General Topics

KEY POINTS
- Point-of-care coagulation testing relies on the property of viscoelasticity. As blood clots, it becomes increasingly elastic.
- The 2 most used viscoelastic haemostatic assays are thromboelastography (TEG) and rotational thromboelastography (ROTEM). Both have their own terminologies.
- TEG and ROTEM provide the clinician with a holistic view of the clotting process from clot initiation and formation to a measure of clot stability and fibrinolysis.
- Conventional coagulation tests take longer to perform and do not provide a measure of platelet function or fibrinolysis.
- Viscoelastic assays may be used to guide resuscitation in major haemorrhage and in those situations in which coagulopathy is common.
- The use of viscoelastic assays may reduce blood product transfusion and improve patient outcomes; however, high-quality prospective evidence remains lacking.
INTRODUCTION
Point-of-care coagulation testing (POCCT) provides clinicians with the ability to rapidly evaluate the coagulation status of a patient in real time. POCCT offers several advantages over traditional coagulation assays. As a result, there is increasing interest in the use of POCCT in a variety of clinical settings including trauma, cardiac surgery, obstetrics, liver disease, and burns.1
Current POCCT relies on the principles of viscoelastic haemostasis, a technology first described by Dr Helmut Hartert in 1948.2 The 2 most used viscoelastic haemostatic assays (VHAs) today are thromboelastography (TEG, Haemonetics Corporation) and rotational thromboelastography (ROTEM, Werfen). This tutorial will introduce the concept of viscoelastic haemostasis and how it is used to generate meaningful measures of coagulation. We will discuss the advantages VHA offers over traditional coagulation assays and the current evidence supporting its use in guiding resuscitation and blood product transfusion.
VISCOELASTIC HAEMOSTATIC ASSAYS
Viscoelasticity refers to a material’s tendency to behave in both a viscous and elastic manner.2 Before clotting, whole blood will respond to shear stress with permanent deformation. The blood will not return to its original shape and can be thought of as viscous. Once clotting begins, blood becomes increasingly elastic, resisting shear stress to return to its original shape following deformation. The degree to which a material resists shear stress is referred to as the shear modulus.3 VHAs are concerned with observing the transition of blood from its viscous, unclotted state to its elastic, clotted state through measuring the shear modulus.
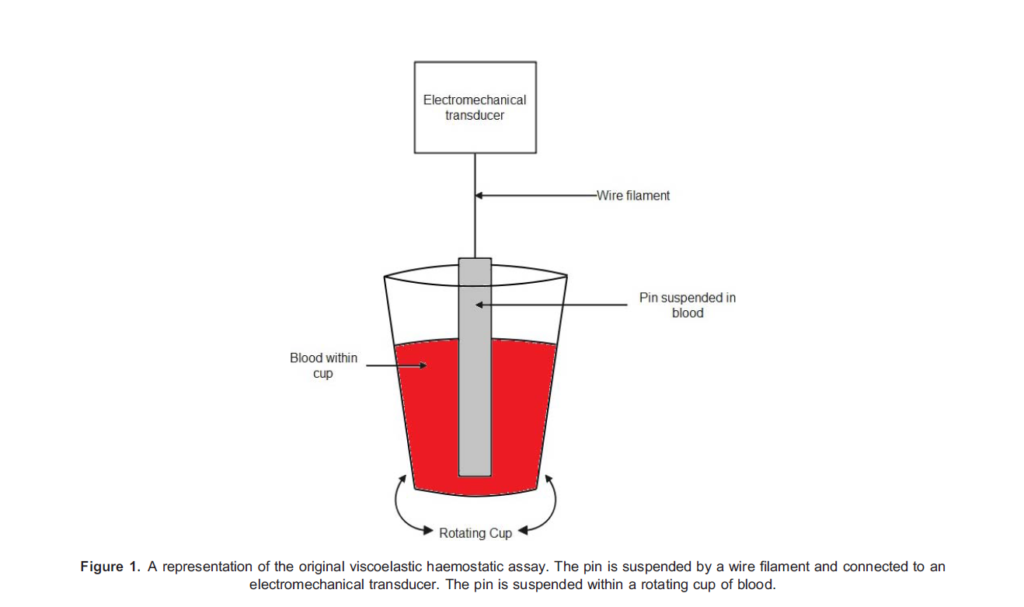
Dr Hartert’s original VHA consisted of a cup containing an activated blood sample. A pin was suspended on a wire within the sample (Figure 1). The test involved rotating the cup through 38, pausing, and then rotating back to its original position over 9
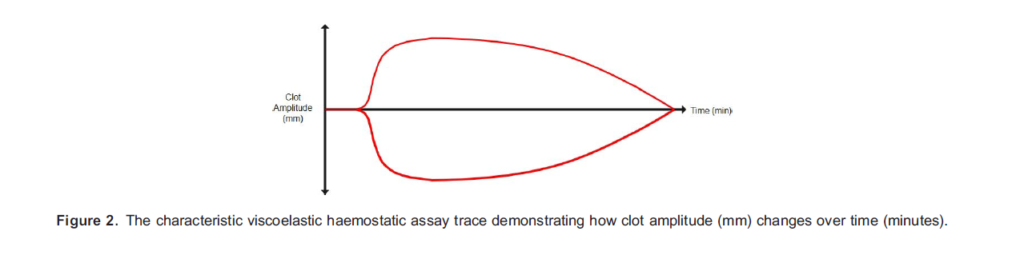
seconds. Shear stress is generated as the blood rotates around the pin. Prior to clotting, the whole blood responds to the shear stress with permanent deformation and no force is exerted on the pin. As the clot begins to form and becomes increasingly elastic, the blood will try to return to its original shape following shear stress. A force is therefore exerted on the pin, causing it to rotate. As the clot strengthens and elasticity increases, so does the rotation of the pin. The degree to which the pin rotates is plotted against time to produce a characteristic trace of developing clot strength. This provides clinicians with a visual representation of clot formation and lysis under shear stress (Figure 2).
TEG evolved from this original technique, employing the same pin and cup mechanism. In TEG the cup rotates around the pin in an arc of 4.758 every 5 seconds. As elasticity increases, a mechanical-electrical transducer converts the degree of rotation of the pin into the characteristic graphical representation of clot strength over time. The latest iteration of TEG (TEG 6s) subjects blood to vibration at a range of frequencies. As the blood’s viscoelastic property changes, so does its natural frequency and this property is used to observe clot formation over time.2
ROTEM is an adaptation of the original technique. Again, activated blood is placed in a cup containing a pin; however, here the pin is rotated within the cup. Prior to clot formation the pin rotates freely.2 As elasticity increases so does resistance to the rotation of the pin. Consequently, the arc of rotation of the pin decreases. A light-emitting diode shines onto a mirror attached to the pin, allowing for a visual representation of the developing clot’s strength over time.
The newest iterations of TEG (TEG 6s) and ROTEM (ROTEM Sigma) use a cartridge-based system, allowing both devices to run 4 assays simultaneously.2 Each assay focuses on a different aspect of the clotting process. TEG 6s requires the pipetting of citrated blood into the cartridge, while ROTEM Sigma operates off a vacutainer of citrated blood.
INTERPRETATION
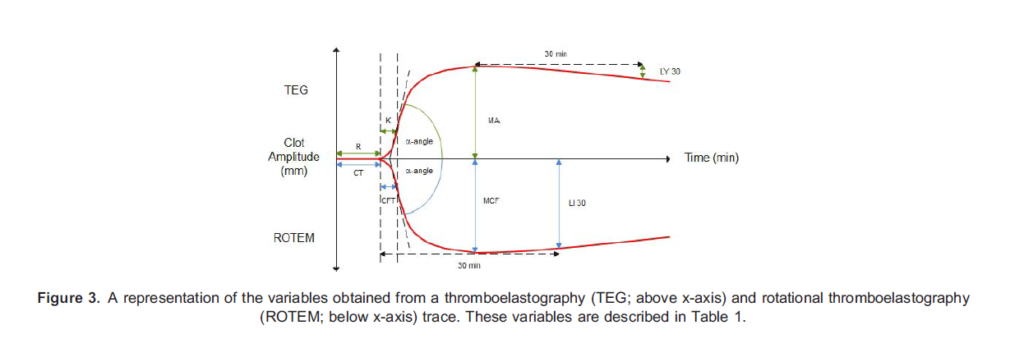
Despite the differing methods, both TEG and ROTEM generate similar information about clot formation and degradation. Figure 3 demonstrates the variables that are obtained from a TEG or ROTEM trace.
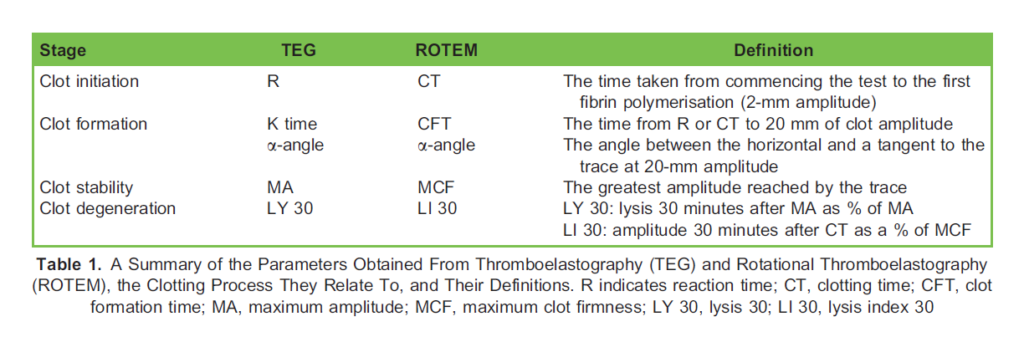
As seen in the above diagram TEG and ROTEM employ differing terminology for the same features of clotting. This is summarised in Table 1. The parameters can be thought of as relating to 4 stages of clotting: clot initiation, formation, stability, and degeneration.4
Clot initiation occurs in response to shear stress. The time taken to initiate a clot (reaction time or clotting time) is primarily dependent on clotting factors.3,4
- Prolonged clot initiation suggests clotting factor deficiencies or the presence of inhibitors such as heparin.
- Rapid clot initiation may suggest early disseminated intravascular coagulation (DIC).
Clot formation (K time, clot formation time, a-angle) is primarily dependent on fibrinogen polymerisation and, to some degree, platelet aggregation.3,4
- Prolonged clot formation therefore suggests hypofibrinogenaemia or thrombocytopenia.
- Rapid clot formation may indicate hyperfibrinogenaemia or early DIC.
Clot stability (maximum amplitude, maximum clot firmness) is a product of platelet number and function, and, to a lesser extent, fibrin strength.3,4
- Reduced stability suggests impaired platelet function, thrombocytopenia, or hypofibrinogenaemia.
- Excessive stability, on the other hand, suggests thrombocytosis or hyperfibrinogenaemia.
Clot degeneration (lysis 30 minutes after maximum amplitude) is an indication of fibrinolysis.3
- Degeneration may be accelerated in states of hyperfibrinolysis, such as tissue plasminogen activator release.
VHAs generate a holistic view of clot formation and breakdown in vitro. Specific abnormalities in the VHA trace provide the clinician with a rationale for guided management of the patient’s coagulation status.
STRENGTHS AND WEAKNESSES
When discussing the strengths and weaknesses of VHAs, it is useful to compare them to lab-based ‘conventional coagulation tests’ (CCTs). CCTs include the prothrombin time, a measure of the extrinsic coagulation pathway; activated partial thromboplastin time, a measure of the intrinsic pathway; Clauss fibrinogen; a measure of fibrinogen concentration and function; and platelet count.5
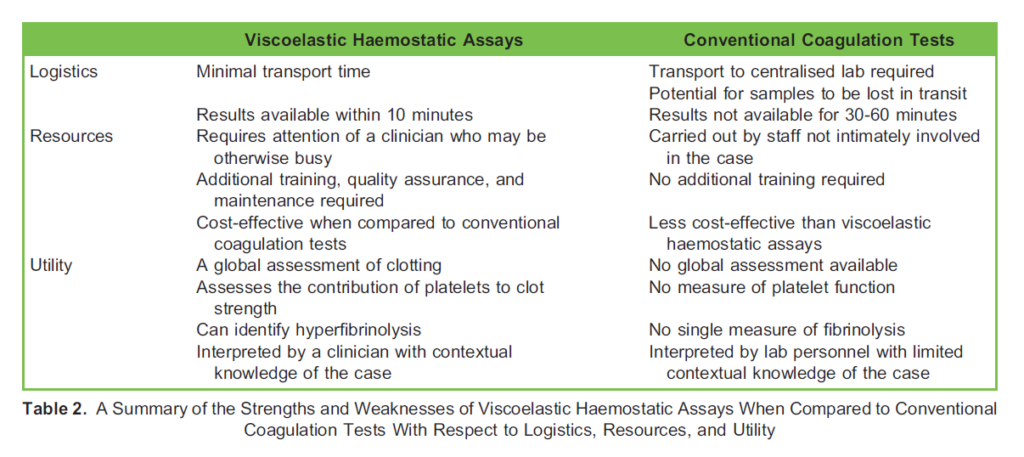
VHAs offer advantages from a logistical point of view. They can be carried out at the point of care, negating the need for transport to a centralised laboratory. This reduces the time taken to obtain a result with meaningful data to within 10 minutes of commencing the test.6 In addition to the time taken to reach the lab, CCTs also take longer to complete. In the context of ongoing haemorrhage, time is clearly an important factor. It should be noted that point-of-care prothrombin time is available, but no current point-of-care test exists for activated partial thromboplastin time, fibrinogen, or platelet count.7
When comparing the resources required, several considerations should be made. If VHAs are to be used at point of care, then the training of clinicians and allied health professionals in their use is required. Running and interpreting VHAs during major haemorrhages, which are generally stressful situations, adds a further demand on clinical personnel. VHA devices are themselves expensive and a significant investment. However, it should be noted that the material cost per ROTEM test is equivalent to that of a standard set of CCTs (£26 in 2013). Indeed, a report into cost effectiveness by the UK’s National Institute for Health Research concluded that VHAs are cost-saving when compared to CCTs.8
Regarding the assay itself, a criticism of CCTs is that they do not accurately represent the in vivo clotting process. CCTs test individual elements of the clotting pathway but do not provide a global assessment of function.7 Furthermore, no single CCT exists for measuring clot stability or fibrinolysis—both critical elements of a patient’s clotting status. Platelet count can be quickly ascertained, but gives no information on platelet function or contribution to clot firmness. In contrast, VHAs provide a real-time holistic view of the clotting process.6 The total strength and durability of clot can be ascertained and there is a measure of fibrinolysis. Specific assays in both TEG and ROTEM can isolate the contribution of platelets and fibrinogen to clot firmness, guiding clinicians in their use of blood products.6 These comparisons are summarised in Table 2.
A final weakness of VHAs is the limited body of evidence supporting their use. The ability of VHAs to rapidly detect abnormalities of coagulation has led to their use in major haemorrhage scenarios and situations in which coagulopathy is expected. As such, the British Society for Haematology has recommended their use in cardiac surgery, obstetrics, major trauma, liver disease, and transplant surgery.1 In contrast, in 2014 the National Institute for Health and Care Excellence stated that there is insufficient evidence to currently support their use in managing emergency bleeding in major trauma and obstetrics.9 The next section will address some of the existing evidence addressing the use of VHAs in these two settings.
APPLICATIONS
VHAs have a role in many aspects of clinical care. Their ability to rapidly detect abnormalities of coagulation has lent to their use in major haemorrhage scenarios, and situations in which coagulopathy is expected. As such, they have become increasingly used in cardiac surgery, liver disease and transplant surgery, and in monitoring the effects of anticoagulation medications.1 Here we will take a closer look at the evidence for their use in major trauma resuscitation and obstetric practice.
Major Trauma
Haemorrhage is responsible for up to 40% of mortality in major trauma.10 Trauma-induced coagulopathy, in conjunction with crystalloid resuscitation and environmental exposure, may further compound blood loss and haemodynamic instability. Prevention of trauma-induced coagulopathy has therefore become a focus of resuscitation in trauma management.
Evidence supporting the use of a VHA in major trauma resuscitation is largely observational. Studies have demonstrated a reduction in mortality and use of allogenic red cells when VHAs are used to guide resuscitation. Interestingly, there is evidence to suggest an increase in platelet transfusion and fibrinogen replacement with VHA use, inferring that non–VHA-based resuscitation may underestimate the requirement for these products.1
Evidence from randomised clinical trials is more conflicting. In 2016 a single-centre randomised clinical trials found an improvement in survival, with reduced plasma and platelet transfusion, with VHA-guided resuscitation.11 The multi-centre ITACTIC randomised clinical trials published in 2020 has cast doubt on the utility of VHA-guided trauma resuscitation. ITACTIC randomised major trauma patients (in whom empirical, balanced transfusion therapies had already been commenced) into a VHA protocol–assisted arm and a CCT protocol–assisted arm. Researchers did not demonstrate any benefit in short and longterm survival, or a difference in massive transfusion requirements between groups. However, the researchers did acknowledge that lower than expected rates of coagulopathy within the study population, likely due to empirical therapy already having been commenced, may have impacted the power of the study. There is a suggestion that VHA-guided resuscitation reduced mortality in those patients with traumatic brain injury.12
The British Society for Haematology has concluded that VHA may reduce mortality and transfusion exposure and if available should be considered for transfusion guidance in trauma haemorrhage.1
Obstetrics
At term, the mother is normally in a procoagulant state with elevated clotting factor and fibrinogen concentrations.1,13 As such, VHA-derived values for normal coagulation should be adapted in the obstetric population. Indeed, a normal, nongravid VHA trace in a parturient should prompt consideration of a developing coagulopathy.1
Thrombocytopenia complicates up to 10% of pregnancies.13 Traditionally, decisions about whether regional anaesthesia or analgesia is safe in the thrombocytopenic parturient have been based on a platelet count. A VHA gives clinicians more information about platelet function and clot stability and may help anaesthetists to make more informed decisions, particularly when considering neuraxial techniques.
VHA-guided management of obstetric haemorrhage has been demonstrated to reduce packed red cell, fresh frozen plasma, and platelet requirements while reducing the risk of circulatory overload.14 Outcomes have also been improved, with observational studies reporting reduced blood loss, rates of hysterectomy, and rates of critical care admission.15
The OBS-1 trial showed that women with postpartum haemorrhage and a VHA trace indicative of hypofibrinogenaemia were more likely to progress to severe postpartum haemorrhage and require blood product transfusion. In 2017 the OBS-2 trial identified ROTEM values for hypofibrinogenaemia below which fibrinogen replacement should be considered, and above which it does not appear necessary.16
These findings are reflected in the British Society for Haematology guidelines suggesting that VHAs may be used to manage postpartum haemorrhage as part of an institution’s local major obstetric haemorrhage protocol, particularly with respect to fibrinogen replacement.1
SUMMARY
Over the past 70 years viscoelastic assays have been refined into increasingly user-friendly devices that can provide the clinician with a rapid, holistic view of a patient’s coagulation function. Several devices exist with similar but potentially confusing terminology. VHAs have found use in a broad range of environments, but particularly those in which coagulopathy and major haemorrhage is widespread. Observational evidence backs up their utility in these situations, but large, prospective trials remain lacking.
REFERENCES
- Curry NS, Davenport R, Pavord S, et al. The use of viscoelastic haemostatic assays in the management of major bleeding. Br J Haematol. 2018;182(6):789-806.
- Hartmann J, Murphy M, Dias J. Viscoelastic hemostatic assays: moving from the laboratory to the site of care—a review of established and emerging technologies. Diagnostics (Basel). 2020;10(2):118.
- Schmidt AE, Israel AK, Refaai MA. The utility of thromboelastography to guide blood product transfusion: an ACLPS critical review. Am J Clin Pathol. 2019;152(4):407-422.
- Carll T, Wool GD. Basic principles of viscoelastic testing. Transfusion. 2020;60(S6):S1-S9.
- Stang LJ, Mitchell LG. Fibrinogen. In: Monagle P, ed. Haemostasis: Methods and Protocols. Totowa, NJ: Humana Press; 2013:181-192.
- Srivastava A, Kelleher A. Point-of-care coagulation testing. Cont Educ Anaesth Crit Care Pain. 2013;13(1):12-16.
- Cohen T, Haas T, Cushing MM. The strengths and weaknesses of viscoelastic testing compared to traditional coagulation testing. Transfusion. 2020;60(S6):S21-S8.
- Whiting P, Al M, Westwood M, et al. Viscoelastic point-of-care testing to assist with the diagnosis, management and monitoring of haemostasis: a systematic review and cost-effectiveness analysis. Health Technol Assess. 2015;19(58):1228, v-vi.
- National Institute for Health and Care Excellence. Detecting, managing and monitoring haemostasis: viscoelastometric point-of-care testing (ROTEM, TEG and Sonoclot systems). Accessed 21st January 2021. URL https://www.nice.org.uk/ guidance/dg13
- Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations, and therapeutic considerations. J Trauma. 2006;60(6 Suppl):S3-11.
- Gonzalez E, Moore EE, Moore HB, et al. Goal-directed hemostatic resuscitation of trauma-induced coagulopathy: a pragmatic randomized clinical trial comparing a viscoelastic assay to conventional coagulation assays. Ann Surg. 2016;263(6):1051-1059.
- Baksaas-Aasen K, Gall LS, Stensballe J, et al. Viscoelastic haemostatic assay augmented protocols for major trauma haemorrhage (ITACTIC): a randomized, controlled trial. Intensive Care Med. 2021;47(1):49-59.
- Waters JH. The role of viscoelastic testing in the management of the parturient. Transfusion. 2020;60(S6):S70-S74.
- McNamara H, Kenyon C, Smith R, Mallaiah S, Barclay P. Four years’ experience of a ROTEM(t) -guided algorithm for treatment of coagulopathy in obstetric haemorrhage. Anaesthesia. 2019;74(8):984-991.
- Snegovskikh D, Souza D, Walton Z, et al. Point-of-care viscoelastic testing improves the outcome of pregnancies complicated by severe postpartum hemorrhage. J Clin Anesth. 2018;44:50-56.
- Collins PW, Bell SF, de Lloyd L, Collis RE. Management of postpartum haemorrhage: from research into practice, a narrative review of the literature and the Cardiff experience. Int J Obstet Anesth. 2019;37:106-117.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/