General Topics

QUESTIONS
Before continuing, try to answer the following questions regarding aspiration during anaesthesia. The answers can be found at the end of the article, with explanations.
True or false?
- Those patients who suffer from gastro-oesophageal reflux are at greatest risk of aspiration
- Gastric emptying for all solids occurs within 6 hours
- Cricoid pressure applied at 30 N compresses the oesophagus in 90% of patients
- Pre-emptive antibiotic therapy is recommended
- Mortality in those who develop symptoms is approximately 10%
INTRODUCTION
Aspiration was first recognised as a cause of an anaesthetic-related death in 1848 by James Simpson. Much later in 1946, Mendelson described the relationship between aspiration of solid and liquid matter, and pulmonary sequelae in obstetric patients. Today it remains a rare but potentially devastating complication of general anaesthesia, quoted as occurring in between 1 in 3000 and 1 in 6000 anaesthetics. This increases to 1 in 600 for emergency anaesthesia in adults.
Aspiration can be defined as the inhalation of material into the airway below the level of the true vocal cords. It is linked with a range of clinical outcomes, being asymptomatic in some instances and resulting in severe pneumonitis and ARDS in others. This tutorial will cover the pathophysiology and predisposing factors, and go on to discuss prevention and management.
PATHOPHYSIOLOGY
The lower oesophageal sphincter (LOS) is functionally distinct from the oesophagus, and acts as a valve preventing the reflux of gastric contents. Barrier pressure is the difference between LOS pressure (normally 20-30mmHg) and intragastric pressure (normally 5-10mmHg) and both are influenced by a number of factors. LOS pressure is reduced by peristalsis, vomiting, during pregnancy (a progesterone effect) as well as pathological conditions such as achalasia, and various drugs (anticholinergics, propofol, thiopentone, opioids). Intragastric pressure is increased if the gastric volume exceeds 1000ml, and with raised intra-abdominal pressure such as that occurring with pneumoperitoneum during laparoscopy. The resulting drop in barrier pressure may increase the risk of aspiration, although it should be pointed out that studies have shown a concomitant increase in LOS pressure in anaesthetised patients undergoing laparoscopy, thus maintaining barrier pressure.
Gastric volume is influenced by the rate of gastric secretions (approx 0.6ml/kg/hr), swallowing of saliva (1ml/kg/hr), ingestion of solids/liquids, and the rate of gastric emptying. The rate of gastric emptying for non-caloric clear fluids is rapid – the half-time being about 12 minutes. Solids however, require six hours or more to be cleared from the stomach, displaying zero-order kinetics. Altered physiological states such as pregnancy, labour, abdominal pain, gastrointestinal orders, renal failure and diabetes will alter the rate of gastric emptying, as well as drugs such as opioids.
PREDISPOSING FACTORS
As suggested above, patients at greatest risk are those undergoing unplanned surgery, but also inadequate level of anaesthesia, those with abdominal pathology or the obese. Other examples are found below:
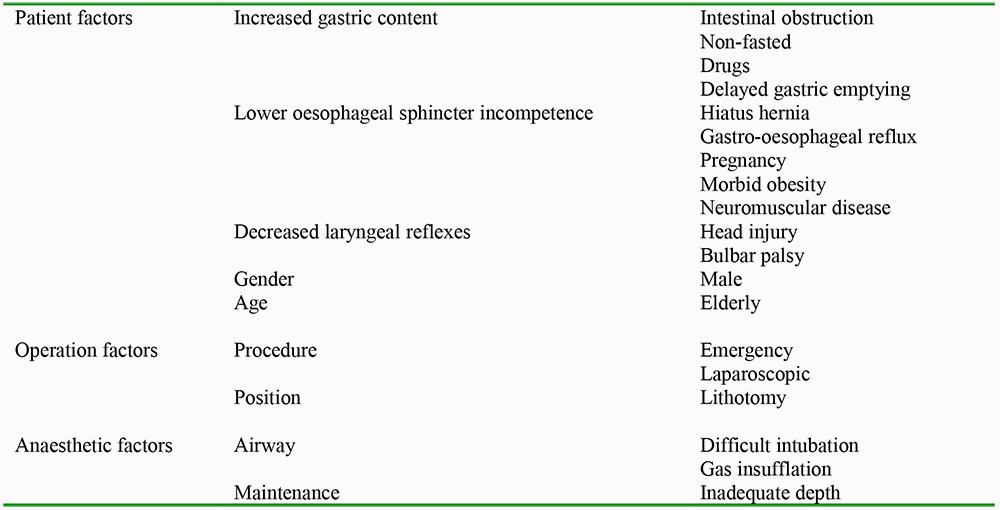
Table 1: Predisposing factors for aspiration under general anaesthesia
CLASSIFICATION
Aspiration pneumonitis
Known as Mendelson’s syndrome, as described by the obstetrician in 1946, this condition involves lung tissue damage as a result of aspiration of non-infective but very acidic gastric fluid. This usually occurs in two phases – firstly desquamation of the bronchial epithelium causing increased alveolar permeability. This results in interstitial oedema, reduced compliance and VQ mismatch. The second stage, occurring within 2 to 3 hours, is due to an acute inflammatory response, mediated by proinflammatory cytokines such as tumour necrosis factor alpha and interleukin 8 and reactive oxygen products. Clinically, this may be asymptomatic, or present as tachypnoea, bronchospasm, wheeze, cyanosis and respiratory insufficiency.
Aspiration pneumonia
This occurs either as a result of inhaling infected material or secondary bacterial infection following chemical pneumonitis. It is associated with typical symptoms of pneumonia such as tachycardia, tachypnoea, cough and fever, and may be evidenced by segmental or lobar consolidation (classically right middle lobe) on chest radiography. The disease process is similar to a community acquired pneumonia although the complication rate is higher, with cavitation and lung abscess occurring more commonly.
Particulate-associated aspiration
If particulate matter is aspirated, acute obstruction of small airways will lead to distal atelectasis. If large airways are obstructed, immediate arterial hypoxaemia may be rapidly fatal.
PREVENTION
Preoperative fasting
The commonly quoted figures of a critical volume of 25ml of aspirate, with a pH < 2.5 being sufficient to cause aspiration pneumonitis are derived from unpublished work by Roberts and Shirely on Rhesus monkeys, and extrapolated to humans. In fact 50% of fasted patients have a residual gastric volume exceeding this, with an average pH of around 2.0. Unnecessarily prolonged nil by mouth (NBM) orders lead to dehydration and possibly hypoglycaemia, with resultant thirst, hunger, discomfort and irritability. Current guidelines are 2 hours for clear fluids, 4 hours for breast milk, and 6 hours for a light meal, sweets, milk (including formula) and non clear fluids.
Reducing gastric acidity
Histamine (H2) antagonists and proton pump inhibitors (PPIs) are commonly used to increase gastric pH, although they do not affect the pH of fluid already in the stomach. Oral sodium citrate solution reliably elevates gastric pH above 2.5, but it increases gastric volume, and is associated with nausea and vomiting. H2 antagonists act by blocking H2 receptors of gastric parietal cells, thereby inhibiting the stimulatory effects of histamine on gastric acid secretion. PPIs on the other hand, block the ‘proton pump’ of the same cell, inhibiting the stimulatory actions of histamine, gastrin and acetylcholine. An oral H2 antagonist must be given 1-2 hours before anaesthesia, and a PPI, 12 hours in advance. A recent meta-analysis by Clark et al suggested that ranitidine was superior to PPIs in both reducing gastric fluid volume and acidity. Its use is recommended in patients at risk of aspiration only, not routinely. Metoclopramide has a prokinetic effect promoting gastric emptying, but there is little evidence to support its use. It does however, remain part of the usual pre-medication for Caesarean section under general anaesthetic.
Rapid Sequence Induction (RSI)
It has been shown that most cases of aspiration occur on induction and laryngoscopy, hence the following is of the utmost importance. For patients at high risk of aspiration, a RSI is the induction of choice unless presented with a sufficiently difficult airway to warrant an awake fibreoptic intubation. The patient should be on a tilting trolley, with suction to hand. Three minutes of pre-oxygenation precede the administration of an induction agent, cricoid pressure (discussed below) and the rapidly acting muscle relaxant succinylcholine. This avoids the need for bag-mask ventilation and the possibility of gastric insufflation. Adequate depth of anaesthesia is important to avoid coughing, laryngospasm and vomiting. Cricoid pressure is not released until confirmation of appropriate placement of the tracheal tube with the cuff inflated.
Cricoid pressure
First described by Sellick in 1961, cricoid pressure remains an essential manoeuvre performed as part of RSI despite significant controversy. The aim is to compress the oesophagus between the cricoid ring cartilage and the sixth cervical vertebral body thus preventing reflux of gastric contents. The force recommended is 30N, or that required to close the oesophagus without distorting the airway. This latter complication is the greatest limiting feature of the manoeuvre, causing malalignment, distortion of the cricoid ring and possible closure of the vocal cords. Even when applied correctly there is doubt as to its efficacy, simply causing anatomical displacement of the oesophagus in some people, and non compression in others. In addition, manometry studies have shown it to reduce LOS tone thus reducing barrier pressure. Cricoid pressure should be released in the case of active vomiting to avoid oesophageal rupture.
Nasogastric tube placement
Patients for emergency theatre with intestinal obstruction frequently have a nasogastric tube in situ. There is evidence from cadaver studies that this does not alter the efficacy of cricoid pressure. Furthermore it can be useful to empty the stomach before induction of anaesthesia. Studies have shown that there is no significant difference between the incidence of gastroesophageal reflux with large or small bore tubes.
Airway device
A cuffed endotracheal tube is considered the gold standard device used for airway protection. However, it has disadvantages – cardiovascular and respiratory instability, postoperative hoarseness, sore throat, increased length of stay in recovery to name but a few. It has also been suggested that microaspiration of secretions occuring between the cuff and tracheal mucosa plays a role in ventilator acquired pneumonia. Alternative supraglottic devices include the classic Laryngeal Mask Airway (LMA) and the Proseal LMA, the latter providing a higher seal pressure (up to 30cmH20) and a drainage channel for gastric contents. These have excellent safety records, and can be used for positive pressure ventilation although the main contraindication to their use is an increased risk of regurgitation.
Emergence
It should be remembered that those patients at risk of aspiration on induction are similarly at risk on emergence. Care should be taken to ensure that their airway reflexes have fully returned before extubation occurs.
MANAGEMENT
Initial management
Initial management involves the recognition of aspiration by way of visible gastric contents in the oropharynx, or more subtle indications such as hypoxia, increased inspiratory pressure, cyanosis, tachycardia or abnormal auscultation, when a list of differentials must be thought through.
Differential diagnosis
- Bronchospasm
- Laryngospasm
- Endotracheal tube obstruction
- Pulmonary oedema
- ARDS
- Pulmonary embolism
Once the diagnosis is suspected, the patient should be positioned head-down to limit pulmonary contamination, and suctioning performed to clear the oropharynx. Some advocate the left lateral position if feasible, but if unfamiliar with managing the airway in this position, then Trendelenburg is indicated. Oxygen (100%) must be administered, followed by immediate RSI and securing of the airway with an endotracheal tube. At this point, tracheal suctioning should ideally precede positive pressure ventilation to avoid any aspirate being forced further down the bronchial tree. Positive end- expiratory pressure is useful at about 5cmH2O, and early bronchoscopy is recommended if aspiration of particulate matter is suspected to prevent distal atelectasis. Symptomatic treatment of bronchospasm with bronchodilators may be necessary.
Management: key points
- Head down tilt
- Oropharyngeal suction
- 100% oxygen
- Apply cricoid pressure and ventilate
- Deepen anaesthesia/perform RSI
- Intubate trachea
- Release cricoid once airway secured
- Tracheal suction
- Consider bronchoscopy
- Bronchodilators if necessary
A clinical decision between the anaesthetist and surgeon must then be made on whether or not to proceed with surgery. This will depend on the underlying health of the patient, the extent of the aspiration, and urgency of the surgical procedure.
A chest x-ray (CXR) can be useful in the case of suspected pulmonary aspiration, although in about 25% of cases there are no radiographic changes initially.
If stable enough for extubation, patients should be observed carefully and those that are asymptomatic 2 hours post-operatively may be discharged from the recovery area. It is suggested that those that develop a new cough/wheeze, are tachycardic or tachypnoeic, drop their SpO2 on room air (by >10% of pre-operative value) or have new pathological changes on CXR should be further managed in an ICU setting.
Further treatment
Empirical antibiotic therapy is strongly discouraged unless it is apparent that the patient has developed a subsequent pneumonia, as occurs in 20-30%. Treatment should then ideally only be prescribed once the organism has been identified, most commonly gram negative bacilli. Inappropriate administration has been linked to ventilator-associated pneumonia with virulent organisms such as Pseudomonas aeruginosa and Acinetobacter.
Corticosteroids should not be given prophylactically in the acute phase following aspiration, as there is no evidence to support a reduction in the inflammatory response. They may even have an adverse effect on mortality in critically ill patients.
SUMMARY
Aspiration is a relatively rare, but potentially fatal complication of general anaesthesia occurring most commonly in emergency patients, those at light level of anaesthesia or with intra-abdominal pathology. The spectrum of symptoms ranges from nil, to severe respiratory compromise and death, and may be due to either a chemical pneumonitis or secondary pneumonia.
Prevention is the key, and there are several mandatory requirements that must be fulfilled in the at-risk patient. However, in the event of aspiration occurring, treatment is essentially supportive once the airway has been secured.
ANSWERS
- False. Those patients undergoing emergency surgery are at greatest risk
- False. It may take 9 hours or more for a substantial meal to be emptied from the stomach. The impact of trauma on gastric emptying is ill-defined but should be taken into account, as should medications and co-morbidities.
- False. The efficacy of cricoid pressure is unclear, although it remains part of a RSI
- False.
- True. Studies suggest that approximately 2/3 of patients who have aspirated are asymptomatic at 2 hours, and require no further intervention. Of the 1/3 who develop respiratory symptoms, a number will require non invasive or mechanical ventilation and around 10% will die. Those that are ventilated for more than 48 hours post aspiration have a 50% mortality rate.
REFERENCES and FURTHER READING
- Ng A, Smith G. Gastroesophageal reflux and aspiration of gastric contents in anesthetic practice. Anesth Analg 2001; 93: 494-513 www.anesthesia analgesia.org/content/93/2/494.full
- Benington S, Severn A. Preventing aspiration and regurgitation. Anaesthesia and Intensive Care 2007; 8:9
- Bernardini A, Natalini G. Risk of pulmonary aspiration with laryngeal mask airway and tracheal tube: analysis on 65 712 procedures with positive pressure ventilation. Anaesthesia 2009; 64: 1289-1294
- Clark K, Lam L, Gibson S, Currow D. The effect of ranitidine versus proton pump inhibitors on gastric secretions: a meta-analysis of randomised control trials. Anaesthesia 2009; 64: 652-7
- Janda M, Scheeren T, Noldge-Schomburg G. Management of pulmonary aspiration. Best Practice & Research Clinical Anaesthesiology Vol. 20, 3: 409-427
- Kalinowski C, Kirsch J. Strategies for prophylaxis and treatment for aspiration. Best Practice & Research Clinical Anaesthesiology Vol.18, 4: 719-737
- Mendelson CL. The aspiration of stomach contents into the lungs during obstetric anaesthesia. American Journal of Obs & Gynae 1946; 52: 191
- Rawlinson E, Minchon A. Pulmonary Aspiration. Anaesthesia and Intensive Care Medicine 2007; 8: 9
- Scarlett M, Crawford-Sykes A, Nelson M. Preoperative starvation and pulmonary aspiration. West Indian Med J 2002; 51 (4): 241-5
- Simpson JY. The alleged case of death from the action of chloroform. Lancet 1848; 1: 175-
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/