Obstetrics Anaesthesia

Key Points
- Hypertensive diseases of pregnancy are still a common cause of maternal death.
- Pre-eclampsia complicates up to 8% of pregnancies in the developed world.
- Pre-eclampsia is associated with widespread endothelial dysfunction leading to placental ischaemia and multi-organ dysfunction.
- Magnesium Sulphate is the anticonvulsant of choice in prevention and treatment of eclamptic fits.
- The main concerns to the anaesthetist are those of an oedematous airway and dysfunction of the cardiorespiratory, cerebro-vascular and coagulation systems.
Introduction & Definitions
Hypertensive diseases of pregnancy are one of the most common direct causes of maternal death in the developed world. The largest single cause of death amongst women with pre-eclampsia and eclampsia in the United Kingdom is intra-cranial haemorrhage – reflecting a failure of effective anti-hypertensive therapy. HELLP syndrome associated with pre-eclampsia is another cause of death.
- Chronic hypertension can precede conception or it can occur in the first half of pregnancy. It can be classified as essential hypertension or hypertension secondary to a pathological process.
- Gestational hypertension occurs after 20 weeks gestation and returns to normal within three months of delivery. It has none of the other features of pre-eclampsia.
- Eclampsia (from the Greek Eklampsis – a sudden development) indicates the occurrence of seizures in a parturient who may have no underlying pathology.
- Pre-eclampsia is a complex multi-system disorder that may sometimes precede eclampsia.
The classical diagnostic triad for pre-eclampsia of hypertension, proteinuria and oedema is no longer considered useful. Oedema occurs in up to 80% of normotensive parturients and, conversely, pre-eclampsia can occur in the absence of proteinuria. There are several definitions of pre-eclampsia, but they generally involve hypertension occurring after 20 weeks with the involvement of at least one other organ system, for instance headache or epigastric pain. Hypertension in pregnancy is defined as a systolic pressure of >140 mmHg and /or a diastolic pressure of >90 mmHg. Mercury sphygmomanometry is the gold standard for blood pressure measurement and automated devices always need to be calibrated against this gold standard since they may significantly under-read.
Epidemiology
Hypertension affects 10% of all pregnancies and pre-eclampsia complicates approximately 2% – 8% in the UK. It is more common in the presence of a greater trophoblastic mass – for instance in multiple pregnancy or molar pregnancy. It also occurs more frequently in a woman who has previously suffered from pre-eclampsia. Other risk factors include diabetes, obesity, advanced age, nulliparity and a family history of pre-eclampsia. The presence of antiphospholipid antibodies and other autoimmune and chronic disease increase the likelihood of pre-eclampsia.
Aetiology
The exact aetiology of pre-eclampsia is unknown and probably complex. However, it only occurs in the presence of placental tissue and may be dependent on immunological and genetic factors.
The structure and function of the utero-placental circulation are consistently abnormal in pre-eclampsia. The normal conversion of the fibro-elastic spiral arteries of the nonpregnant uterus to the low-pressure high-flow circulation necessary for fetal well-being fails to occur. Subsequently the fetus will fail to grow and may even develop oligohydramnios. Evidence suggesting the presence of either of these two factors is a defining feature of severe pre-eclampsia.
Endothelial Dysfunction
In pre-eclampsia there is widespread endothelial dysfunction leading to placental ischaemia and multi-organ dysfunction. The endothelium is an important barrier that controls movement between the intra-vascular and extra-cellular compartments. It is also a highly active metabolic organ. Therefore, the synthesis of many substances including nitric oxide (NO) and prostacyclin (PGI2) may be decreased in pre-eclampsia. This leads to a major effect on smooth muscle reactivity and platelet adhesion.
Prophylaxis
The prevention of pre-eclampsia is still controversial. However, there is some evidence that anti-platelet drugs and calcium supplementation may reduce the risk of preeclampsia. Other dietary supplementations and interventions are of unknown effectiveness.
Pathophysiology
Cardiovascular and Respiratory function
Most authors consider that patients with pre-eclampsia are relatively vasoconstricted and hypovolaemic. However, the haemodynamic findings in pre-eclampsia are complex and vary widely between studies. It seems likely that with increasing severity of disease, there is progression to a more vasoconstricted hypovolaemic circulation with a lower cardiac output. Circulating catecholamines and administered vaso-active drugs may cause exaggerated responses.
Patients with pre-eclampsia are at risk of developing pulmonary oedema due to low colloid oncotic pressure and increased vascular permeability. They are also at risk of narrowing of the upper airways secondary to mucosal oedema.
Haematological
Coagulation changes in pre-eclampsia are well documented. Early in the disease process the hyper-coagulable state of normal pregnancy may be enhanced. Later on, both platelet activation and consumption are increased which can lead to significant thrombocytopenia (platelet count <100,000 mm-3) in approximately 15% of women with severe preeclampsia. DIC occurs in 7% of cases of severe pre-eclampsia.
Renal function
Renal tubular function deteriorates relatively early in pre-eclampsia – and the severity of the disease can be followed by measuring serial serum urate levels. The proteinuria of severe pre–eclampsia occurs later and reflects an ischaemic insult to the glomerulus. Normal individuals have an upper limit of proteinuria of about 100mg/day. In severe pre-eclampsia this may exceed 500mg/day. Patients rarely develop oliguria that is resistant to optimisation of the intravascular volume status.
Hepatic function
Abnormal liver function tests are frequently found in pre-eclampsia. More rarely, epigastric pain may be a symptom of tension on the capsule of the liver caused by oedema or intrahepatic haemorrhage. HELLP syndrome is the well-recognised association of Haemolysis, Elevated Liver enzymes and Low Platelets.
Neurologic changes
The neurological changes associated with severe pre-eclampsia include headaches, visual disturbances and hyper-reflexia. This may culminate with seizures (eclampsia). Cerebral vasospasm has been demonstrated by intra-cranial Doppler velocimetry in patients with pre-eclampsia and from MRI studies demonstrating reduced blood flow. Ischaemia due to vasospasm and/or cerebral oedema may be the cause of neurological symptoms.
Drug therapy
Drug therapy in pre-eclampsia is based on symptomatic organ support and prevention of complications. In the presence of severe pre-eclampsia , control of blood pressure and other measures of support should be undertaken if possible in a high dependency or intensive care setting. Delivery remains the only curative treatment for pre-eclampsia although the disease process may not resolve immediately.
Anti-hypertensives
Important considerations for the use of vasoactive drugs during pregnancy are the effects that they have on utero-placental flow and the fetus. The aim of anti-hypertensive treatment is to prevent maternal and fetal morbidity from labile hypertension. ACE inhibitors and angiotensin 2 antagonists are contraindicated before delivery because of their effects on the fetus.
Oral Anti-Hypertensive Agents
Methyl dopa is a centrally acting alpha2 agonist that has been extensively used as an antihypertensive in pregnancy. It has a number of common side effects including orthostatic hypotension, bradycardia, depression and drowsiness and may have important clinical interactions with any other CNS depressants and MAOIs.
Beta blockers such as labetalol and calcium channel blockers such as nifedipine are alternative treatments during pregnancy.
Intravenous agents
Hydrallazine is commonly used parenterally for the treatment of hypertensive emergencies during pregnancy. A labetalol infusion can be used to control blood pressure on its own or in combination with hydrallazine to counteract a tachycardia. Other intravenous agents such as nitrates and sodium nitroprusside have been used for severe refractory hypertension.
Magnesium
It is now accepted worldwide that Magnesium Sulphate (MgSO4) is the anticonvulsant of choice in preventing and treating eclamptic fits. Magnesium sulphate is usually administered as a slow intravenous bolus of 4 to 6grams and then as an infusion of 1 – 2 grams per hour to keep the serum Mg in the therapeutic range. MgSO4 is a safe drug to use in the pregnant patient but the most important effect of moderately high levels is its effect on the neuromuscular junction. MgSO4 may also increase the likelihood of hypotension during regional anaesthesia and will tend to blunt the response to vasoconstrictors. Treatment of overdose is supportive in the first instance and also includes intravenous calcium (e.g. Calcium gluconate 1g). Magnesium therapy is often continued for at least 24 hours post partum.
Clinical indicators of magnesium toxicity include the absence of tendon reflexes and decreased respiratory rate. ECG changes occur (P–Q interval prolonged, QRS complex widened) which may progress to conduction defects and cardiac arrest. The risks increase in the presence of oliguria since magnesium depends the kidneys for excretion.
Pre-anaesthetic assessment
Fluid balance & Haemodynamics
The presence of hypo-albuminaemia, increased capillary permeability and a high hydrostatic pressure (from the hypertension) leads to the risk of pulmonary and pharyngolaryngeal oedema. However, judicious administration of fluid may be necessary to avoid the pre renal oliguria that is common with pre-eclamptic patients. With adequate treatment it is rare these days for the oliguria to proceed to chronic renal dysfunction. It is recommended for each department to have a protocol to guide the treatment of these patients in a consistent way. Invasive monitoring of the central venous pressure and arterial blood pressure may provide useful information to guide management. Estimation of cardiac output can be considered in the setting of oliguria, pulmonary oedema or hypertension resistant to initial therapy. Frusemide may be used to treat persistent oliguria in the presence of an adequately filled circulation.
Coagulation
Assessment of the coagulation status of the blood is essential before regional anaesthesia, particularly in severe pre-eclampsia. Thrombocytopenia is a common corollary to severe pre-eclampsia but there is no absolute level of platelet count that accurately predicts the occurrence of bleeding associated with regional anaesthesia. If the platelet count is less than 80,000 mm-3 then further assessment of the coagulation status is justified. The results of the PT, APTT and perhaps thromboelastography can be compared with the normal range for pregnant patients.
Epidural analgesia
Early epidural analgesia is an ideal form of pain relief during labour in a pre-eclamptic patient. It helps to control the exaggerated hypertensive response to pain and can also improve the placental blood flow in these patients. A functioning epidural may safely be extended for caesarean section.
The block should be developed slowly with a weak solution of local anaesthetic and opiate and the blood pressure measured frequently for at least the first 20 minutes. Should hypotension occur, despite these precautions, it should be treated with a fluid bolus and adoption of the full lateral position by the patient. Vasoactive hypertensive agents may be necessary but should be used cautiously bearing in mind the sensitivity of some pre-eclamptic patients to them.
Anaesthesia for Caesarean section
The advantages of regional over general anaesthesia for Caesarean section include avoidance of the hypertensive response to laryngoscopy (which is pronounced in preeclamptic women), a blunting of the neuro-endocrine response to surgery and prevention of the transient neonatal depression associated with general anaesthesia. The relative merits of epidural versus spinal anaesthesia are hotly debated. A spinal is quicker and more reliable in onset and involves less potential trauma in the epidural space. However, the disadvantages include the theoretical risk of a more abrupt hypotension in a patient who may be relatively hypovolaemic and with a fetus who may be compromised by placental insufficiency. Recent studies have demonstrated the safety of spinal anaesthesia in pre-eclampsia. Alternatively, a combined spinal epidural approach can be used with a limited dose of local anaesthetic in the sub arachnoid space and the option of utilising the epidural as necessary.
General anaesthesia may be necessary and so difficult intubation should be prepared for meticulously (it being impossible to predict consistently). The main concerns are of mucosal oedema of the upper airway and the severe hypertensive responses to laryngoscopy and surgery. It is important that the obstetric intubation trolley has a range of endotracheal tubes down to a size 5.5 internal diameter and a variety of laryngoscopes and other aids to securing the airway. Drugs used to attenuate the hypertensive response to laryngoscopy include the pre-induction use of magnesium, labetalol, nitrates, nitroprusside, lidocaine and/or potent parenteral opioids. Patients on magnesium may be very sensitive to the effects of non-depolarising neuromuscular blocking drugs.
Summary
Pre-eclampsia is a heterogeneous multisystem disorder of pregnancy. Controversies still exist with regard to its aetiology, diagnosis and treatment. Careful control of the blood pressure in a high dependency setting is paramount. The main concerns to the obstetric anaesthetist are those of the potential problems with the airway and the effects of organ dysfunction particularly those of the cardiorespiratory, cerebral and coagulation systems.
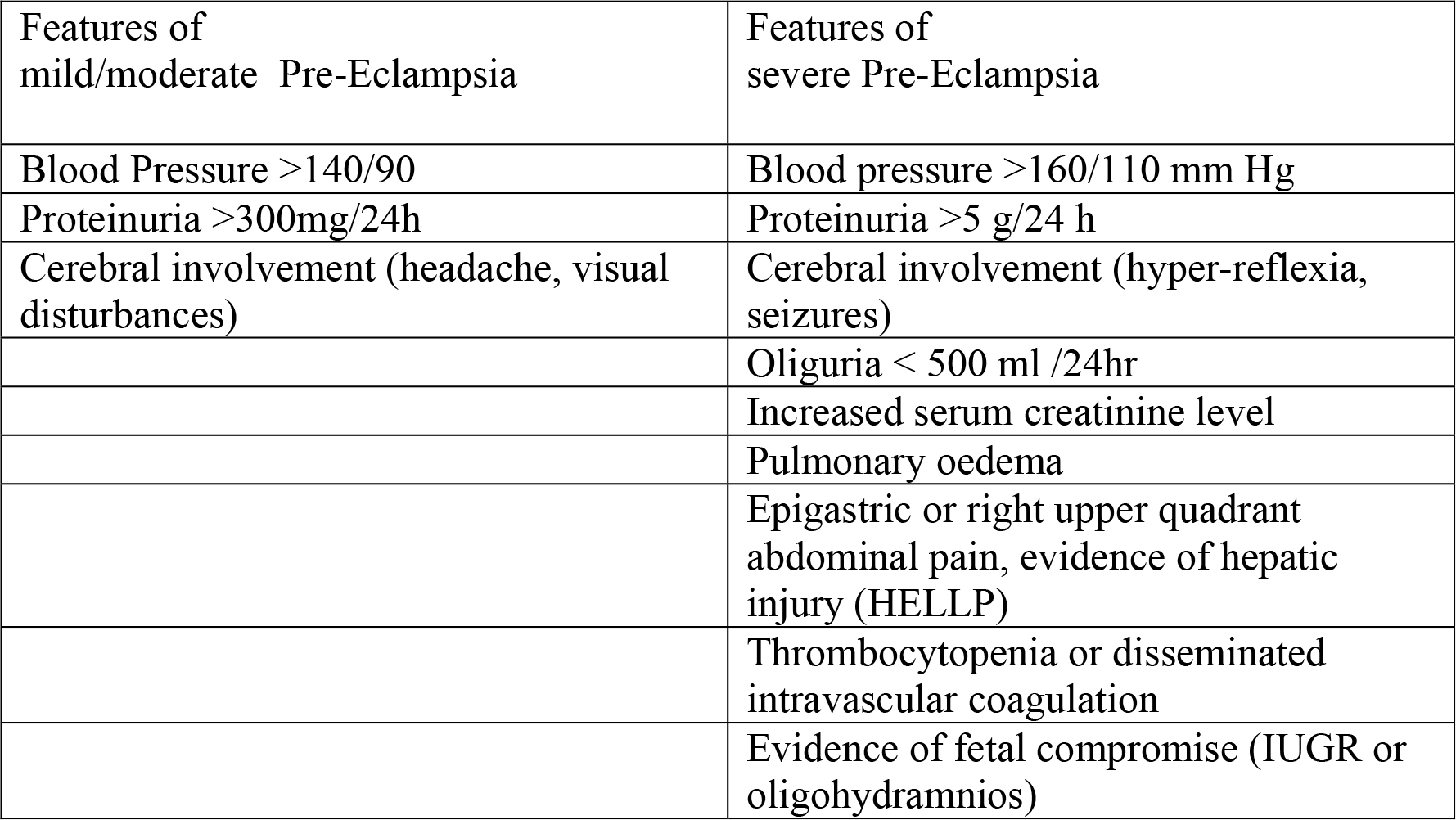
Table 1 Severity of Pre-Eclampsia
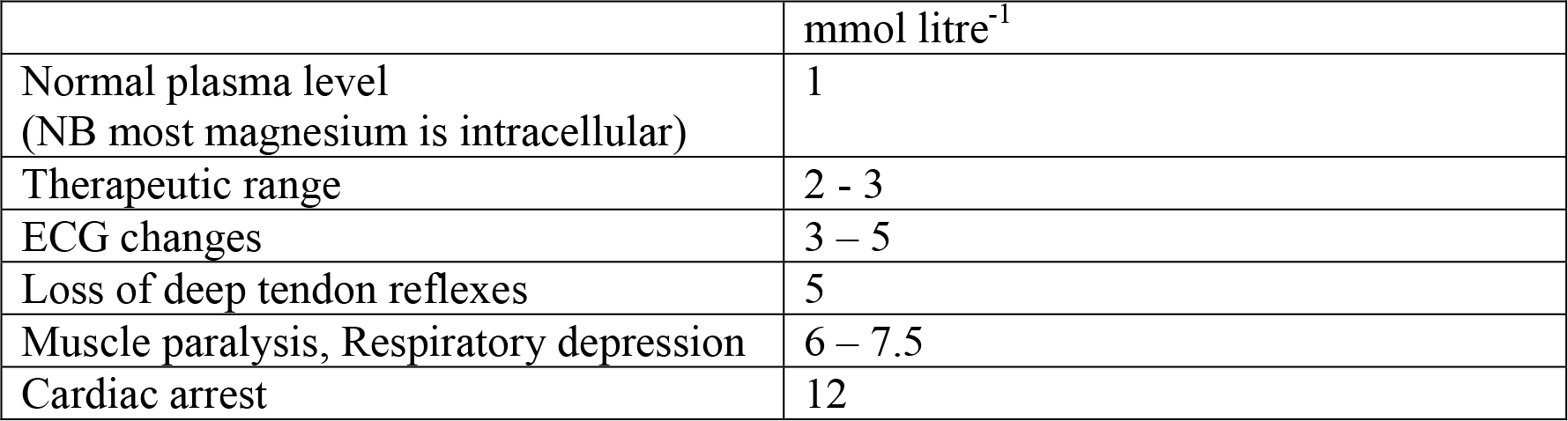
Table 2 Effects of rising plasma magnesium level
Suggested references.
- Duley L, Farrell B et al Do women and their babies benefit from magnesium sulphate? The Magpie trial : a randomised placebo controlled trial. Lancet 2002; 359: 1877 – 90
- Why Mothers Die 1997 – 1999. The Confidential Enquiry into Maternal Deaths in the United Kingdom. RGOG Press, London
- The Confidential Enquiry into Maternal and Child Health (CEMACH) 2000 – 2002 http://www.cemach.org.uk/publications.htm
- Brodie H and AM Malinow. Anesthetic management of pre-eclampsia/eclampsia. Int J Obstet Anesth 1998, 8:110-124.
- Chestnut DH: Obstetric Anesthesia – Principles and Practice. Mosby Inc: St. Louis. (2nd Ed.)1999 chapter 44
Multiple Choice Questions
- In pre-eclamptic parturients, magnesium sulphate is likely to
- decrease maternal heart rate
- prolong the effects of non depolarising muscle relaxants
- decrease succinyl choline induced fasciculations
- prevent hypokalaemia
- produce fetal bradycardia
- Regarding features of Eclampsia/ Pre-Eclampsia;
- General oedema is a useful diagnostic feature
- Pre-eclampsia always precedes eclampsia
- A blood pressure of 160/110 gives a diagnosis of severe pre-eclampsia
- Thrombocytopenia is a common finding in pre-eclampsia
- The use of spinal anaesthesia is absolutely contra-indicated
- A 25 year old woman is receiving magnesium for eclampsia at 36 weeks gestation. Each of the following is a potential maternal effect of this treatment
- sedation
- sensitisation to depolarising muscle relaxants
- sensitisation to non depolarising muscle relaxants
- decreased uterine blood flow
- loss of deep tendon reflexes prior to significant cardiac dysrhythmia
- Two hours after delivery a healthy multiparous woman has a grand mal seizure that is initially controlled with intravenous diazepam. Subsequent management may include
- magnesium sulphate
- lithium
- anti-hypertensives
- diuretics
- intravenous twice normal saline
- HELLP syndrome is characterised by the following features
- Fatty liver
- Thombocytopenia
- Pelvic pain
- Haemolysis
- Abnormal renal function
MCQ Answers
- Question 1
- (a) False (b) True (c) True (d) False (e) False
- (a,e) Magnesium does slow the rate in an isolated heart. However, this effect does not occur physiologically due to decreased acetyl choline release by the vagus in the presence of a raised serum magnesium. (b,c) Magnesium will decrease the release of acetyl choline at the neuromuscular junction and thereby prolong both non-depolarizing and depolarising block. (d) Magnesium has diuretic actions but may be useful in arrythmias associated with hypokalaemia. Miller 5th Edition
- Question 2
- (a) False (b) False (c) True (d) False (e) False
- (a) Oedema occurs in up to 80% of normotensive parturients whereas pre-eclampsia complicates less than 10% of pregnancies. (b) An eclamptic fit may occur without preceding symptoms and signs of pre-eclampsia. (c) By definition. (d) Thrombocytopenia is one part of HELLP syndrome together with haemolysis and elevated liver enzymes. (e) Opinions differ
- Question 3
- (a) True (b) True (c) True (d) False (e) True
- (a,b,c,e) All known effects of increasing magnesium levels. (d) Magnesium is a vasodilator.
- Question 4
- (a) True (b) False (c) True (d) True (e) False
- (a,c,d) Magnesium, anti-hypertensives and diuretics may all be utilized in management of eclampsia and pre-eclampsia.
- Question 5
- (a) False (b) True (c) False (d) True (e) False
- (a – e) HELLP syndrome is Haemolysis, Elevated Liver enzymes and Low Platelets
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/