General Topics

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Which is the most common nerve that is injured perioperatively?
- Which of the following nerve injuries is least avoidable, even with ideal positioning?
a. Lateral femoral cutaneous nerve
b. Brachial plexus
c. Ulnar nerve
d. Sciatic nerve - Which of the following groups has the best prognosis after nerve injury (Sneddon’s classification)?
a. Neurapraxia
b. Axonotmesis
c. Neurotmesis
INTRODUCTION
Perioperative peripheral nerve injuries (PPNI) are a common and potentially catastrophic complication of anaesthesia and surgery. These injuries include a range of morbidity from transient and clinically minor injury, through to severe permanent injury. The ASA Closed Claims Project database, which was commenced in 1985, is an important source of information about perioperative nerve injury. Closed claims analysis has shown that peripheral nerve injuries are a consistently common cause of litigation claims against anaesthetists, comprising 16% of claims1. Nerve injury was the second most common claim in the entire database.
Incidence of nerve injuries
The exact incidence is difficult to determine, and underreporting of nerve injury complications is likely. Retrospective studies have found that the incidence of permanent nerve damage after a surgical procedure and anaesthesia is 0.03% to 1.4%. Some of these retrospective studies have included patients who received neuraxial blockade or regional anaesthetic techniques, while others have excluded them. Regional and neuraxial techniques may slightly increase the incidence of permanent nerve damage, however this has not been well demonstrated.
Commonly injured nerves include the ulnar nerve (28%), brachial plexus (20%), lumbosacral root (16%), and spinal cord (13%). Injury is less common for the sciatic, median, radial and femoral nerves. Many cases of nerve damage have no identifiable mechanism of nerve injury, such as in 91% of ulnar nerve injuries.
While causative factors in PPNI can be multi-factorial, optimum positioning of surgical patients is helpful to reduce the risk of patient harm. This article will focus on perioperative injury to peripheral nerves and discuss methods to reduce the risk of nerve injury occurring.
CLINICAL FEATURES AND DIAGNOSIS
Onset
Onset of neuropathy symptoms can occur rapidly (within hours) or may be delayed several weeks after the initial insult. Rapid onset of neuropathy is more likely to be direct nerve injury. Delayed onset symptoms are suggestive of tissue inflammation or swelling as a cause.
Character of symptoms and signs
Symptoms can involve sensory and/or motor loss. This may include anaesthesia, paraesthesia, hypaesthesia, hyperaesthesia, and pain. Disabling autonomic dysfunction can occur and chronic regional pain syndrome may develop. Severe cases may lead to muscle wasting, joint dysfunction and bone weakness.
Significance of the injury
This varies greatly and depends on the nature of the symptoms, the extent of the injury as well as the impact on daily life for the patient. For example, motor weakness of the dominant hand of a young carpenter with a family to support is likely to have a different impact when compared to the same injury in a retired elderly patient.
PATHOPHYSIOLOGY
The peripheral nerve consists of a cell body and an axon. The nerve axon is wrapped in Schwann cells, which form the myelin sheath of the cell. The Schwann cells are surrounded by endoneurium, which forms a continuous protective cover along the length of the individual nerve cell. Collections of nerve fibres are surrounded by a layer of connective tissue, called the perineurium. There is an outer layer of connective tissue which collects all the nerve fibre bundles together to form a peripheral nerve. This outermost tissue layer is called the epineurium. Injury to the myelin sheath or axon of a nerve can lead to focal conduction block, degeneration and demyelination.
CLASSIFICATION OF NERVE INJURY
Seddon’s classification
Seddon’s classification system divides nerve injury into three groups based on the nerve pathology.
- Neurapraxia: damaged myelin with intact axon. Impulse conduction across the affected segment fails. Mild and reversible nerve injury. Recovery usually occurs in weeks to months and prognosis is good.
- Axonotmesis: axonal disruption. Endoneurium and other supporting connective tissue are preserved. Recovery and prognosis is variable.
- Neurotmesis: nerve is completely severed. There is complete destruction of all supporting connective tissue structures. Surgery may be required and prognosis is poor.
Sunderland’s classification
Sunderland’s classification system has five groups based on which connective tissue components are disrupted.
- Type 1: Local myelin injury (equivalent to Seddon’s ‘neurapraxia’ group). Recovery in weeks to months. Good prognosis.
- Type 2: Disruption of axonal continuity with Wallerian degeneration. Regeneration of axon required for recovery. Good prognosis.
- Type 3: Loss of axonal continuity and endoneurial tubes. Perineurium and epineurium preserved. Scarring can compromise recovery. Guarded prognosis. Surgery may be required.
- Type 4: Loss of axonal continuity, endoneurial tubes and perineurium damaged. Epineurium remains intact. Poor prognosis. Surgery necessary.
- Type 5: Nerve entirely severed (equivalent to Seddon’s ‘neurotmesis’ group). Surgery required. Prognosis poor.
PREDISPOSING FACTORS
Patient factors
- Thin or obese body habitus
- Old age
- History of vascular disease, diabetes, smoking
- Male gender
- Hypotension, hypovolaemia, dehydration
- Coagulopathy or presence of haematoma near nerve
- Infection/presence of abscess near nerve
- Pre-existing generalized neuropathy
- Hereditary predisposition
- Structural anomaly/congenital abnormality (eg. constriction at thoracic outlet or condylar groove, or arthritic narrowing of joint space)
- Hypothermia (there is a high incidence of nerve injury after induced hypothermia)
Surgical factors
The type of surgery is probably the single most important risk factor in PPNI. Surgery involves the use of needles, sutures, retractors, diathermy and scalpels, which can cause damage to nerves. The highest risk of nerve injury occurs with neurosurgery, cardiac surgery, general surgery and orthopaedic surgery. Risk is higher when surgery involves tourniquet use and tight fitting plaster casts. Ulnar nerve injuries are associated with cardiac surgery because rib retraction may stretch the brachial plexus. Pneumonectomy and axillary lymph node dissection can lead to stretch of the long thoracic nerve leading to motor deficit of the serratus anterior muscle and disrupted scapula movement. The various surgical positions each have specific nerves that are particularly at risk. Positioning considerations are discussed later in this article. Longer hospital stays (greater than 14 days) are associated with higher risk of nerve injury.
Anaesthetic factors and positioning
- Direct needle damage during regional anaesthesia
- Inadequate padding
- Poor positioning
AETIOLOGY
There are many factors that can lead to a PPNI. A nerve injury can occur with a single mechanism, or several can combine to damage the nerve. There are also nerve injuries that occur with no known cause, especially in the case of ulnar nerve injury.
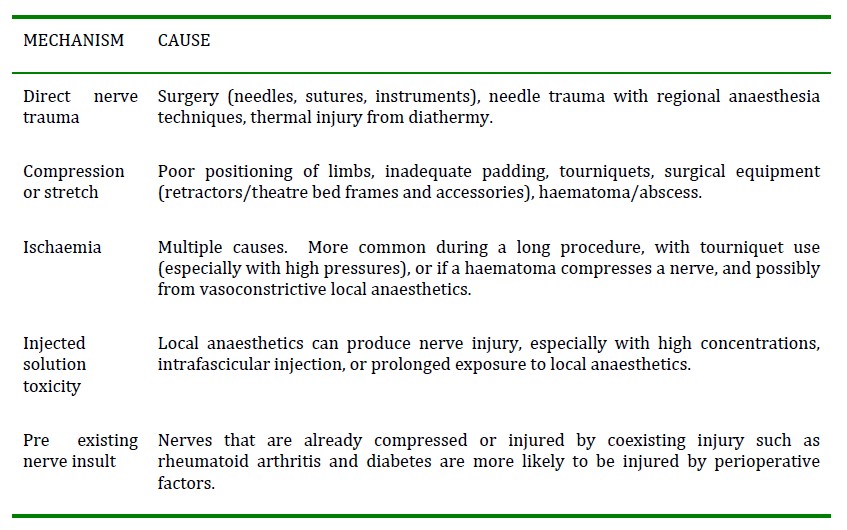
Table 1. Mechanisms for perioperative peripheral nerve injury
THE IMPORTANCE OF POSITIONING
The aim of surgical positioning is to allow good surgical access while minimising risk of harm to the patient. An unconscious surgical patient is reliant on the anaesthetist to be attentive to their safe positioning throughout the procedure. Safe patient positioning includes ensuring that;
- The patient is secure on the operating table
- All limbs are placed in natural positions without stretch to nerves/muscles/tendons/vessels
- All pressure areas are padded and eyes are protected
Peripheral nerve injuries are often related to positioning of the patient and to the surgical procedure. This is not always the case for the ulnar nerve for which spontaneous injury can occur where there is not obvious mechanism of injury. Pressure applied over nerves can damage neurons, cause ischaemic insult, and lead to necrosis. These pressure injuries are most likely when nerves are anatomically exposed to external compression. This situation occurs for the ulnar nerve at the elbow and for the common peroneal nerve at the head of the fibula.
PREVENTION OF POSITION RELATED NERVE INJURY
Some peripheral nerve injuries may be unavoidable, however attention to minimising risk factors can decrease the incidence of nerve insult. In some cases it is appropriate to position the patient prior to induction of anaesthesia, to ensure the position is comfortable. This is useful in the case of fixed flexion disorders and pre existing joint or nerve pain.
Final positioning should be carefully assessed before draping commences. The head and neck must be in a neutral position to help avoid vascular or neural injury. Shoulder abduction with lateral rotation should be avoided where possible to avoid brachial plexus stretch. Upper limb joints should not extend beyond ninety degrees. Forearm supination helps protect the ulnar nerve, as prolonged pronation of the forearm can compress the ulnar nerve in the cubital tunnel.
Good documentation of anaesthetic care includes specific information on positioning, including stating when padding has been used.
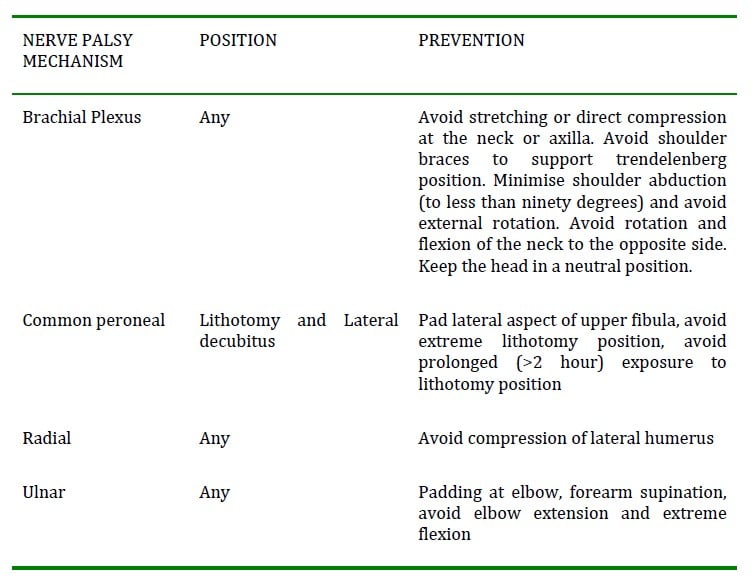
Table 2. Position related complications and their prevention^2
COMMON PERIPHERAL NERVE INJURIES
Ulnar neuropathy
This injury usually occurs at the superficial condylar groove of the elbow and is the most common peripheral nerve injury. The frequency of injury is likely associated with its superficial location. A prospective study of 6538 patients in 1987 found the incidence of ulnar neuropathy to be 1 in 3503. The majority of ulnar nerve injuries are reported to have a delayed onset (greater than 1 day post operatively), and the injury may occur while the patient is resting in bed. Persistent ulnar neuropathy (greater than 3 months duration) occurs in approximately 1 in 2700 surgical patients. It is reported to be more common in males (3:1). The gender difference suggests a narrow cubital tunnel (as found in males) may predispose a person to ulnar nerve injury. Risk increases at extremes of weight and with prolonged hospital stay. The majority of ulnar nerve injuries occur after general anaesthesia. The ulnar nerve is vulnerable to compression against the operating table, especially with forearm extension and pronation. Extreme elbow flexion with the arm across the chest can lead to stretch injury of the ulnar nerve. PPNI of the ulnar nerve can lead to severe ulnar nerve injuries with poor or incomplete recovery.
Brachial plexus neuropathy
The most common causes of brachial plexus neuropathy are stretch, compression or direct injury (via surgical or regional techniques). Brachial plexus stretch can be caused by arm abduction, external rotation and posterior shoulder displacement. This can occur with a supine patient when the neck is flexed laterally, along with an abducted externally rotated arm position. Extreme abduction of the arm, (with hands above the head) also stretches the brachial plexus. Compression of the brachial plexus has been associated with sternotomy and sternal retraction. Compression can also occur in the lateral position when the plexus is compressed between the thorax and the humeral head. The long thoracic nerve can be damaged in brachial plexus PPNI, causing winging of the scapula.
The upper brachial plexus roots are more commonly damaged, and catheter techniques during regional blockade do not appear to increase the incidence of nerve injury. For brachial plexus neuropathy closed claims cases, where a regional block was performed, pain or paraesthesia during injection were reported in only half of the patients.
Lumbosacral nerve root neuropathy
Risk of permanent lumbosacral root injury is approximately 1:5000, and over 90% of cases occur in association with a regional technique. The vast majority of these are associated with central neuraxial approaches. Symptoms on injection are often reported, including pain or paraesthesia on injection. Risk of lumbosacral nerve root injury increases with the number of attempts to pass a needle through the area. The most common ongoing symptom is persistent paraesthesia.
Other common peripheral nerves injured perioperatively
Other nerves commonly injured include the common peroneal, radial, sciatic, femoral, tibial, saphenous, supraorbital, facial nerve, and lateral cutaneous nerve of the thigh.
Common peroneal nerve
This is the most frequent of the lower limb nerve injuries. The common peroneal nerve is at risk of injury in the lithotomy position, where it can be compressed by the head of the fibula, or in the lateral position where it can be compressed between the fibula and the operating table.
Radial nerve
Radial nerve injury occurs most commonly due to compression of the radial nerve between the operating table and the humerus. Radial nerve injury can also occur when a patient is in the lateral position with their upper arm abducted beyond ninety degrees and suspended from a support.
Sciatic nerve
The sciatic nerve is more at risk with very thin patients, long procedures and hard operating surfaces. Elevation of the opposite buttock (such as for some hip surgery) increases the risk further. Excessive stretch of the sciatic nerve can occur when the lithotomy position is used and extreme external rotation of the thigh is applied. Sciatic nerve injury has been reported post coronary artery bypass graft, possibly from prolonged nerve pressure along with low perfusion pressure.
REDUCING THE RISK OF NERVE INJURY
The anaesthetist has a responsibility to be aware of the potential for nerve injury and interventions which can minimise the risk. In addition to positioning considerations as described above, there are other ways to reduce the risk of perioperative nerve injury.
Hypotension should be avoided and haemodynamic stability maintained. Pre-existing coagulopathy or infection should be identified and treated as appropriate. The timing of the procedure and the anaesthetic technique should be considered carefully in the presence of coagulopathy or infection.
Patients with pre-existing neuropathy should be carefully examined and the findings documented. An anaesthetic technique should be selected that is appropriate for the neuropathy and clinical circumstances. For example, the anaesthetist may choose to avoid a regional technique where preexisting neuropathy exists and alternative analgesia and anaesthesia techniques are safe. There may however, be patients with neuropathy where exposure to additional risk factors (such as tourniquets, lithotomy position, and regional anaesthesia) is overall the safest choice and unavoidable.
Surgical positions known to have a high risk of nerve injury should be avoided wherever possible. If a tourniquet is necessary it should be pneumatic. The tourniquet pressure and duration of use must be minimised.
MANAGEMENT OF PERIOPERATIVE PERIPHERAL NERVE INJURIES
Assessment
The patient should be assessed, including a full history and examination. Findings must be well documented and neurologist review should occur early. An experienced neurologist can usually distinguish between specific peripheral nerve root injury and radiculopathy. Investigations include nerve conduction studies. Progressive or severe pathology needs urgent neurologist assessment and immediate investigation.
Electromyography and Nerve conduction studies
Electromyography (EMG) involves examination of muscle activity at rest and during movement. EMG provides useful information about the nerve supply to a muscle. Nerve conduction studies involve stimulation of motor or sensory nerves and recording of propagated action potentials. Assessment of conduction velocities is possible, and the number of nerve fibres participating in conduction can be estimated. These tests are performed by a neurophysiologist and are interpreted in relation to the clinical history.
Electrophysiology can help distinguish between nerve dysfunction due to axonal degeneration (such as with PPNI) and nerve dysfunction due to demyelination (such as with chronic compressive lesions including carpal tunnel syndrome). The electrophysiological diagnosis of degeneration is based on finding reduced numbers of functioning axons.
Diagnosis of the site of the lesion is based on the distribution of abnormal findings. In demyelination, there is focal slowing of motor and or sensory conduction across the injured part of the nerve with normal conduction proximal and distal to the injury.
The timing of electrophysiology studies is important in obtaining an accurate diagnosis. Fourteen days or more may be required for the process of nerve degeneration to be completed. For this reason it is often recommended to have electrophysiology studies done several weeks after the onset of symptoms to avoid falsely reassuring assessment.
Electrophysiology studies can also be used to monitor nerve injury recovery over time.
CONTROVERSIES IN PERIPHERAL NERVE INJURIES
Studies have shown that the anaesthetic technique is unrelated to incidence of ulnar nerve injury. Unconscious patients are not at increased risk of ulnar nerve injuries compared to awake patients. This leads one to question whether patient positioning, nerve compression and stretch are significant mechanisms in perioperative ulnar nerve injury. Initial symptoms of ulnar nerve injury occur most frequently more than 24 hours after the surgical procedure. In addition, abnormal nerve conduction is often found in the contralateral unaffected arm, indicating likely predisposition to ulnar nerve symptoms preoperatively. These finding and its delayed onset has lead to much debate regarding the aetiology of the injury. Closed claims analysis has also demonstrated that nerve injury can occur even with optimal patient positioning and padding to risk areas (such as the elbow.) Thus, the aetiology of peripheral nerve injury can be complex and multifactorial.
OUTCOMES
In most cases, injuries resolve within 6-12 weeks. More than 50% of patients typically regain full sensory and motor function within 12 months. Patients with poor recovery can have ongoing or permanent symptoms. Permanent injury may be minor (such as small area of sensory loss that is minimally inconvenient to the patient), or major and disabling (such as significant motor loss and chronic pain). Poor recovery can have a profound impact on quality of life for patients with ongoing nerve injury.
Perioperative peripheral nerve injuries remain a common and potentially avoidable perioperative patient injury. Avoiding nerve injury requires understanding of the anatomy and pathophysiology involved in these injuries, and attention to using all possible preventative measures. If nerve injury symptoms or signs are identified, thorough assessment and investigation must be undertaken. Perioperative nerve injury can cause permanent and severe disability for patients. Thorough preventative measures are essential for patient safety.
- Perioperative nerve injury is usually avoidable
- Nerve injury can be severe, permanent and disabling
- Good positioning of the patient for surgery can reduce the risk of most perioperative nerve injuries
ANSWERS TO QUESTIONS
- Which is the most common nerve that is injured perioperatively?
Ulnar nerve injury is significantly more common than any other nerve injury. - Which of the following nerve injuries is least avoidable, even with ideal positioning?
Over 90% of ulnar nerve injuries have no known cause. They can occur even with ideal positioning and padding. - Which of the following groups has the best prognosis after nerve injury (Sneddon’s classification)?
A neurapraxia is the mildest injury and has a good prognosis.
WEB RESOURCES
An excellent summary of the issues can be found at the ASRA Practice Advisory on Neurologic Complications in Regional Anesthesia and Pain Medicine: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2869280/
More information on the ASA closed claims database can be found here: http://depts.washington.edu/asaccp/index.shtml
REFERENCES and FURTHER READING
- Lalkhen, A. G. & Bhatia, K. Perioperative peripheral nerve injuries. Contin Educ Anaesth Crit Care Pain; 2012;12,38–42.
- Nitti, J. & Nitti, G. Anesthetic complications. Clinical anesthesiology; 2006; 959–977.
- Alvine, F. G. & Schurrer, M. E. Postoperative ulnar-‐nerve palsy. Are there predisposing factors? J Bone Joint Surg Am; 1987; 69, 255–259.
- Sawyer, R. J., Richmond, M. N., Hickey, J.D. & Jarratt, J. A. Peripheral nerve injuries associated with anaesthesia. Anaesthesia; 2000; 55, 980-‐991.
- Werrett, G. Consent and anaesthetic risk. Oxford Handbook of anaesthesia; 2008; 30–33.
- Contractor, S. & Hardman, J. G. Injury during anaesthesia. Contin Educ Anaesth Crit Care Pain; 2006; 6, 67–70.
- Kroll, D. A., Caplan, R. A., Posner, K., Ward, R. J. & Cheney, F. W. Nerve injury associated with anesthesia. Anesthesiology; 1990; 73, 202–207.
- Cheney, F. W., Domino, K. B., Caplan, R. A. & Posner, K. L. Nerve injury associated with anesthesia: a closed claims analysis. Anesthesiology; 1999; 90, 1062–1069.
- Welch, M. B. et al. Perioperative peripheral nerve injuries: a retrospective study of 380,680 cases during a 10-‐year period at a single institution. Anesthesiology; 2009; 111, 490–497.
- Neal, J. M. et al. ASRA Practice Advisory on Neurologic Complications in Regional Anesthesia and Pain Medicine. Reg Anesth Pain Med; 2008; 33, 404–415.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/