Basic Sciences

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation. Please answer True or False:
- You are transferring an intubated patient with a traumatic subdural haematoma and C2/3 fractures. Regarding the physiological changes that can occur during land ambulance transfer:
a. There can be an increase in intracranial pressure (ICP) during deceleration
b. Acceleration can be associated with a decrease in blood pressure
c. There is potentially an increased risk of aspiration during acceleration
d. There is a risk of hypothermia during transfer
e. Inertial forces can potentially displace unstable spinal fractures - An intubated and ventilated patient on the critical care unit is due to be transported by aircraft for treatment nearer home. Important considerations during air transport include:
a. Ascent causes a decrease in the volume of gas filled spaces
b. Endotracheal cuffs can be filled with saline to prevent changes in volume on ascent
c. Endotracheal intubation during flight is relatively easy due to patient positioning and access
d. Pneumothoraces should never be drained prior to transfer
e. Air transport is always the fastest and preferred method of patient transport - Regarding the physical principals related to transfer:
a. Only the patient is subjected to inertial forces
b. Newton’s third law of motion states that for every action there is an equal and opposite reaction
c. Atmospheric pressure increases with altitude
d. The fractional concentration of oxygen remains constant with changes in altitude
e. Boyles law states that at a constant temperature the volume of a given mass of gas varies inversely with the absolute pressure
Key Points
- Critically ill patients are at an increased risk of instability during transfer due to their acute pathology and current drug therapy, which can reduce the patient’s ability to compensate.
- Inertial forces from acceleration and deceleration can cause significant changes in blood pressure, heart rate, intracranial and gastric pressure.
- Flying at altitude exposes patients to the risk of hypoxia and hypothermia from the drop in atmospheric pressure and adverse events secondary to the expansion of gas filled spaces, vibration and inertial forces.
- Time spent preparing and stabilising the patient and predicting potential problems prior to transfer is essential in preventing adverse events and limiting physiological changes during transfer.
INTRODUCTION
The transfer of critically ill patients either from the prehospital setting or between hospitals is frequently performed to enable patient access to specialist care or repatriation to a hospital nearer to home. It’s estimated that over 11,000 inter-hospital transfers of critically ill patients are undertaken in the UK each year.
The transfer of critically ill patients is not without risk and protocols to guide the transfer of critically ill patients from the Intensive Care Society (ICS)[1] and the Association of Anaesthetists of Great Britain and Ireland (AAGBI)[2] exist.
Adverse events commonly occur during inter-hospital transfer of critically ill patients. A prospective audit from the Netherlands reported adverse events occurred in 34% of transfers, of these adverse events 70% were felt to be avoidable. Many of these adverse events related to equipment failure, inadequate preparation, and poor documentation/communication. A recent ATOTW article on inter-hospital transfers looks at many of these aspects in more detail [3].
Critically ill patients can be exposed to significant physiological changes during transfer that can lead to significant instability with hypoxia, hypotension, arrhythmias and changes in intracranial pressure (ICP). This tutorial will explore the physiological effects that land and air transfer have on critically ill patients and describe how these adverse physiological sequelae can be avoided or reduced.
PHYSIOLOGICAL EFFECTS OF LAND TRANSFER
Patients are commonly transported from the pre-hospital setting and between hospitals via land ambulance. The effects of deceleration and acceleration can be significant in critically ill patients due to their reduced ability to compensate. Acceleration and deceleration have an impact on a patient’s physiology because of Newton’s laws of motion (Figure 1).
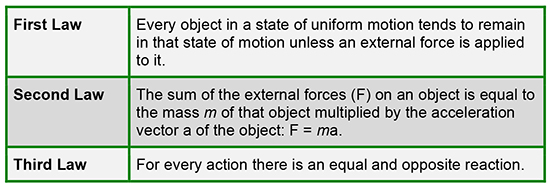
Figure 1: Newton’s three laws of motion
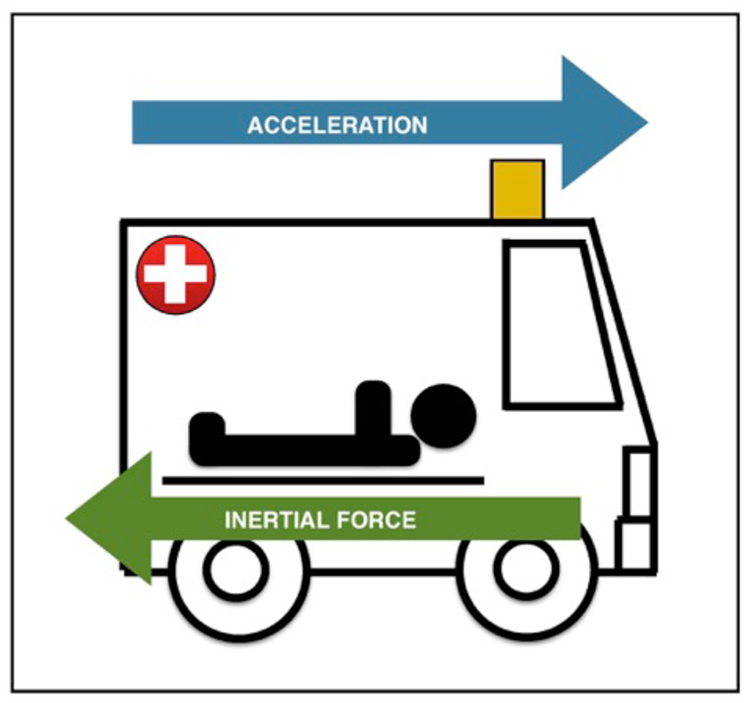
Figure 2a: Acceleration
Newton’s third law states that for every action there is and equal and opposite reaction. When a patient is accelerated due to the application of an external force there will be and equal and opposite force enacted termed inertia (Figure 2a/b)
For example, as a patient accelerates in an ambulance (figure 2a) the external force causing acceleration is towards the patient’s head. The inertia force is in the opposite direction i.e. towards the patient’s feet. This inertial force causes the displacement of non-tethered organs and fluids such as blood towards the patients feet. The amount of displacement depends on the rate, magnitude and direction of acceleration. The direction of acceleration can be in the anterior-posterior, lateral or cephalo-caudal axis. Commonly in ambulance transport the axis of acceleration is in the cephalic-caudal direction, which has the most significant effect on physiology. [4]
Deceleration (figure 2b) would have the opposite effect, this time the external force causing deceleration is towards the patient’s feet and displacement of blood would be towards the head. The breaking force of an ambulance is much greater than its acceleration force and as such deceleration has a greater impact on a patient than acceleration. [4]
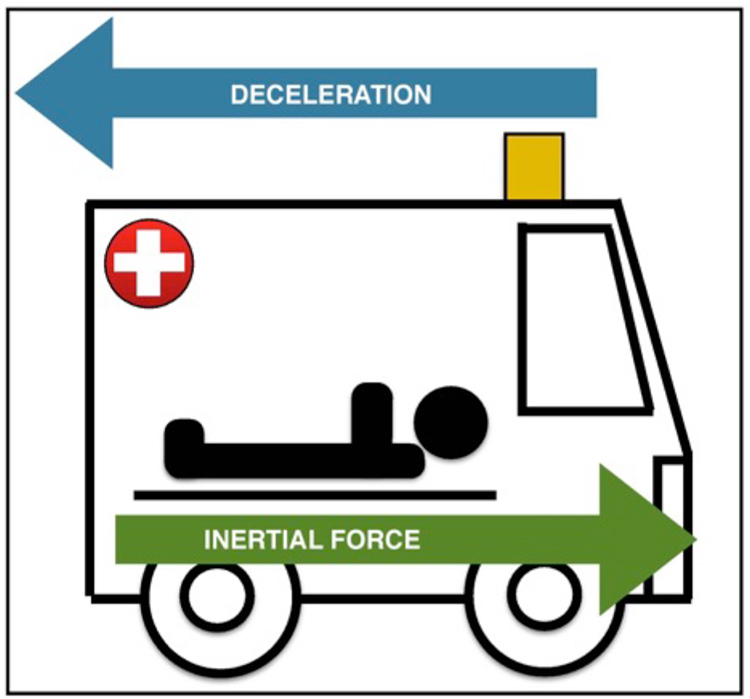
Figure 2b: Deceleration
Physiological consequences of acceleration
Cardiovascular system:
- Blood will pool in the feet resulting in decreased venous return and cardiac output causing hypotension. In health the baroreceptor receptor reflex would compensate for this by an increase in vascular tone, however, in critical illness this reflex can be significantly reduced or absent either due to the critical illness eg sepsis or secondary to drug therapy. Profound hypotension can occur requiring increased inotropic and vasopressor support. Hypotension is exacerbated by hypovolaemia and positive pressure ventilation, both of which reduce preload.[4]
Neurological system:
- Hypotension can lead to reduced cerebral perfusion which can affect a patient’s conscious level and is significant in those with head injuries where cerebral perfusion pressure needs to be maintained.
- Cerebral perfusion pressure (CPP) = Mean Arterial Pressure (MAP) – Intracranial pressure (ICP)
Physiological consequences of deceleration:
Cardiovascular system:
- Venous return will be increased due to inertial forces ‘pushing’ blood in a cephalic direction (towards the head). In patients with cardiac impairment the increased volume in the right ventricle can lead to cardiac failure, pulmonary oedema, and arrhythmias.
Neurological system:
- Due to the displacement of venous blood and CSF the ICP is increased. This is important in patients who already have a raised ICP as their cerebral perfusion may be further compromised during deceleration.
Gastrointestinal system:
- Inertial force displaces the stomach towards the patient’s head, this can increase the risk of aspiration.
- This upwards displacement of viscera can also increase trans-diaphragmatic pressure and cause either smaller tidal volumes or higher intrathoracic pressure depending on the mode of ventilation in use.
Musculoskeletal system:
- In patients with significant spinal injuries the inertial force acting during deceleration results in axial loading which can cause displacement of unstable spinal fractures.
It is important to note that these forces also apply to equipment and medical personnel. For this reason equipment should be secured and all medical personnel should be sat down and secured with a seat belt during ambulance movement to reduce the risk of injury. Medical staff are less affected physiologically due to having intact compensatory mechanisms and the direction of inertia acting in the anterior posterior direction because of their seated position. Acceleration and deceleration are dynamic hazards however, there are also static hazards that have a significant effect on patients including:
Noise
- This can affect communication between medical staff as well as patients and cause distress.
Temperature
- Ambulances are not able to regulate their temperature as effectively as hospitals, therefore in extreme heat and cold the patient is exposed to the risk of hypo and hyperthermia. It is therefore, important to monitor a patient’s temperature closely during transfer and prepare for cold temperatures with additional blankets and fluid warmers.
Duration
- Pressure areas need to be protected and monitored especially during long journeys. Space is often limited during transfer and meticulous attention needs to be paid to the position of lines and the temptation to rest equipment on the patient must be avoided.
- During prolonged transfer, blood and other bodily fluids can pool in dependent parts of the body and in addition to pressure over bony prominences, this may contribute to tissue maceration and the development of pressure sores. On hard extrication boards (spinal boards) the early stages of pressure sore development can be seen after only 20 minutes in healthy volunteers with normal skin perfusion. In critically ill patients receiving vasopressor therapy these changes can happen more quickly. For this reason, extrication boards should not be used for prolonged transfers, and the Royal College of Surgeons of Edinburgh have released a position statement in 2013 on pre-hospital spinal immobilisation to this effect[5]. A vacuum mattress should be used wherever possible during transfers.
PHYSIOLOGICAL EFFECTS OF AIR TRANSFER
Air transfer either by helicopter or fixed wing aircraft is commonly carried out by the military and other specially trained personnel following additional training. It is however, important to understand the physiological effects of air transport because ICU patients may be transported by air and this will affect how the patient is prepared prior to transfer.
Physiological effects of altitude
Atmospheric pressure
- Atmospheric pressure decreases in a non linear fashion with altitude. The fractional concentration of oxygen remains constant at 0.21 however the partial pressure of oxygen falls. A fall in atmospheric pressure results in a reduction in the alveolar partial pressure of oxygen, which can lead to hypoxia unless supplemental oxygen (increased FiO2) is given.
- Hypoxia can cause tachycardia, bradycardia, arrhythmias, hypotension, tachypnoea behavioural changes and altered conscious level in all people. Oxygen supplementation in healthy individuals is usually not required until above 10,000ft.
- At sea level the atmospheric pressure is 101Kpa, at 10,000ft the atmospheric pressure falls to 70kpa. This drop in atmospheric pressure has a significant effect on the partial pressure of oxygen as demonstrated by the alveolar gas equation figure 3.
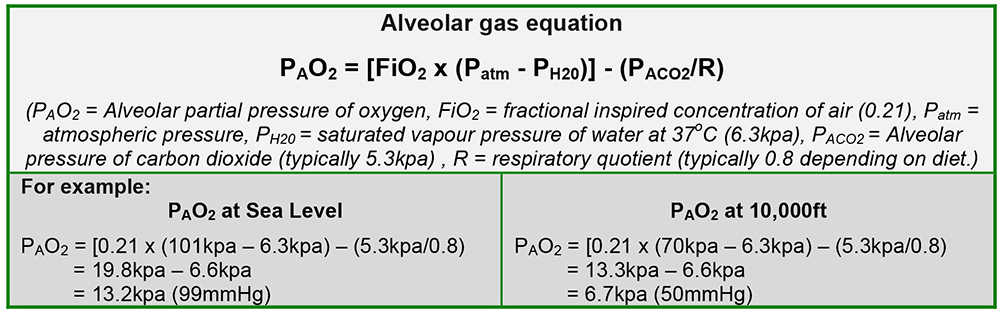
Figure 3: Alveolar gas equation
If a critically ill patient becomes hypoxic during flight this can be treated with either an increase in the inspired oxygen concentration (fiO2) or by increasing the partial pressure of oxygen by reducing the altitude of flight or pressuring the cabin to a lower altitude.
Consideration should be given to patients with significant alveolar:arterial gradient mismatches such as advanced COPD, pulmonary contusions or pulmonary fibrosis as the relative hypoxia at altitude will result in a lower PaO2 in this patient group. It is therefore important to discuss the flying altitude with the pilot prior to takeoff so that a risk assessment of the potential impact of altitude on the patient can be made.
Volume expansion
- Boyles law states that at a constant temperature the volume of a given mass of gas varies inversely with the absolute pressure (Figure 4). Therefore, as you ascend the volume of any gas filled spaces will increase. This will affect any gas filled body cavities and equipment because the volume of gas in enclosed spaces will increase with the drop in atmospheric pressure.
- Physiological effects of volume expansion:
- Pneumothoraces should be vented and a chest drain inserted prior to air transfer to avoid an increase in the size of a pneumothorax and risk of tensioning.
- Patients with bowel obstruction or recent bowel surgery requiring anastamosis should be flown at lower altitude or land transfer considered. Fixed wing aircraft may be considered as they are able to pressurise their cabins to sea level or a lesser altitude.
- Expansion of air in the eustachian tubes can cause pain and discomfort during ascent and descent if patients are not able to equilibrate. This also applies to medical staff.
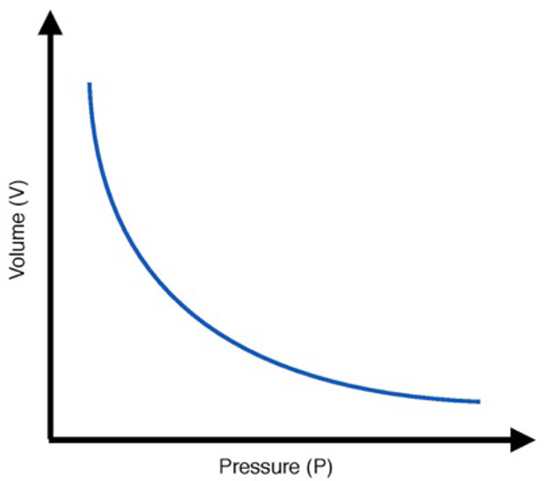
Figure 4: Boyles law
- Pneumoperiteum and intracranial air are relative contraindications to air transport. In a patient with intracranial air the volume expansion may worsen ICP and reduce cerebral perfusion.
- Equipment with air filled cuffs such as endotracheal tubes, Sengstaken–Blakemore tubes, stoma bags and inflatable pressure bags should have their pressures monitored. On ascent the volume expansion of air in the endotracheal cuff causes a rise in cuff pressure, the volume of air in the cuff will need to be reduced to maintain an appropriate pressure. On descent additional air will need to be added to the cuffs. Another option is to fill the endotracheal cuff with saline. Liquid expands much less than air.
Temperature
- As altitude increases the air temperature falls by 2°C for every 1000ft increase in altitude. Patients being transported at high altitude in aircraft without isolated cabins able to be pressurised and/or for long periods are at risk of hypothermia. As for land transfer appropriate measures to reduce heat loss should be used.
Humidity
- Dehydration occurs faster at higher altitudes due to lower air pressure and humidity, which causes more rapid evaporation of moisture from the skin and lungs. The significance of this is greatest for patients undergoing long transfers and these patients should have their input and output closely monitored to avoid hypovolaemia and dehydration.
- Reduced humidity can lead to thickened secretions and risk of mucous plugging, a heat moisture exchange filter (HMEF) or humidified oxygen via a facemask should be used.
- For extended transfers patient’s eyes should be lubricated with artificial tears and frequent mouth care is important.
Other considerations for air transport
Acceleration and deceleration
- Patients being transported by air be it helicopter or airplane will still be exposed to the same acceleration and deceleration forces as discussed above for land transfer. The only consideration is that the forces may be acting in a different axis due to the direction of travel and how the patient is orientated. The same considerations as mentioned above still apply.
Noise and vibration
- The noise and vibrations in a helicopter can be distressing for conscious patients especially if there is an element of delirium and this should be considered.
- The increased noise makes communication between the team difficult and is achieved via specialised headsets. The patient should also be provided with ear protection/headset.
- Vibration is the commonest cause of fatigue in medical personnel during helicopter flight and all team members should be alert to this risk. Air crews are subject to strict hours limitations to mitigate the risk of fatigue, and in the event of prolonged transfer the same degree of planning should be extended to accompanying medical staff.
- Vibration also affects monitoring equipment in particular non-invasive blood pressure cuffs that function via the oscillometric method. Patients who require accurate blood pressure monitoring should therefore have an arterial line inserted prior to transfer to allow more accurate blood pressure monitoring during flight.
Limited space
- Space is even more limited in helicopters than land ambulances. Intubation is extremely difficult if not impossible in a helicopter once in flight and so all patients at risk of deterioration should be intubated prior to transfer.
The above considerations are all important however, in practice many of the above complications may not be as significant as you might expect. This is because helicopters transferring patients pre-hospital or between hospitals typically fly at an altitude at 1,000ft. This reduces the effect of volume expansion and drop in partial pressure of oxygen.
Fixed wing aircraft are able to fly at much higher altitudes than helicopters but they are able to pressurise their cabin to lower altitudes unlike helicopters. Civilian aircraft typically set their cabin pressure at 7000-9000ft. Aircraft are able to pressurise their cabins to ‘ground level’ however this limits the altitude that aircraft are able to ascend to due to the pressure difference across the cabin walls.
Mode of Transport
As detailed above the different modes of transport can have very significant physiological effects on the body, especially in critically ill patients who are not able to compensate for these changes. The decision as to which mode of transport is used will be determined by location, urgency of transfer, availability of transport modes, weather and also patient factors.
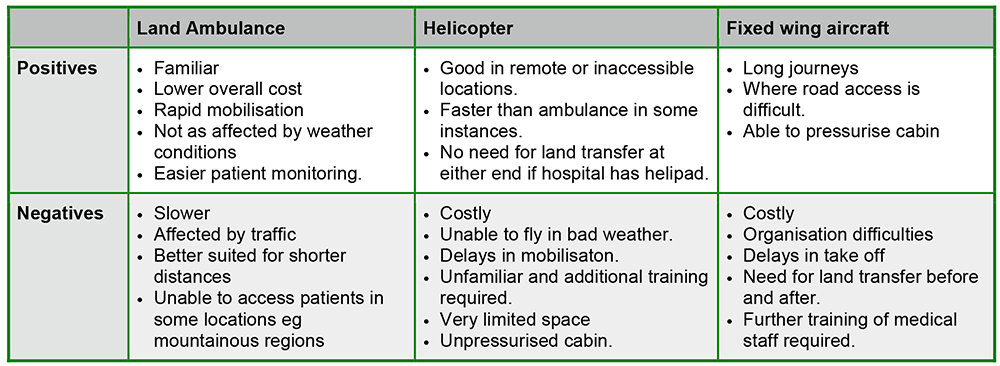
Figure 5: The positives and negatives for the different modes of transfer
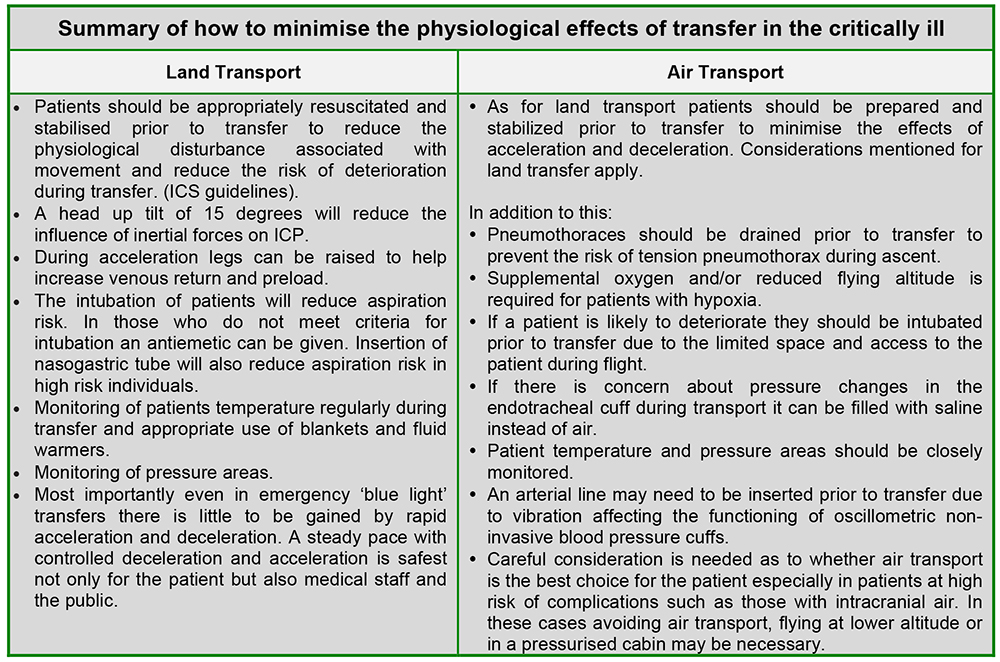
Summary
Patient transfer can have significant physiological effects that influence critically ill patients because critically ill patients are less able to compensate either due to their acute pathology or secondary to drug therapy.
Understanding the physiological impact that both land and air transfer has on the patient enables the patient to be prepared appropriately for transfer and will reduce risk of patient instability and deterioration during transfer.
It is vital to remember that the above principles not only apply to the patient but also to medical staff and equipment. Medical staff should ensure that they remain hydrated and aware to the risk of fatigue especially on long journeys. Monitoring equipment can be effected by vibration and indwelling devices filled with air such as endotracheal cuffs need to have their pressures monitored or be filled with saline during flight. All equipment is subjected to the force of inertia that can cause significant injury to staff if not secured properly.
Answers to questions
- ..
a. True – In an ambulance the external force causing deceleration is towards the patient’s feet. The inertial force acts in the opposite direction and causes displacement of blood and CSF towards the head, resulting in a rise in ICP.
b. True – During acceleration in an ambulance, the inertial force which opposes the acceleration results in the displacement of blood towards the patient’s feet. Blood will pool in the feet resulting in hypotension.
c. False – During deceleration there is an increased risk of aspiration due to the displacement of the stomach and its contents towards the patient’s head.
d. True – Ambulances are not able to regulate their temperature as well as heated buildings, exposing patients to cold environments. Patients under anaesthesia/sedation are not able to respond to dropping body temperature ie putting on more clothes and vasodilation causes increased loss of heat through redistribution of blood flow.
e. True – In patients with significant spinal injuries the inertial force acting during deceleration/acceleration results in axial loading, which can cause displacement of unstable spinal fractures. - ..
a. False – Boyles law states that at a constant temperature the volume of a given mass of gas varies inversely with the absolute pressure. Therefore, as you ascend the volume of any gas filled spaces will increase.
b. True – Saline does not expand as much as air during ascent and its volume is therefore less affected by altitude.
c. False – Space is limited in an ambulance but even more so when in a helicopter/aircraft, this makes accessing the patient challenging and intubation is often extremely difficult if not impossible once in flight.
d. False – The size (volume) of pneumothoraces increases with altitude due to gas expansion (Boyles Law), this increases the risk of the pneumothorax tensioning.
e. False – Air transport is not always the fastest method of transport due to delays in mobilisation, flight restrictions and in some cases need for land ambulance transfer to and from the airport/landing site. There are also risks associated with flying at altitude such as expansion of gas filled spaces and hypoxia, which are discussed in more detail in the article. - ..
a. False – Acceleration/deceleration and inertial forces also apply to equipment and medical personnel. For this reason equipment should be secured and all medical personnel should be sat down and secured with a seat belt during the transfer to reduce the risk of injury.
b. True – Newtons Third Law states that for every action there is an equal and opposite reaction.
c. False – Atmospheric pressure decreases with altitude due to the reducing effect of gravity on air molecules.
d. True – The fractional concentration of oxygen remains constant at 0.21 however the partial pressure of oxygen falls
e. True – This is the correct definition of Boyles Law.
References and further reading
- Intensive Care Society. Guidelines for the transport of the critically ill adult (3rd Edition 2011). (http://www.ics.ac.uk/icshomepage/guidelines-and-standards/)
- AAGBI Interhospital Transfer, AAGBI Safety Guideline (https://www.aagbi.org/sites/default/files/interhospital09.pdf)
- D Cleary, K Mackey. Inter-hospital transfers. Anaesthesia tutorial of the week, Intensive Care. Tutorial 319. 5th August 2015 http://resources.wfsahq.org/components/com_virtual_library/media/10ab57fa5fe491b831e42c0ca636e245-319-Inter-hospitaltransfers.pdf
- Critical care network, North West London. Critical care transfer training handbook.
- Pre-hospital Spinal Immobilisation: An Initial Consensus Statement. D Connor, K Porter, M Bloch, I Greaves. The Royal College of Surgeons of Edinburgh. https://fphc.rcsed.ac.uk/media/1764/pre-hospital-spinal-immobilisation.pdf
- I Macartney, P Nightingale. Transfer of the critically ill adult patient. British Journal of Anaesthesia CEPD reviews. 2001 Number 1.
- A Bersten, N Soni. OH’s Intensive Care Manual. Chapter 4 Transfer of critically ill patients. Pigs 27-37
- P Davis, G Kenny. Basic Physics and Measurement in Anaesthesia. Chapter 4 The Gas Laws. Pigs 37-50
- Traumatic Brain Injury (TBI) and Effects of Altitude: An Analysis of the Literature (http://hprconline.org/environment/altitude/traumatic-brain-injury-and-the-effects-of-altitude-pdf)
- USA Air Ambulance (http://www.usairambulance.net/effects-of-altitude.php)
- US Army Aviation Training Website https://rdl.train.army.mil/catalog-ws/view/100.ATSC/C696BACA-168F-4B4A-9750-BB445E08BECE-1300757497629/3-04.93/chap4.htm
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/