General Topics

KEY POINTS
- Perioperative stroke has been recently defined as a cerebrovascular accident occurring up to 30 days after surgery.
- A substantial proportion is covert in presentation, commonly manifesting as postoperative cognitive dysfunction or delirium. Health care workers’ awareness of perioperative stroke can be improved.
- The risk of recurrent stroke is highest within the first 3 months and stabilizing by 9 months, but it remains elevated compared with patients without prior stroke history. Elective surgeries should be postponed for at least 9 months following perioperative stroke.
- Risk factors are being identified that will help in the development of a scoring system to predict risk of perioperative stroke.
- Prehabilitation might offer some protection for perioperative stroke, but evidence is pending.
- Perioperative stroke in general carries a poorer prognosis than nonoperative stroke does. Intra-arterial thrombectomy is a promising option for treatment of perioperative stroke.
INTRODUCTION
Perioperative stroke is defined as a brain infarction of ischaemic or haemorrhagic aetiology that occurs during surgery or within 30 days after surgery.1 It is a distinct entity from nonperioperative stroke owing to differences in clinical presentations and prognoses. It not only complicates the course of surgical recovery but also may carry up to 8 times the mortality of nonperioperative stroke, according to previous studies.2 This figure has probably been underestimated, as most perioperative strokes are covert, manifesting as postoperative cognitive decline and sometimes complicated by delirium.3 Despite the increased awareness and research done in this area, incidence is still accumulating.4 In thisarticle, we will review the special characteristics of this challenging disease entity including its pathophysiology, aetiology, risk stratification, diagnosis and treatment options.
CHARACTERISTICS OF PERIOPERATIVE STROKE
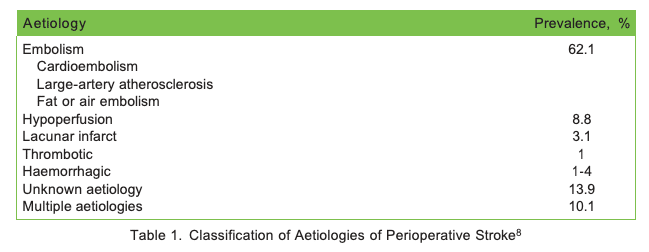
According to an article published by the New England Journal of Medicine,5 the mean global lifetime risk of all forms of stroke increased from 22.8% in 1990 to 24.9% in 2016. The risk of perioperative stroke varies largely depending on the type of surgery, with an incidence of 0.1% to 1.9% in noncardiovascular, nonneurologic and minor vascular surgery. Fifty percent of cases occur within the first postoperative day6 and are mainly ischaemic in nature,6 which is the same as observed in nonperioperative settings.1 Anterior cerebral circulation is also the most affected location in both perioperative and nonperioperative strokes.7 After the primary ischaemic insult to the brain, secondary brain damage can set in as common perioperative physiological derangements arise, such as hypotension, hypocapnia or hypercapnia.1 The aetiologies of perioperative strokes are summarized in Table 1.
A recent study noted that about 7% of perioperative strokes remain unrecognized, as defined by an acute brain infarct detected on magnetic resonance imaging (MRI) of the brain after noncardiac surgery in a patient with no clinical stroke symptoms.3 Perioperative covert stroke has been shown to be associated with doubling of the risk of delirium from 5% to 10% (P = 0.02) and an increase of cognitive decline at 1 year from 29% to 42% (P = 0.006).3
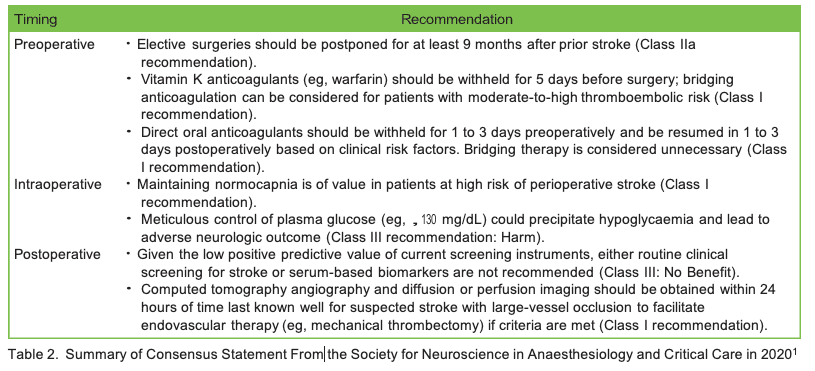
There is also great heterogeneity in research evidence and clinical recommendations due to varying case presentations, diagnostic criteria, treatment modalities and prognoses. A Consensus Statement from the Society for Neuroscience in Anaesthesiology and Critical Care in 2020 provides a comprehensive overview, addressing and clarifying the clinical management of surgical patients at high risk for perioperative stroke,with a summary of the recommendations listed in Table 2.1
RISK STRATIFICATION AND PATIENT CONSENT
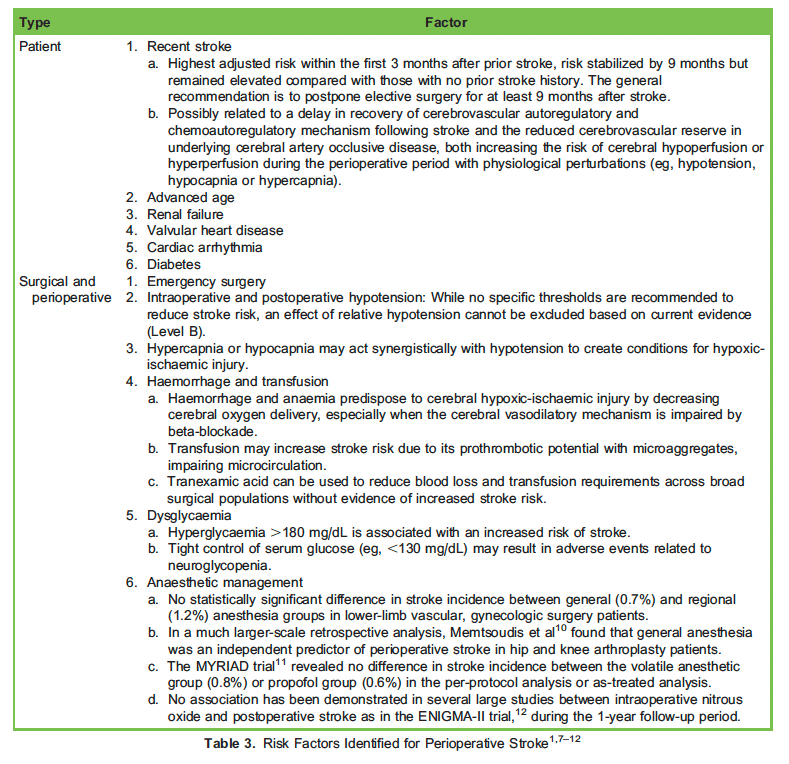
A recent history of stroke (within 3 months of surgery) is the most significant risk factor for perioperative stroke. Current recommendations are to postpone elective operations for at least 9 months after previous stroke to achieve full recovery of cerebral autoregulation. Other risk factors consistently identified for perioperative stroke are included in Table 3.
The Myocardial Infarction or Cardiac Arrest risk score and the American College of Surgeons Surgical Risk Calculator are the most discriminatory for perioperative stroke.8 However, further work is still required to determine the optimal sensitivity and specificity thresholds before they can be effectively incorporated into daily practice.
According to a survey by Canadian anaesthesiologists, less than 50% of respondents routinely discuss perioperative stroke with high-risk patients. In addition, less than 50% correctly identified stroke incidence, aetiology and mortality rates.1 The lack of standardized risk assessment and insufficient awareness regarding perioperative stroke contributes to the incomplete risk discussion and informed consent.
PERIOPERATIVE MONITORING
Potential assessment tools to detect perioperative cerebrovascular disease include but are not limited to the following:
- transcranial Doppler (to visualise micro-embolism)
- electroencephalography (to identify a distinct wave pattern, eg, oscillatory asymmetry and increased delta/alpha ratios associated with cerebral ischaemia)
- cerebral oximetry (to continuously record the change in cerebral tissue oxygenation)
However, their utility in predicting or detecting cerebral ischaemia has not been defined in the setting of noncardiac, minor vascular or nonneurologic surgeries.
POTENTIAL ROLE OF PREHABILITATION IN PREVENTION OF PERIOPERATIVE STROKE
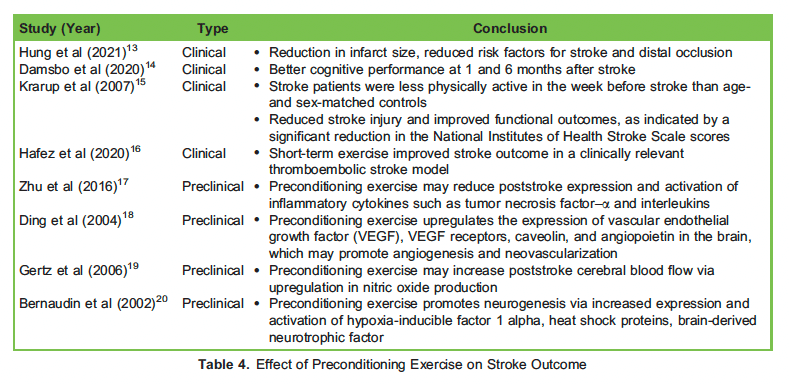
Ischaemic preconditioning involves short durations of ischaemia that protect the brain against longer and more lethal complications. Observational studies show that regular physical exercises of moderate to high intensity reduce the risk and severity of stroke and improve outcomes and recovery after stroke. However, the applicability to perioperative settings has not yet been researched. These findings may provide hope for neuroprotection involving ‘‘exercise mimetics.’’ For example, metformin, as an 5/ adenosine monophosphate-activated protein kinase (AMPK) activator, may induce nitric oxide synthase 3. The use of vascular endothelial growth factor (VEGF) analogues and VEGF receptor agonists may promote cerebral angiogenesis. Table 4 summarizes some studies comparing physical activity level and incidence and severity of stroke with hypothesized biochemical mechanisms.21
POSTOPERATIVE DIAGNOSIS
Recognition and diagnosis of perioperative stroke poses a great challenge to clinicians due to the interaction of residual anaesthetics and postoperative delirium, which is commonly observed in the elderly population, who are also identified as high risk of suffering from perioperative stroke.1 Therefore, the anaesthetic technique should be individualized to allow early neurologic assessment in the high-risk group, for example, with the use of ultra-short-acting agents where possible. Delayed emergence, altered mental status, and/or the presence of new focal neurologic deficits in the absence of convincing causes should raise the suspicion for stroke. Ideally, clinical diagnostic tools that are sensitive, specific, and reproducible should be used to detect perioperative stroke. They should also be handy to use and widely available. The National Institute of Health Stroke Scale score has been trialled before but found to have low specificity.1 The diagnosis of overt stroke largely depends on neuroimaging, namely, computed tomography of the brain and cerebral arteries. Biochemical screening methods are not currently convincing.1
In covert stroke, brain MRI is required to detect silent infarction. However, the decision of proceeding to MRI scan is subjected to availability of resources, level of suspicion of clinicians, and the complications that arises from ‘‘clinically significant’’ covert stroke (most notably being delirium or cognitive decline). This knowledge gap needs to be further explored, as the identification of such cases is crucial for secondary prevention purposes. The serum neurofilament light level has been shown to be closely associated with imaging and clinicalfeatures of small-vessel disease. This might complement MRI markers in assessing small- vessel disease in covert stroke.22
ROUTINE COGNITIVE TESTING AND TRAINING
The association between postoperative cognitive decline and perioperative stroke makes a strong argument for introducing mandatory training inperioperative cognitive assessment. This could be conducted by perioperative physicians to see whether it can reduce the incidence and sequelae of perioperative stroke. Perioperative cognitive assessment may also alert clinicians so that they exercise a higher index of suspicion for patients at risk. The implementation of routine perioperative cognitive testing such as the Montreal cognitive assessment, as part of ‘‘vital sign assessment,’’ is one example.
TREATMENT OPTIONS AND PROGNOSIS
Treating perioperative stroke is challenging. This is not only because of delayed diagnosis but also because of competing therapeutic challenges involved with co-managing surgical site bleeding. In-patient stroke may theoretically allow earlier diagnosis and a higher likelihood of receiving timely reperfusion treatment. However, there is no current evidence of improved outcome after early postoperative reperfusion; rather, there are associations with increased mortality and increased length of hospital stay. Prognosis following perioperative stroke-related interventions is worse (mechanical thrombectomy [MT] and intravenous tissue plasminogen activator) than in the outpatient stroke setting.23
According to 2019 Update to the American Heart Association/American Stroke Association (AHA/ASA) 2018 Guidelines for the Early Management of Acute Ischaemic Stroke, intravenous thrombolysis should be administered when a strong clinical suspicion of ischaemic stroke exists, in the absence of contraindications to therapy. These contraindications, however, are often found in postoperative period. It should be noted that recent surgery (within 14 days) is considered a relative contraindication.24
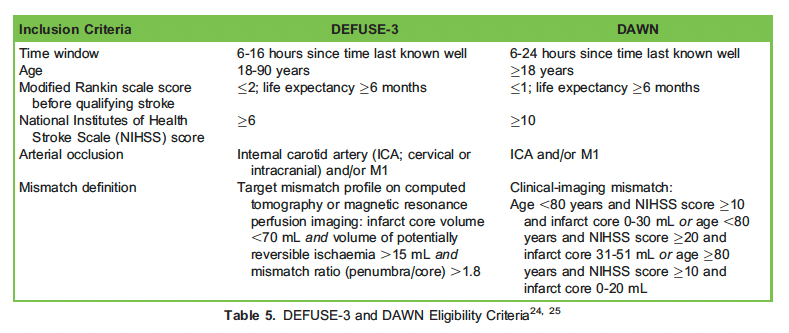
Fortunately, the recent development of endovascular thrombectomy allows revascularization of large-vessel occlusion with a number needed to treat (NNT) of 2.6.25 This is a milestone in management of all forms of ischaemic stroke, and hopefully similar success can be shown with perioperative stroke. MT has been traditionally restricted, as there is a 6-hour treatment window since the suspected time of stroke for it to beeffective. In the latest recommendation from AHA/ASA, extended-window MT should be recommended or reasonable for up to 16 or 24 hours if DEFUSE-3 or DAWN eligibility criteria are met, respectively.24 In a meta-analysis, MT was a strong outcome modifier, reducing the odds ofunfavourable outcome by a factor of 5 for patients with acute ischaemic stroke associated with large ischaemic core at presentation (odds ratio, 0.19). MT is consistently associated with a decreased odds for mortality (odds ratio, 0.60) but does not appear to influence incidence of secondary intracranial haemorrhage.25,26
Hence, focused assessment of large-vessel disease would be useful in high-risk groups if neurologic deficits are present. The availability of endovascular thrombectomy warrants further research to clarify the best approach to provide early identification of suitable patients. However,aggressive early intervention after perioperative stroke presents a challenge. This is because of its covert nature, delays in diagnosis, andcompeting goals of care that can be at odds with dangers of postoperative bleeding.
This would explain in part the higher rates of death and disability observed compared with nonperioperative stroke. Supportive care and functional rehabilitation remain the mainstay of management to minimize the effect brought about by perioperative stroke. Management of perioperative stroke from prevention through to diagnosis and treatment requires a multidisciplinary team with expertise in neurology, nursing, anaesthesia and interventional radiology. There is still a lot of work to do to improve overall care and treatment for this challenging group of patients.
SUMMARY
Perioperative stroke should not be perceived as identical to nonperioperative stroke for its unique aetiology, perplexing presentation andrelatively poor prognosis. It is no longer as rare as commonly thought given the emerging evidence of ‘‘covert’’ stroke. The development of endovascular MT has announced a breakthrough in the management of this difficult disease entity and should be considered particularly in patients with large-vessel thromboembolic occlusion as soon after stroke symptoms are confirmed. Nonetheless, detecting neurologic deficits in a postoperative setting is difficult especially when this complication is not suspected by anaesthetic providers, delaying the opportunity to ‘‘save the brain’’ in a timely manner. Currently, accurate and meticulous preoperative risk factor identification, strong suspicionin the early postoperative period together with focused postoperative monitoring still serve as the mainstay of management. Anaesthesiologists should play a critical role along this perioperative journey.
REFERENCES
- Vlisides PE, Moore LE, Whalin MK, et al. Perioperative care of patients at high risk for stroke during or after non-cardiac, non-neurological surgery: 2020 guidelines from the Society for Neuroscience in Anaesthesiology and Critical Care. J Neurosurg Anaesthesiol. 2020;32(3):210-226.
- Mashour GA, Shanks AM, Kheterpal S. Perioperative stroke and associated mortality after non-cardiac, non-neurologic surgery. Anaesthesiology. 2011;114(6):1289-1296.
- The NeuroVISION Investigators. Perioperative covert stroke in patients undergoing non-cardiac surgery: a prospective cohort study. Lancet. 2019;394(1003):1022-1029.
- Smilowitz NR, Gupta N, Ramakrishna H, et al. Perioperative major adverse cardiovascular and cerebrovascular events associated with non-cardiac surgery. JAMA Cardiol. 2017;2(2):181-187.
- GBD 2016 Lifetime Risk of Stroke Collaborators. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N Engl J Med. 2018;379:2429-2437.
- Al-Hader R, Al-Robaidi K, Jovin T, et The incidence of perioperative stroke: estimate using state and national databases and systematic review. J Stroke. 2019;21(3):290-301.
- Dong Y, Cao W, Cheng X, et al. Risk factors and stroke characteristic in patients with postoperative strokes. J Stroke Cerebrovasc Dis. 2017;26(7):1635-1640.
- Wilcox T, Smilowitz NR, Xia Y, et Cardiovascular risk scores to predict perioperative stroke in noncardiac surgery.Stroke. 2019;50:2002-2006.
- Jorgensen ME, Torp-Pedersen C, Gislason GH, et al. Time elapsed after ischaemic stroke and risk of adverse cardiovascular events and mortality following elective noncardiac surgery. JAMA. 2014;312(3):269-277.
- Memtsoudis SG, Sun X, Chiu YL, et al. Perioperative comparative effectiveness of anesthetic technique in orthopedic patients. Anesthesiology. 2013;118:1046-1058.
- Landoni G, Lomivorotov VV, NigroC Neto, et al. Volatile anesthetics versus total intravenous anesthesia for cardiac surgery. N Engl J Med. 2019;380:1214-1225.
- Leslie K, Myles PS, Kasza J, et Nitrous oxide and serious longterm morbidity and mortality in the evaluation of nitrous oxide in the gas mixture for anaesthesia (ENIGMA)-II trial. Anesthesiology. 2015;123:1267-1280.
- Hung SH, Ebaid D, Kramer S, Werden E, Baxter H, Campbell BC, et Pre-stroke physical activity and admission stroke severity: a systematic review. Int J Stroke 2021 Feb 23 [Epub]. https://doi.org/10.1177/1747493021995271.
- Damsbo AG, Mortensen JK, Kraglund KL, Johnsen SP, A en G, Blauenfeldt Prestroke physical activity and poststroke cognitive performance. Cerebrovasc Dis 2020;49:632-638.
- Krarup LH, Truelsen T, Pedersen A, Lerke H, Lindahl M, Hansen L, et Level of physical activity in the week preceding an ischemic stroke. Cerebrovasc Dis 2007;24:296-300.
- Hafez S, Khan MB, Awad ME, Wagner JD, Hess DC. Short-term acute exercise preconditioning reduces neurovascular injury after stroke through induced eNOS activation. Transl Stroke Res 2020;11:851-860.
- Zhu L, Ye T, Tang Q, Wang Y, Wu X, Li H, et al. Exercise p ditioning regulates the toll-like receptor 4/nuclear factor- j B signaling pathway and reduces cerebral ischemia/reperfusion inflammatory injury: a study in rats. J Stroke Cerebrovasc Dis 2016;25:2770-2779.
- Ding YH, Luan XD, Li J, Rafols JA, Guthinkonda M, Diaz FG, et Exercise-induced overexpression of angiogenic factors and reduction of ischemia/reperfusion injury in stroke. Curr Neurovasc Res 2004;1:411-420.
- Gertz K, Priller J, Kronenberg G, Fink KB, Winter B, Schro¨ck H, et Physical activity improves long-term stroke outcome via endothelial nitric oxide synthase-dependent augmentation of neovascularization and cerebral blood flow. Circ Res 2006;99:1132-1140.
- Bernaudin M, Nedelec AS, Divoux D, MacKenzie ET, Petit E, Schumann-Bard Normobaric hypoxia induces tolerance to focal permanentcerebral ischemia in association with an increased expression of hypoxia-inducible factor-1 and its target genes, erythropoietin and VEGF, in the adult mouse brain. J Cereb Blood Flow Metab 2002;22:393-403.
- Hafez S, Eid Z, Alabasi S, et al. Mechanisms of preconditioning exercise-induced neurovascular protection in stroke. J Stroke. 2021;23(3):312-326.
- Duering M, Mark JK, Steffen T, et Serum neurofilament light chain levels are related to small vessel disease burden. J Stroke. 2018;20(2):228-238.
- Bekelis K, Missios S, Coy S, et Comparison of outcomes of patients with inpatient or outpatient onset ischaemic stroke.J Neurointerventional Surg. 2016;8:1221-1225.
- Powers WJ, Rabinstein AA, Ackerson T, et 2018 guidelines for the early management of patients with acute ischaemic stroke: aguideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50:e344-e418.
- Griessenauer CJ, Medin C, Maingard J, et al. Mechanical thrombectomy in patients with a large ischaemic volume at presentation: systematic review and meta-analysis. World Neurosurg. 2018;2:263-269.
- Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta- analysis of individual patient data from five randomised trials. Lancet. 2016;387:1723-1731.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/