Regional Anaesthesia

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- TRUE or FALSE: On injection of local anaesthetic
- It safe to inject the full dose of local anaesthetic in ONE go
- Aspiration should reveal no blood
- It is usual for the patient to complain of pain
- The spread of anaesthetic MUST be seen on the screen when using ultrasound
- Which of the following statements is correct?
- Intravenous access is not needed when performing a peripheral nerve block
- Knowledge of anatomy is not needed if you use an ultrasound machine
- Confusion and peri-oral numbness are early signs of local anaesthetic toxicity
- Insulated needles are used to prevent electric shock to the anaesthetist
- What is the
- Maximum recommended safe dose of bupivacaine in mg/kg?
- Minimum advised monitoring required for performing regional anaesthesia?
- Correct treatment for suspected LA toxicity?
- Name of a long acting local anaesthetic?
INTRODUCTION
Peripheral nerve blocks (PNB) are an established and effective method for providing post-operative analgesia. They can also be used as the sole anaesthetic technique for some operations. A successful nerve block results from placing the right drug in the right place. A peripheral nerve block can be achieved as a result of placing local anaesthetic next to a nerve eg the femoral nerve, next to a plexus eg the brachial plexus or into a compartment containing peripheral nerves eg tranversus abdominis plane block.
This tutorial is aimed at informing you of the basic requirements for performing any peripheral nerve block. You need to have prepared your patient, your environment, your equipment and yourself. Prior to attempting any peripheral nerve block it is important to “prepare yourself”. You must have a sound knowledge of the relevant anatomy, techniques for performing the block and an awareness of any potential complications is required. Specific blocks and their potential problems will be covered as part of ATOTW regional anaesthesia series.
PATIENT
During your pre-operative assessment (Figure 1) you will have determined if there is a suitable peripheral nerve block that would benefit the patient for their operation and that the patient has no contraindications to this particular block. Consent must be obtained and the patient appropriately prepared.

Figure 1. Patient being pre-assessed
Consent
Informed consent must be obtained from the patient before performing a peripheral nerve block. This must include explaining the procedure, its benefits, the alternatives, any side-effects and any potential complications such as nerve damage. This discussion should be documented in the notes. You should also discuss and document a “plan B” should the block fail.

Table 1. Potential complications of peripheral nerve blocks
Patient Preparation
Even if there is a plan to keep the patient awake, the patient must be adequately starved because the need for general anaesthesia may arise, e.g. block failure or the onset of local anaesthetic toxicity. Minimum monitoring as advised by the Association of Anaesthetists Great Britain and Ireland (AAGBI 2007a) (electrocardiogram, pulse oximetry, non-invasive blood pressure) must be established and intra-venous access obtained prior to commencing a block. The patient needs to be positioned appropriately for the block with the correct side confirmed.
ENVIRONMENT
General
An appropriately trained assistant who is familiar with the block is essential. Full resuscitation equipment must be available and the specialist equipment for the block assembled. Access to intralipid is recommended so it can be used should local anaesthetic toxicity occur (Table 2).
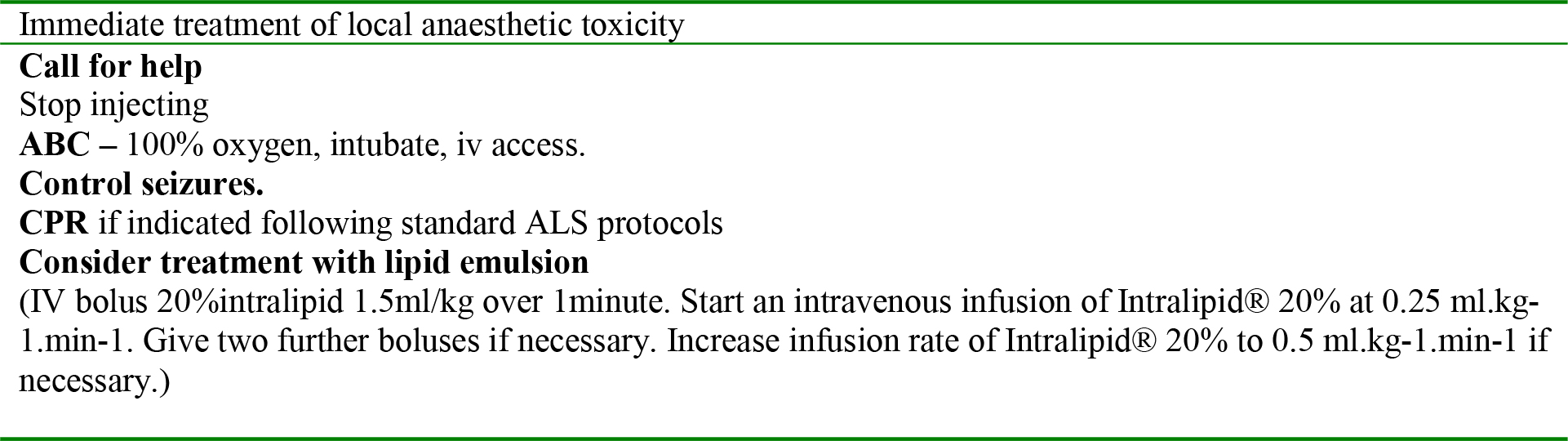
Table 2. Immediate treatment of local anaesthetic toxicity – Summary of AAGBI recommendations
Infection Control
Sterile gloves and antiseptic cleaning solution should be used for a single dose block (AAGBI 2002). Full asepsis (thorough hand washing, sterile gloves and gown, a hat, face mask and sterile drapes applied after skin preparation) (Fig 2), should be used if a catheter is being introduced.

Figure 2. Full asepsis requires hat, facemask, gown and sterile gloves.
Specialist Equipment
The equipment required for the block will need to be assembled and you should have familiarized yourself with it. Historically paraesthesia was championed for locating nerves accurately and there are some regional anaesthetists who still use this method. However the development of well designed peripheral nerve stimulators (Figure 3), and more recently ultrasound machines (Figure 4), provide a more reliable method for nerve location. These should be used where possible.

Figure 3. Three peripheral ultrasound machine

Figure 4. A micromax nerve stimulators
Special insulated needles are required when performing a peripheral nerve block with a peripheral nerve stimulator. They have a special insulating coating along the length of the needle except for the needle tip, so that current only passes to the tip. Therefore a muscle contraction resulting from stimulation of the nerve means that the needle tip is very near to the nerve. (More detail about peripheral nerve stimulators and insulated needles will follow in the next regional anaesthesia tutorial). This type of needle is also often used during ultrasound guided peripheral nerve blocks because it has a separate injection port which will allow your assistant to inject local anaesthetic without disturbing the needle’s position. No specific needle has yet been proven easier to see under ultrasound.
Drugs
Local anaesthetics which can be used for peripheral nerve blockade are lidocaine, lidocaine with adrenaline (epinephrine), bupivacaine, levo-bupivacaine, prilocaine and ropivacaine.
The indication for the PNB will influence your choice of local anaesthetic, you will need to consider:
- Onset – A rapid onset may be more convenient when using PNB as a sole anaesthetic technique. Lidocaine and ropivacaine have relatively fast onset times (10-30minutes) depending on which nerves they are used to block.
- Duration – If significant pain is expected, then maximum benefit from your PNB will be achieved if you choose a longer acting local anaesthetic such as bupivacaine, levobupivacaine or ropivacaine. The duration of a PNB will depend on the site of the block and the amount of drug used. You must make sure you keep within the safe recommended dose of local anaesthetic based on your patient’s weight (Table 3).
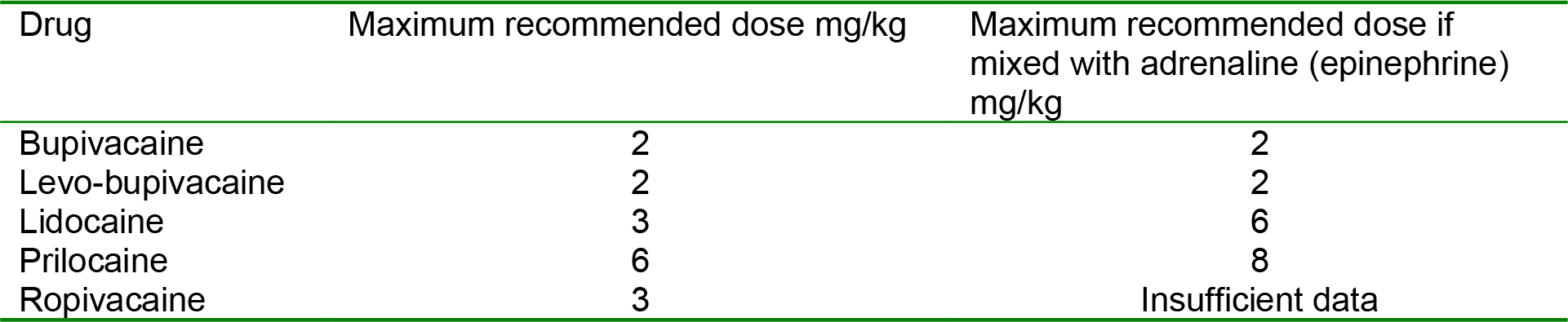
Table 3. Maximum recommended dose of local anaesthetics
TECHNIQUE
In order to establish blockade of a peripheral nerve, local anaesthetic solution must be placed as close as possible to the nerve but not in the nerve. It is therefore imperative if you wish to perform peripheral nerve blocks that you know the relevant anatomy for each block you wish to perform. Using ultrasound guidance does not remove this requirement in fact you may need to know the anatomy in greater detail to identify all the visualised structures.
It is important to perform a “safe injection”. This should be in small increments of up to a maximum of 5mls at a time. Aspiration should always precede injection to confirm your needle tip is NOT in a blood vessel. It should be easy and painless to inject, if not your needle tip may be IN the nerve. If using a PNS, appropriate muscle twitches should stop immediately on starting the injection. If twitches continue this suggests your needle tip may be IN the nerve. If you are using ultrasound local anaesthetic MUST be seen spreading around the nerve to exclude intraneural or intravascular injection and ensure correct placement. If in doubt, STOP and if necessary start from the beginning again or abandon the procedure. Be aware of signs of local anaesthetic toxicity (Table 5) and know how to treat them (Table 2).
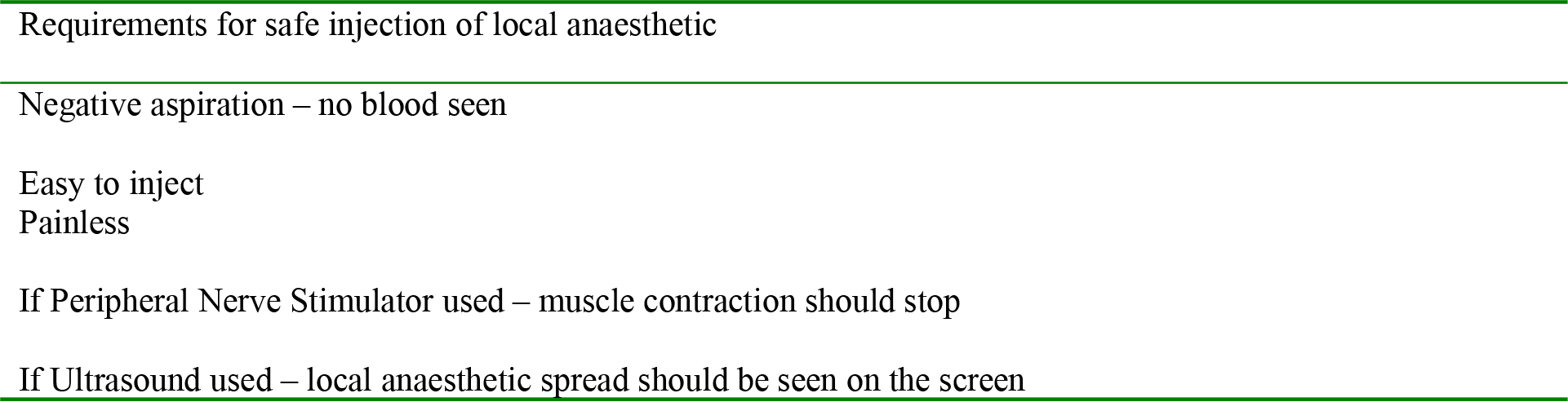
Table 4. Guide to safe injection of local anaesthetic.
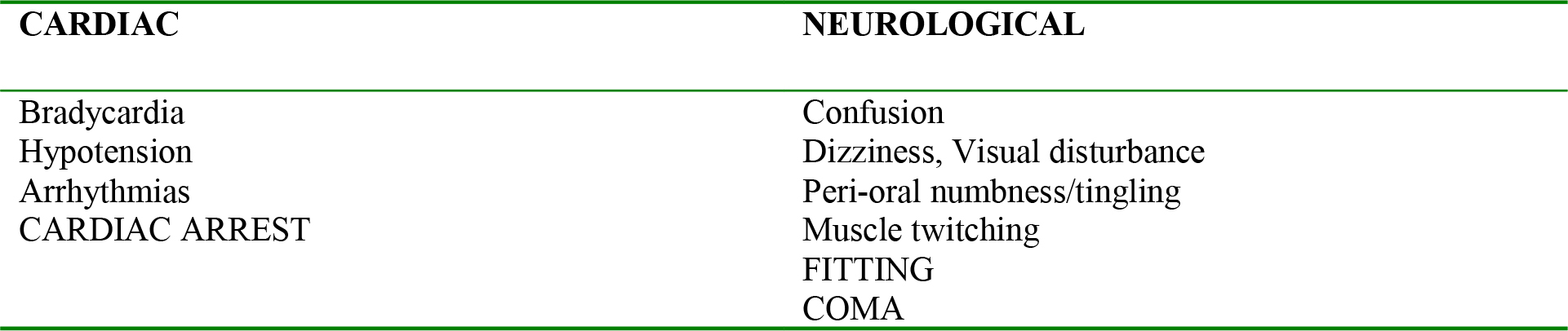
Table 5. Signs and symptoms of local anaesthetic toxicity
REMEMBER
- Prepare your patient, equipment and environment Safe dose of local anaesthetic
- Safe dose of local anaesthetic
- Safe injection – negative aspiration, painless, LA spread seen on ultrasound.
SUMMARY
- PNBs performed properly are safe and effective
- Know your anatomy and technique
- Suitable setting – assistant, equipment, resuscitation facilities
- Prepared patient – informed consent, monitoring, I.V. access, position
- SAFE technique. If in doubt, STOP!
ANSWERS TO QUESTIONS
-
- FALSE Local anaesthetic should be injected slowly at a maximum of 5mls at a time.
- TRUE It essential to have a negative aspiration to ensure you are not in a blood vessel.
- FALSE Injection of local anaesthetic should be painless otherwise it suggests you may be intraneural.
- TRUE
-
- FALSE You must secure iv access prior to performing a peripheral nerve block.
- FALSE A sound knowledge of anatomy is needed for safe and successful performance of PNB.
- TRUE
- FALSE Peripheral nerve block needles are insulated along their shaft to focus the impulse to the tip.
-
- The maximum recommended safe dose of bupivacaine is 2mg/kg. (See Table 3)
- The minimum monitoring required for performing regional anaesthesia advised by the AAGBI is electrocardiogram, pulse oximetry and non-invasive blood pressure
- ABC, CPR if appropriate and consider intralipid. See Table 2 or AAGBI website for full guidelines
- Bupivacaine, levobupivacaine and ropivacaine have a long duration of action.
WEBLINKS, REFERENCES and FURTHER READING
- www.ragbi.org
- www.nysora.com
- http://www.aagbi.org/publications/guidelines.htm#m
- http://www.rcoa.ac.uk/index.asp?PageID=1209
- Association of Anaesthetists Great Britain & Ireland (AAGBI) 2002 Infection Control in Anaesthesia London, AAGBI
- Association of Anaesthetists Great Britain & Ireland (AAGBI) 2007a Standards of Monitoring During Anaesthesia and Recovery 4th Edition London, AAGBI
- Association of Anaesthetists Great Britain & Ireland (AAGBI) 2007b Guidelines for the Management of Severe Local Anaesthetic Toxicity London, AAGBI
- Auroy Y, Benhamou D, Bargues L, Ecoffey C, Falissard B, Mercier FJ,et al. Major complications of regional anesthesia in France: The SOS Regional Anesthesia Hotline Service. Anesthesiology. 2002 Nov;97(5):1274-80
- Barreett J, et al. Peripheral Nerve Blocks and Peri-operative Pain Relief. 2004 Saunders Ltd UK
- Liu SS, Ngeow JE, Yadeau JT. Ultrasound-guided regional anesthesia and analgesia: a qualitative systematic review. Reg Anesth Pain Med. 2009 Jan-Feb;34(1):47-59
- Marhofer P, Chan VW. Ultrasound-guided regional anesthesia: current concepts and future trends. Anesth Analg. 2007 May;104(5):1265-9
- Nicholls B, Conn D, Roberts A. The Abbott Pocket guide to Practical peripheral nerve blockade Maidenhead, Abbott Laboratories Ltd 2003
- Royal College of Anaesthetists (RCoA) 2006 Risks associated with your Anaesthetic. Section 12: Nerve damage associated with peripheral nerve block Available from: www.rcoa.ac.uk/docs/nerveperipheral.pdf
- Sites BD, Chan VW,et al.. The American Society of Regional Anesthesia and Pain Medicine and the European Society Of Regional Anaesthesia and Pain Therapy Joint Committee recommendations for education and training in ultrasound-guided regional anesthesia. Reg Anesth Pain Med. 2009 Jan-Feb;34(1):40-6
AND a good anatomy book of your choice.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/