Basic Sciences

Questions
- List the factors that determine the duration of a local anaesthetic nerve block.
- How much more potent is bupivocaine when compared to lidocaine?
- How does the addition of epinephrine increase the duration of a nerve block?
- What is the maximum recommended dose of:
- Plain lidocaine?
- Lidocaine with epinephrine 1:200 000?
- What is the recommended dose of
- Clonidine to be added to local anaesthetic solution?
- Sodium bicarbonate?
In this section, I will discuss the pharmacology of local anaesthetic agents and then describe the various additives used with these agents. I will also briefly cover the pharmacology of the other drugs commonly used in regional anaesthesia practice. A great number of drugs are used in regional anaesthesia. I am sure no two anaesthetists use exactly the same combinations of drugs. I will emphasise the drugs I use in my own practice but the reader may select a different range of drugs according to his experience and drug availability. The important point is to use the drugs you are familiar with. For the purposes of this discussion, I am going to concentrate on the following drugs:
Local anaesthetic agents
- Lidocaine
- Prilocaine
- Bupivacaine
- Levobupivacaine
- Ropivacaine
Local anaesthetic additives
- Epinephrine
- Clonidine
- Felypressin
- Sodium bicarbonate
Commonly used drugs
- Midazolam/Temazepam
- Fentanyl
- Ephedrine
- Phenylephrine
- Atropine
- Propofol
- Ketamine
- EMLA cream
- Ametop gel
- Naloxone
- Flumazenil
PHARMACOLOGY OF LOCAL ANAESTHETIC DRUGS
History
- In 1860, cocaine was extracted from the leaves of the Erythroxylon coca bush.
- In 1884 Koller used it as a topical ophthalmic anaesthetic.
- In 1904, procaine was synthesised. Amethocaine was released in 1930. These agents were esters and, despite a risk of allergic reactions, were widely used.
- In 1943 Lofgren developed lidocaine. This was an amide and had a low risk of allergic reactions. This was followed by mepivacaine (1957), prilocaine (1960), bupivacaine (1963), ropivacaine(1997) and levobupivacaine (2000).
In North America, the esters (amethocaine, chloroprocaine and procaine) are still used but there is a growing trend in other parts of the world to avoid the esters due to their allergic potential. The amides (lidocaine, prilocaine, mepivacaine, bupivacaine, levobupivacaine and ropivacaine) are widely used throughout the world, and I propose to discuss only these agents in this article. An easy method to determine if a local anaesthetic is an ester or an amide is to check the prefix. Amides have an ‘i’ in the prefix, esters do not.
AMIDES: lidocaine, prilocaine, mepivacaine, bupivacaine, ropivacaine and levobupivacaine.
ESTERS: cocaine, procaine, amethocaine and chloroprocaine.
Lidocaine, bupivacaine, levobupivacaine, prilocaine and ropivacaine are all amides. They are stable in solution and are metabolised in the liver. Local anaesthetics act by causing a reversible conduction block in nerves. By blocking the sodium channels in the nerve membrane, they interfere with the nerve action potential and thus prevent propagation of the action potential along the axon. These agents cause vasodilation, which increases their tissue absorption. By adding a vasoconstrictor, the duration of block increases and the local anaesthetic toxicity risk decreases.
The block duration is influenced by several factors:
- The nature of the drug ( lidoocaine – short acting; bupivacaine – long acting)
- The drug concentration (the higher the concentration, the longer the block)
- The drug volume ( the larger the volume, the faster the onset and the more dense the block)
- Use of additives ( epinephrine and sodium bicarbonate speed the onset and prolong the block)
- Type of block ( Leg blocks last longer than arm blocks. This is a function of nerve size and vascularity)
Local anaesthetics can be used topically (conjunctiva, skin, mucous membranes and ear drum). They act within minutes and last an hour or so. Care is required if large areas are exposed to a topical local anaesthetic, as toxic blood levels may ensue. This is especially so in infants and small children.
When the skin is infiltrated, the action is almost immediate, owing to the small unmyelinated nerve fibres being rapidly penetrated by the local anaesthetic. Skin infiltration of plain lidoocaine lasts 2 hours and plain bupivacaine lasts 4 hours. These times can be extended by adding a vasoconstrictor.
Larger nerves (e.g. sciatic) are thicker and well myelinated. The local anaesthetic takes longer to penetrate these nerves and hence the onset time is longer.
It is not surprising that local anaesthetics act on other cell membranes in the same manner as nerve membranes. Of particular importance is heart muscle cells. By blocking the sodium channels in myocardial cells, local anaesthetics cause pacemaker suppression. resulting in bradycardia and sinus arrest. There is also a negative inotrophic effect.
Bupivacaine can cause refractory ventricular fibrillation which is difficult to defibrillate.
Fortunately, the CNS toxic signs and symptoms occur at a lower serum level and give a degree of advance warning as to possible cardiac toxicity.
Lidocaine (lignocaine, xylocaine)
This agent has been used in clinical practice for almost 60 years. It has a rapid onset of action but the block is of a relatively short duration.
Clinical usage
- Skin infiltration – 0.2–1.0 % lidocaine. Use with epinephrine 1:200,000 or 1:400,000
- Biers block (IVRA) – 40 ml of 0.5% lidocaine (without epinephrine)
- Peripheral nerve blocks – 1–2% lidocaine (with or without epinephrine)
- Dental blocks – lidocaine 2% (with epinephrine 1:80,000)
- Topical anaesthesia – 2% gel (urethra) or 4% spray (oro-pharyngo-laryngo- tracheal)
- Subarachnoid block – 2% lidocaine plain (no epinephrine). I no longer use 5% lidocaine, as it is associated with transient radicular irritation (TRI). The risk of this complication is low with the less concentrated solution
The recommended maximum safe doses of lidocaine are as follows:
- LIDOCAINE WITHOUT EPINEPHRINE —— 3 mg/kg
- LIDOCAINE WITH EPINEPHRINE —— 7 mg/kg
These maximum dosages are not universally accepted. Patients vary both in body habitus and metabolism. Rates of absorption vary in tissues, depending on the blood flow. Body weight gives no indication of lean tissue mass.
I believe the above figures are conservative but safe. Lidocaine can be carbonated by adding sodium bicarbonate. This shortens the onset and prolongs both the intensity and duration of block.
Prilocaine (Citanest)
This drug is closely related to lidocaine and is very similar in its clinical action. Its advantage is that it is more rapidly metabolised and hence less toxic. It can cause methaemoglobinaemia when used in high dosage (> 600 mg). Methaemoglobinaemia causes a blue skin discolouration and results in false pulse oximeter readings. The condition is usually benign and resolves within a couple of hours. The treatment is methylene blue 1 mg/kg i.v. over 5 minutes. The clinical usage and doses are similar to those of lidocaine. Prilocaine is safer if large doses of local anaesthetic are being used. Prilocaine 0.5% is the drug of choice in Biers block.
The recommended maximum safe doses of prilocaine are as follows:
- PRILOCAINE WITHOUT EPINEPHRINE —– 6 mg/kg
- PRILOCAINE WITH EPINEPHRINE —– 9 mg/kg
Bupivacaine (Marcain)
This drug has been used in clinical practice for more than 40 years. It is remarkably stable in solution and is commercially available in 0.25% and 0.5% solutions (with and without epinephrine). Spinal heavy bupivacaine (0.5% bupivacaine + 6% glucose) is also manufactured. It is four times more potent than lidocaine. Therefore, 0.25% bupivacaine is equipotent with 1% lidocaine. Bupivacaine is particularly cardiotoxic and should never be used in Biers blocks. Bupivacaine binds tightly to tissues and thus has a long duration of action (up to 24 hours in some cases). Adding epinephrine will decrease its toxicity by delaying the drug absorption but will have minimal effect on the duration of the block.
The recommended maximum safe doses of bupivacaine are as follows:
- BUPIVACAINE WITHOUT EPINEPHRINE ——- 2.0 mg/kg
- BUPIVACAINE WITH EPINEPHRINE ——- 2.5 mg/kg
Levobupivacaine
This is a relatively new agent and to all intents and purposes is the same as bupivacaine. Bupivacaine is a racemic mixture of the R and S enantiomers. Levobupivacaine contains the S enantiomer only. Compared with bubivacaine it is said to have greater vasoconstrictive action and less motor block. The real advantage is that it is apparently less cardiotoxic.
It may replace bupivacaine for safety reasons but it is significantly more expensive. It is not currently licensed for subarachnoid injection.
The recommended maximum safe dose of levobupivacaine is as follows:
- LEVOBUPIVACAINE —– 2.5–3.0 mg/kg (insufficient data)
Ropivacaine (Naropin)
Concerns about bupivacaines toxicity led to the development of ropivacaine. Ropivacaine is an aminoamide local anaesthetic. It has been used clinically for the past decade. Clinical evidence indicates thst it is indeed less toxic than bupivacaine. In particular, it is less cardiotoxic.
The addition of epinephrine or sodium bicarbonate does not appear to alter the speed of onset or duration of the block. The intensity and duration of the motor block are lower than with bupivacaine. It is slightly less potent than bupivacaine (in peripheral nerve blockade, 0.5% bupivacaine is equipotent with 0.6% ropivacaine).
It is not currently licensed for subarachnoid usage. I have found it to have much the same clinical profile as bupivacaine but its increased safety margin gives it a clear advantage. I expect it will replace bupivacaine in the near future.
The recommended maximum safe dose of ropivacaine is as follows:
- ROPIVACAINE (WITH or WITHOUT EPINEPHRINE ) — 3-4 mg/kg
In summary, the following principles apply in the clinical usage of local anaesthetics:
- For surgical cases where rapid onset peripheral blockade is required, use lidocaine 1-2% or prilocaine 1-2%.
- If prolonged postoperative analgesia is required, use bupivacaine 0.25-0.5% (or ropivacaine 0.4–0.7%)
- If large doses of local anaesthesia are used (e.g. plexus blocks and expansive skin infiltration),
- it is safer to use ropivacaine or levobupivacaine
- There is little clinical advantage in mixing local anaesthetics
- Do not inject if patient complains of severe pain
- There should be no resistance to injection
- NEVER exceed the maximum recommended dose
LOCAL ANAESTHETIC ADDITIVES
Epinephrine, felypressin, clonidine and sodium bicarbonate can be added to local anaesthetic agents. They act to prolong the duration and intensity of the block, as well as reducing the risk of local anaesthetic toxicity.
Epinepherine
Epinephrine is added to local anaesthetics to cause vasoconstriction. This reduces the local anaesthetic absorption and results in the twin benefits of prolonging the block duration and reducing toxicity. Epinephrine does not significantly prolong the duration of bupivacaine or ropivacaine but it does slow the absorption of these agents and thus reduces peak plasma levels. This reduces the toxicity risk of these two local anaesthetics.
Epinephrine is commercially available in two ampoule sizes:
- A 1 ml ampoule containing 1 mg (i.e. 1:1000)
- A 10 ml ampoule containing 1 mg (i.e. 1:10,000)
It is important to understand exactly what these figures mean. Novice practitioners are often confused by this subject. A 1% solution of any drug contains 1 gram (i.e. 1000 mg) of drug per 100 ml of solution.
Therefore, a 1% lidocaine solution contains 1000 mg of lidocaine per 100 ml (which is the same as 10 mg/ml)
Commit the following to memory: A 1% LIDOCAINE SOLUTION CONTAINS 10 MG OF LIDOCAINE PER ML.
Epinephrine concentration is measured differently. A 1 mg ampoule of 1:1000 epinephrine means that the solution contains 1 mg of epinephrine per ml.
Commit the following to memory: EPINEPHRINE 1:1000 CONTAINS 1 MG OF EPINEPHRINE PER ML.
- It follows that a 1:10,000 solution of epinephrine contains 0.1 mg of epinephrine (or 100 micrograms) per ml
- OR a 1:100,000 solution contains 10 micrograms per ml
- OR a 1:200,000 solution contains 5 micrograms per ml
- OR a 1:400,000 solution contains 2.5 micrograms per ml
Commit the following to memory as it is the most common epinephrine concentration used in regional anaesthesia: A 1:200,000 EPINEPHRINE SOLUTION CONTAINS 5 MICROGRAMS PER ML.
It is essential the reader has a clear understanding of the above calculations and I suggest you take a piece of paper and practise a few hypothetical examples.
Example 1
How do you make up 25 ml of 2% lidocaine with 1:250,000 epinephrine?
Answer
Take an ampoule of 1:1000 epinephrine (i.e. 1 mg/ml). Add 10 ml of saline to give 1:10,000 (i.e. 100 micrograms per ml).
Add 1 ml of this epinephrine solution to 25 ml of 2% plain lidocaine. (i.e. 100 micrograms per 25 ml = 4 micrograms per ml). This is not exactly correct but near enough.
Example 2
How do you prepare a 1:200,000 solution of epinephrine in 1% lidocaine?
Answer
Take 0.1 ml of epinephrine from a 1:1000 ampoule and add it to 19.9 ml of 1% plain lidocaine. Epinephrine-containing solutions should not be used in parts of the body which are supplied by end arteries (fingers, toes, penis, nose, ears).
The maximum safe dose of epinephrine is controversial. There is no good reason to use concentrations in excess of 1:200,000 in the skin and in fact 1: 400,000 is quite adequate in most cases. Use 1:200,000 for peripheral nerves. Adopt the habit of never using a concentration greater than 1:200,000 (5 micrograms/ml).
Dentists prefer 1:80,000 but the volumes used are low.
MAXIMUM SAFE DOSE OF EPINEPHRINE = 4 MICROGRAMS PER KG.
Therefore, an 80 kg man = 320 micrograms = 64 ml of a 1:200,000 solution.
This maximum dose should be reduced in cases of serious ischaemic heart disease, thyrotoxicosis and hypertension. In such cases, it would be prudent to avoid epinephrine all together. Remember that epinephrine reduces the peak local anaesthetic blood levels but this varies with the site of block. For instance, absorption occurs rapidly following an intercostal block but more slowly from a brachial plexus block. Epinephrine containing local anaesthetic solutions give an early warning of accidental intravascular injection. Always inject large volumes slowly and listen carefully to the pulse oximeter. A sudden onset tachycardia is an emergency stop sign!
Felypressin (Octapressin)
Felypressin is a synthetic derivative of vasopressin from the posterior pituitary. It causes vasoconstriction but has minimal antidiuretic effect. It has no effect on cardiac rate or rhythm and is therefore popular in dental surgery where, used in conjunction with 3% prilocaine, it increases the intensity and duration of dental nerve blocks.
Felypressin is useful when epinephrine is contraindicated (e.g. serious ischaemic heart disease, thyrotoxicosis and hypertension). The commonly used vasoconstrictive concentration is 0.02–0.03 U/ml.
Clonidine (Catapres)
Clonidine is an alpha-2 adrenoreceptor agonist. For many years it was used to treat hypertension by its centrally mediated reduction of sympathetic drive. Clonidine has widespread effects on the nervous system. It acts on the brain to cause sedation and has analgesic effects on the central and peripheral nervous systems.
It prolongs and intensifies blocks when added to local anaesthetics. Adding clonidine 75–100 micrograms can extend the duration of peripheral blocks by 50–100%.
For Biers blocks (IVRA), clonidine 150 micrograms can be added to the local anaesthetic solution. It reduces tourniquet pain and causes no adverse effects when the tourniquet is released. Clonidine is regularly used when prolonged postoperative analgesia is required.
Sodium bicarbonate
Sodium bicarbonate is added to local anaesthetics to raise the pH of the solution. This has the effect of increasing the proportion of unionised local anaesthetic, enabling it to penetrate the nerve membranes more readily. Thus, the speed of onset is increased. It also prolongs the duration and intensity of the block. Bicarbonate reduces the pain of injection (injection pain is associated with a low pH and cold solution). The recommended dose is 1 ml of 8.4% sodium bicarbonate per 10 ml of local anaesthetic. There is little advantage in adding it to bupivacaine or ropivacaine.
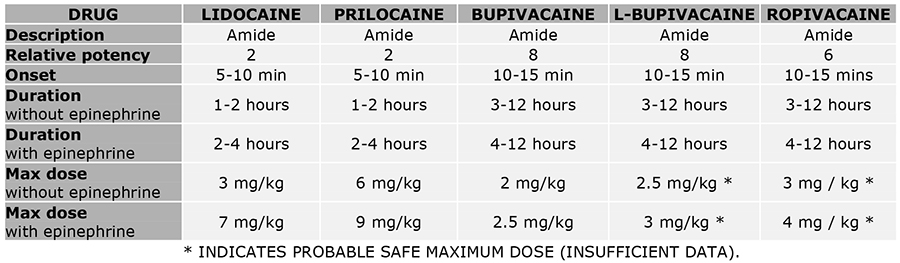
Table 1: Local anaesthetic drug information
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/