases
- Put up signs on the doors to notify staff, and minimise traffic in and out of an isolation room
- Utilise the AIIR for recovery of extubated patients to minimise unnecessary contact with staff or other patients
- Identify/establish protocols for decontamination of the room after a suspected or confirmed case
Patient Transfer
Minimise need for transfer if possible. Surgical mask should be given to patient to reduce droplet transmission. Apply lowest oxygen flow possible to maintain oxygenation to minimise aerosol-generation. Consider early intubation, if patient requires high-flow oxygen for transport.
Health care workers responsible for transfer should employ droplet and contact precaution.18 Depending on the individual risk assessment, if a patient requires high oxygen administration, PPE may be appropriate.
Route from ward to operating theatre should be planned ahead to minimise patient contact with others. In the operation theatre area, avoid transporting patient via a common control or recovery area. If that is not possible, other patients should be partitioned off from the path of the infected patient.
PREOPERATIVE ASSESSMENT
The preoperative assessment aims at identification of high-risk patients and procedures, as well as optimisation of patient’s condition if required.
Identify Suspected COVID-19 Patients
Although suspected and confirmed case should ideally be identified prior to anaesthetic assessment, anaesthesiologists should maintain a high index of suspicion, particularly in clinic setting (see Table 4).
If patient is considered high risk, discuss with surgeons on urgency of operation, and delay if possible. Involve infection control team early in suspected cases. Consider performing rapid test to confirm diagnosis to guide infection control measures if time allows. If diagnosis has been established, coordinate with infection control team for isolation purposes.
Identify High-Risk Procedures
Identify procedures in the operating theatre that are at high risk of aerosol-generation which necessitates airborne precaution.
Surgical procedures that may cause aerosol-generation include rigid bronchoscopy, tracheostomy and surgery involving high- speed drilling (see Table 5). Apart from intubation and extubation, anaesthetic procedures that may cause aerosol-generation include NIV, manual ventilation and awake fibre-optic intubation (see Table 5).
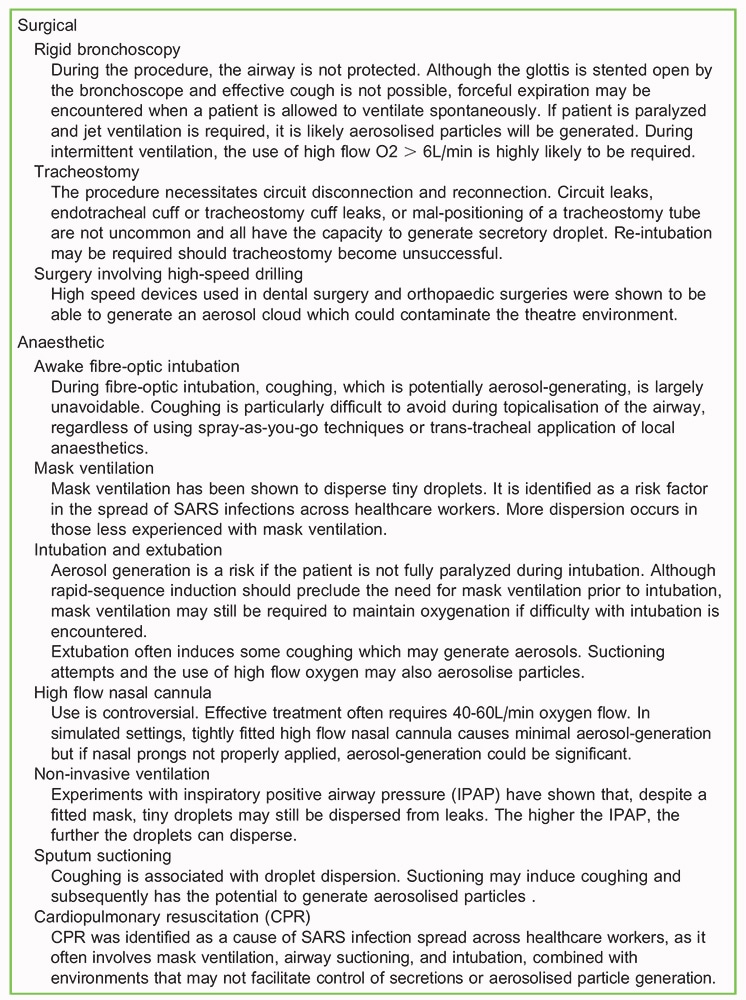
Table 5. List of anaesthetic and surgical procedures that are considered aerosol generating. 16,28,34–36
Optimise Patients Confirmed with COVID-19
For patients who are confirmed to have COVID-19, the preoperative assessment should focus on optimising the patient’s respiratory condition.
- Assess airway meticulously and formulate airway plan
- Determine severity of respiratory compromise. Note oxygen requirements, chest x-ray changes, arterial blood gas
- Look for organ failure, particularly signs of shock, liver failure, renal failure
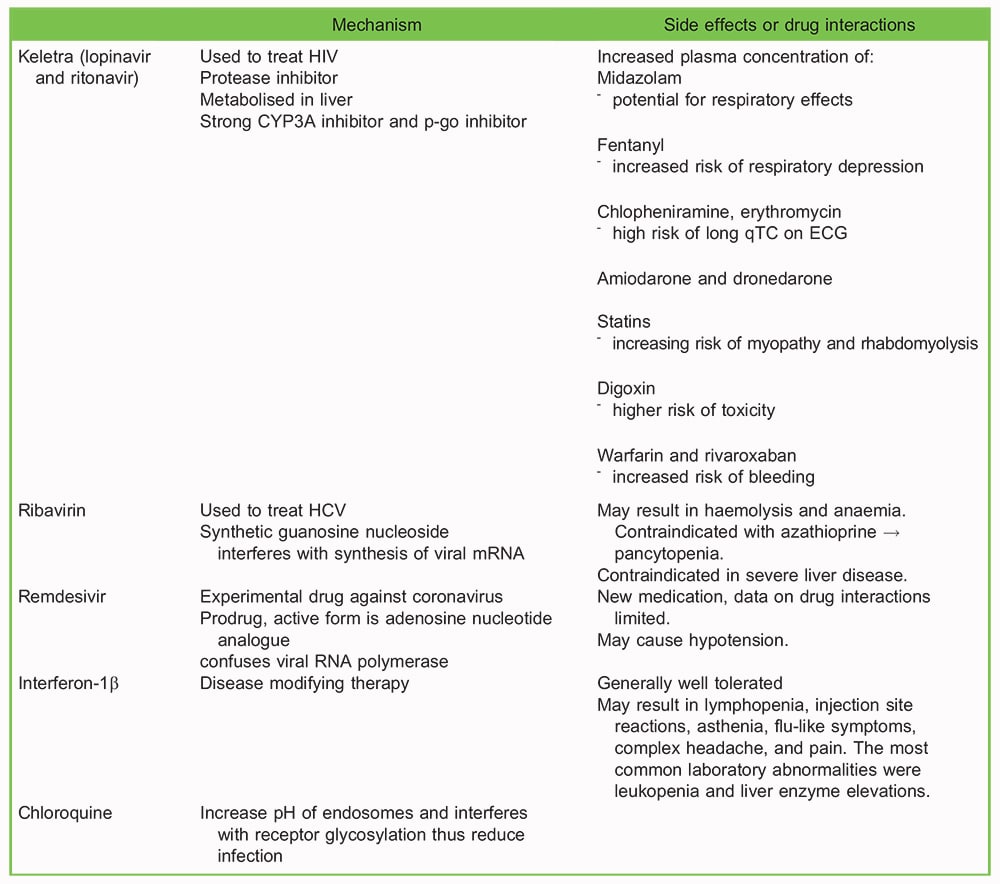
Table 6. Currently used antiviral therapies for COVID-19, and potential side effects or drug-drug interactions. HIV: human immunodeficiency virus. HCV: hepatitis C virus. 6,31–33
- Review current antivirals to avoid drug interactions with anaesthetic medications (see Table 6). Determine post-operative disposition of the patient, including the need for intensive care support
INTRAOPERATIVE MANAGMENT
Modifications of anaesthetic practice will be required in managing patients who are confirmed to have COVID-19.
General Anaesthesia
Modifications are important to minimise aerosol generation and optimise respiratory condition of patients with COVID-19 (see Figure 2).
Before Induction
- Ensure all staffs in theatre are wearing appropriate PPE according to departmental protocol. Integrity of the N95 respirator has to be tested with positive and negative pressure test18
- Reiterate infectious risk of the patient and the level of precautions required to all members in the theatre.
- Communicate clearly with anaesthetic nurse or assistant on airway plan as talking and hearing through N95 respirators and face shields could be difficult.
- Use video laryngoscopes with disposable blades to optimise best first attempt
- Insert bacterial viral filter to the expiratory limb of the breathing circuit apart from the heat and moisture exchanger(HME)19
- Consider disposable covers for surfaces to reduce droplet and contact contamination
Induction
- Minimise number of people in room during induction
- Intubate by experienced practitioner to reduce attempts and time, consider double gloving
- Preoxygenate with minimal gas flow possible i.e. less than 6L per min, ensure good seal with facemask
- Give fentanyl slowly, in small aliquots if required to reduce coughing
- Utilise rapid sequence induction to reduce the need for mask-ventilation
- Maintain airway patency, ensure onset of paralysis before performing intubation, to avoid coughing
- Use two-hand grip to optimise seal if mask-ventilation becomes necessary. Ask for assistance with bagging, while utilising the lowest flows. Give small tidal volumes.
- Start positive pressure ventilation only after the cuff of the endotracheal tube is inflated
- Remove outer gloves after intubation if using the double glove technique to reduce environmental contamination
- Use pre-cut tape to secure endotracheal tube
- Confirm tube position by observing bilateral chest rise or ultrasound, as auscultation may be difficult due to personalprotective equipment.15
- Perform hand hygiene
Maintenance
- Minimise tube and circuit disconnection
- Use a closed-suctioning system if available
- Place the ventilator on standby whenever a circuit disconnection is required, such as tube repositioning. Restart mechanical ventilation only after the circuit has been reconnected/ closed.
- Employ lung protective mechanical ventilation strategies by maintaining tidal volumes of 5-6mL/kg. Increase respiratory rate to maintain minute ventilation, keep peak airway pressure below 30mmHg
Emergence
- Give anti-emetics to minimise vomiting
- Ensure smooth emergence and minimise coughing
- Keep confirmed patient in isolation operating theatre for post-anaesthetic care.
- Arrange case handover with the receiving team in the operating theatre.
- Strict adherence to proper de-gowning at designated location, perform hand hygiene
Regional Anaesthesia
Some researchers cautioned against performing neuraxial anaesthesia, secondary to concerns of the theoretical risk of seeding infection into the central nervous system in viraemic patients. However, there is no evidence to suggest that spinal anaesthesia has resulted in central nervous system involvement in patients with human-immunodeficiency virus (HIV)20 or varicella21. Spinal anaesthesia and epidural blood patches have been performed in obstetric patients with HIV.22 Although the risk of CNS infection is plausible, it should be balanced against the risk of performing general anaesthesia on patients with COVID-19.
Modifications in Regional Procedures
- Use droplet and contact level precautions at the minimum(23), bearing in mind the possibility of converting to general anaesthesia should regional anaesthesia fails. Airborne precautions are necessary if the patient requires high flow oxygen.
- Surgical masks should be worn by the patient throughout the procedure.
- Use a pencil-point spinal needle for spinal anaesthesia. It may reduce the risk of introducing viral material into the CNS, as there is less tissue coring compared with cutting tip spinal needles.21
- Full-length sheaths/covers for ultrasound probes to minimse contamination.24
- Hand hygiene before and after procedure.

Table 7. Effective disinfectants against coronavirus. 37, 38
Obstetric Anaesthesia
Consider early epidural analgesia to minimise need for general ananesthesia in case of emergency caesarean section.25 Insert a hygroscopic filter in the circuit if Entonox is necessary, to prevent the circuit from being contaminated with the virus.25
Consider regional anaesthesia unless contraindicated. There is a higher morbidity risk with general anaesthesia in obstetrics patient and regional anaesthesia is considered safe in COVID-19 patients.26
Temporarily separate the mother from her baby after delivery while diagnostic testing is being performed. Although there is currently no evidence to suggest vertical transmission takes place, transmission after birth via contact with infectious respiratory secretions is possible.27 Involve paediatricians early for caring for neonates born to COVID-19 mothers. Meanwhile insure contact PPE (gown, gloves, facemask and eye protection) for feeding and care.
Modifications on CPR
CPR involves a series of events that increase the risk of aerosol generation, including suctioning, mask ventilation and intubation. Although the risk of disease transmission from chest compressions and defibrillation alone is less certain, any resuscitation attempts should be considered aerosol generating.28
- Consider apnoeic oxygenation instead of providing breaths via bag valve mask to maintain airway patency and ventilation.
- Intubate early in a resuscitation to secure and isolate the airway and possible aerosol generation.
- Hold chest compressions temporarily during intubation to reduce the risk of inhaling infective aerosols by the intubating clinician.29
- Consider utilising chest compression system LUCAS to deliver automated compressions if available. This reduces the number of healthcare workers required in close proximity to the patient.
POSTOPERATIVE MANAGEMENT
To minimise transmission from the patient to health-care workers and other patients, employ the following measures.
- Avoid transferring confirmed cases to the post-anaesthetic care unit.
- Clean and disinfect high-touch surfaces on the anaesthesia machine and anaesthesia work area with an Environmental Protection Agency (EPA)-approved hospital disinfectant(24) (see Table 7).
- Allow time for aerosols in isolation to be washed out, the time required depends on the air changes per hour of the specific location.24
- Consider applying a surgical mask to all other awake and stable patients in the recovery area.
- In the recovery room, distance between patient beds should be at least 1 m. 18, 30
- Avoid giving high flow oxygen, NIV, or nebulised medications. 30
SUMMARY
The COVID-19 is a highly contagious disease, posing a huge burden to the health care system. In providing optimal perioperative care to patients, it is also our duty to protect health care workers and other patients from contracting the disease. In this article, we have outlined perioperative concerns and have suggested methods to overcome potential obstacles. With careful planning and execution of infection control measures, disease transmission can be minimised.
REFERENCES
- World Health Organisation. Coronavirus disease (COVID-2019) situation Report – 54 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 16/03/2020)
- Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA. 2020.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet. 2020;395(10223):497-506.
- Yeo C, Kaushal S, Yeo D. Enteric involvement of coronaviruses: is faecal-oral transmission of SARS-CoV-2 possible? The Lancet Gastroenterology & Hepatology.
- Peeri NC, Shrestha N, Rahman MS, Zaki R, Tan Z, Bibi S, et al. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: what lessons have we learned? International Journal of Epidemiology. 2020.
- Wang Y, Wang Y, Chen Y, Qin Q. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. Journal of Medical Virology.n/a(n/a)
- Backer JA, Klinkenberg D, Wallinga J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Eurosurveillance. 2020;25(5):2000062.
- World Health Organisation. Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected Interim guidance 2020. https://www.who.int/publications-detail/clinical-management-of-severe- acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected (accessed on 16/03/2020).
- Nick W, Amanda K, Lucy Telfar B, Michael GB. Case-Fatality Risk Estimates for COVID-19 Calculated by Using a Lag Time for Fatality. Emerging Infectious Disease journal. 2020;26(6).
- Ng M-Y, Lee EY, Yang J, Yang F, Li X, Wang H, et al. Imaging Profile of the COVID-19 Infection: Radiologic Findings and Literature Review. Radiology: Cardiothoracic Imaging. 2020;2(1):e200034.
- World Health Organisation. Coronavirus disease (COVID-19) technical guidance: Laboratory testing for 2019-nCoV in humans. 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/laboratory-guid ance (accessed on 09/03/2020)
- Centers for Disease Control and Prevention. Interim Guidance for discontiuation of transmission-based precautions and disposition of hospitalised patient with COVID-19 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/disposition-hos pitalised-patients.html (accessed on 26/02/2020)
- Centers for Disease Control and Prevention. What healthcare personnel should know about caring for patients with confirmed or possible 2019-nCoV infection: Centers for Disease Control and Prevention 2020 https://www.cdc.gov/ coronavirus/2019-ncov/hcp/caring-for-patients.html (accessed on 16/02/2020)
- World Health Organisation. Infection prevention and control during health care when novel coronavirus(nCoV) infection is suspected Interim guidance 25 January 2020 Geneva2020 https://www.who.int/publications-detail/infection-prevention- and-control-during-health-care-when-novel-coronavirus-(ncov)-infection-is-suspected-20200125 (accessed on 17/02/ 2020)
- Wax RS, Christian MD. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus
(2019-nCoV) patients. Canadian Journal of Anesthesia/Journal canadien d’anesthésie. 2020. - Christian MD, Loutfy M, McDonald LC, Martinez KF, Ofner M, Wong T, et al. Possible SARS coronavirus transmission during cardiopulmonary resuscitation. Emerg Infect Dis. 2004;10(2):287-93.
- University of California San Francisco. Tuberculosis Infection Control: A Practical Manual for Preventing TB. https://www. currytbcenter.ucsf.edu/products/tuberculosis-infection-control-practical-manual-preventing-tb (accessed on17/02/2020)
- World Health Organisation. Epidemic-prone & pandemic-prone acute respiratory disease infection prevention & control in health-care facilities summary guidance 2007. https://www.who.int/csr/resources/publications/WHO_CDS_EPR_2007_8/ en/ (accessed on 16/02/2020)
- Wilkes AR. Heat and moisture exchangers and breathing system filters: their use in anaesthesia and intensive care. Part 1 – history, principles and efficiency. Anaesthesia. 2011;66(1):31-9.
- Hughes SC, Dailey PA, Landers D, Dattel BJ, Crombleholme WR, Johnson JL. Parturients Infected with Human Immunodeficiency Virus and Regional Anesthesia : Clinical and Immunologic Response. Anesthesiology: The Journal of the American Society of Anesthesiologists. 1995;82(1):32-7.
- Brown NW, Parsons APR, Kam PCA. Anaesthetic considerations in a parturient with varicella presenting for Caesarean section. Anaesthesia. 2003;58(11):1092-5.
- Tom Dari J, M.D., Gulevich Steven J, M.D., Shapiro Harvey M, M.D., Heaton Robert K, Ph.D., Grant I, M.D. Epidural Blood Patch in the HIV-positive Patient Review of Clinical Experience. Anesthesiology: The Journal of the American Society of Anesthesiologists. 1992;76(6):943-7.
- World Federation of Societies of Anaesthesiologists. Coronavirus – guidance for anaesthesia and perioperative care providers 2020. https://resources.wfsahq.org/latest-news/latestnews/943-coronavirus-staying-safe (accessed on 3/3/2020)
- American Society of Anesthesiologists. Coronavirus (2019-nCoV) Information for Health Care Professionals Recommendations 2020. https://www.asahq.org/about-asa/governance-and-committees/asa-committees/committee-on- occupational-health/coronavirus (accessed on 3/3/2020)
- Obstetric Anaesthetists’ Association. Management of pregnant women with known or suspected COVID-19 2020. https:// icmanaesthesiacovid-19.org/obstetric-anaesthesia (accessed on 19/03/2020)
- Xia H, Zhao S, Wu Z, Luo H, Zhou C, Chen X. Emergency Caesarean delivery in a patient with confirmed coronavirus disease 2019 under spinal anaesthesia. British Journal of Anaesthesia.
- Centers for Disease Control and Prevention. Interim considerations for infection prevention and control of coronavirus disease 2019 (COVID-19) in inpatient obstetric healthcare settings 2020. https://www.cdc.gov/coronavirus/2019-ncov/ hcp/inpatient-obstetric-healthcare-guidance.html (accessed on 25/02/2020)
- Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol Generating Procedures and Risk of Transmission of Acute Respiratory Infections to Healthcare Workers: A Systematic Review. PLOS ONE. 2012;7(4):e35797
- Peng PWH, Ho P-L, Hota SS. Outbreak of a new coronavirus: what anaesthetists should know. British Journal of Anaesthesia.
- Tan TK. How Severe Acute Respiratory Syndrome (SARS) Affected the Department of Anaesthesia at Singapore General Hospital. Anaesthesia and Intensive Care. 2004;32(3):394-400.
- Marziniak M, Meuth S. Current Perspectives on Interferon Beta-1b for the Treatment of Multiple Sclerosis. Advances in Therapy. 2014;31(9):915-31.
- Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Research. 2020;30(3):269-71.
- Fombon FN, Thompson JP. Anaesthesia for the adult patient with rheumatoid arthritis. Continuing Education in Anaesthesia Critical Care & Pain. 2006;6(6):235-9.
- Chan MTV, Chow BK, Lo T, Ko FW, Ng SS, Gin T, et al. Exhaled air dispersion during bag-mask ventilation and sputum suctioning – Implications for infection control. Scientific Reports. 2018;8(1):198.
- Hui DS, Chow BK, Lo T, Tsang OTY, Ko FW, Ng SS, et al. Exhaled air dispersion during high flow nasal cannula therapy versus CPAP via different masks. European Respiratory Journal. 2019:1802339.
- Hui DS, Hall SD, Chan MTV, Chow BK, Tsou JY, Joynt GM, et al. Noninvasive Positive-Pressure Ventilation: An Experimental Model to Assess Air and Particle Dispersion. CHEST. 2006;130(3):730-40.
- Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. Journal of Hospital Infection. 2020;104(3):246-51.
- United States Environmental Protection Agency. Disinfectants for Use Against SARS-CoV-2 2020. https://www.epa.gov/ pesticide-registration/list-n-disinfectants-use-against-sars-cov-2 (accessed on 16/03/2020)
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/