General Topics

The WFSA has been working on information about pulse oximetry and the following tutorial is part of the material. Feedback would be very useful and should be sent to iain.wilson@rdeft.nhs.uk
Pulse oximetry is used every day in our theatres and recovery areas. How much do you know about how an oximeter works – before reading the tutorial, we would like you to assess your knowledge about pulse oximetry. The correct answers are in the next section.
- How is oxygen transported from the atmosphere to the tissues?
- What is the normal oxygen saturation in arterial blood?
- What is preoxygenation?
- A patient undergoing general anaesthesia for hernia repair has an oxygen saturation of 82% during surgery. Is this reading high or low? Is any action required?
OXYGEN
Human beings depend on oxygen for life. All organs require oxygen for metabolism but the brain and heart are particularly sensitive to a lack of oxygen. Shortage of oxygen in the body is called hypoxia. A serious shortage of oxygen for a few minutes is fatal.
During anaesthesia, patients’ airways may become obstructed, their breathing may become depressed, their circulation may be affected by blood loss or an abnormal heart rhythm or the anaesthetic equipment may develop a problem such as an accidental disconnection or obstruction of the breathing circuit. These factors can result in a reduction of oxygen delivery to the tissues which, if not managed correctly, could lead to death or injury. The earlier the anaesthesia provider detects a problem, the sooner it can be treated so that no harm comes to the patient.
OXYGEN TRANSPORT TO THE TISSUES
Oxygen is carried around the body attached to an iron-containing protein called haemoglobin, (Hb) contained in red blood cells. After oxygen is breathed into the lungs, it combines with the haemoglobin in red blood cells as they pass through the pulmonary capillaries. The heart pumps blood continuously around the body to deliver oxygen to the tissues.
There are five important things that must happen in order to deliver enough oxygen to the tissues:
- Oxygen must be breathed in (or inspired) from the air or anaesthesia circuit into the lungs.
- Oxygen must pass from the air spaces in the lung (called the alveoli) to the blood. This is called alveolar gas exchange.
- The blood must contain enough haemoglobin to carry sufficient oxygen to the tissues.
- The heart must be able to pump enough blood to the tissues to meet the patient’s oxygen requirements
- The volume of blood in the circulation must be adequate to ensure oxygenated blood is distributed to all the tissues.
HOW MUCH OXYGEN DOES THE BLOOD CARRY?
In a patient who is in good health:
- Each gram of haemoglobin combines with 1.34 ml of oxygen. Therefore, in blood with a normal haemoglobin concentration of 15g/dl, 100 mls of blood carries approximately 20 mls of oxygen combined with haemoglobin. In addition, a small quantity of oxygen is dissolved in the blood.
- The heart normally pumps approximately 5000 ml of blood per minute to the tissues in an average sized adult. This delivers about 1000 ml of oxygen to the tissues per minute.
- The cells in the tissues extract oxygen from the blood for metabolism, normally around 250ml of oxygen per minute. This means that if there is no oxygen being exchanged in the lung, there is only enough oxygen stored in the blood for around 3 minutes (only 75% of the oxygen carried by the haemoglobin is available to the tissues).
- Breathing 100% oxygen prior to induction of anaesthesia (preoxygenation) increases the oxygen stores in the lungs. If a patient stops breathing and is not ventilated, the amount of oxygen in the lungs will rapidly diminish. If the patient has been given 100% oxygen to breathe for several minutes prior to induction of anaesthesia, the increased oxygen reservoir will supply much needed oxygen, adding potentially life-saving minutes. There are many situations where this may be a factor. One example is in the pregnant mother where the big uterus reduces lung volume and the metabolic demands are increased by the foetus. Another example is in young children who have small lung volumes and high metabolic demands. They can use up oxygen very quickly and can sometimes be resistant to efforts to preoxygenate them.
- Anaemic patients have lower levels of haemoglobin and are therefore unable to carry as much oxygen in the blood. At a haemoglobin concentration of less than 6g/dl, delivery of oxygen to the tissues may become too low to meet the metabolic demands. Patients who suffer major blood loss during surgery and become acutely anaemic should be given 100% oxygen to breathe. This will increase the amount of dissolved oxygen in the blood and will improve tissue oxygen delivery by a small amount. Blood transfusion may be life saving.
WHAT IS OXYGEN SATURATION?
Red blood cells contain haemoglobin. One molecule of haemoglobin can carry up to four molecules of oxygen after which it is described as “saturated” with oxygen. If all the binding sites on the haemoglobin molecule are carrying oxygen, the haemoglobin is said to have a saturation of 100%. Most of the haemoglobin in blood combines with oxygen as it passes through the lungs. A healthy individual with normal lungs breathing air will have an arterial oxygen saturation of 95% – 100%. Venous blood that is collected from the tissues contains less oxygen and normally has a saturation of around 75%. (See appendix 1 for more details about this).
Arterial blood looks bright red whilst venous blood looks dark red. The difference in colour is due to the difference in haemoglobin saturation. When patients are well saturated their tongues and lips appear pink in colour; when they are very desaturated they appear blue. This is called cyanosis. However, it is difficult to detect cyanosis clinically, particularly in a dark skinned patient, and you may not notice this sign until the oxygen saturation is less than 90%. In a poorly lit operating theatre detecting cyanosis is even harder!
Cyanosis is only visible when the haemoglobin concentration is greater than 5 g/dl. A severely anaemic patient may not appear cyanosed even when extremely hypoxic as there is very little haemoglobin circulating through the tissues.
During anaesthesia the oxygen saturation should always be 95 – 100%. If the oxygen saturation is 94% or lower, the patient is hypoxic and needs to be treated quickly. A saturation of less than 90% is a clinical emergency.
Learning point: It is difficult to detect cyanosis clinically until the saturation is <90%. A patient who is severely anaemic may not appear cyanosed, even if the oxygen saturation is very low
PULSE OXIMETER QUIZ 2:
The correct answers are in the next section.
- What two things does a pulse oximeter measure?
- What is displayed on a pulse oximeter screen?
- An oximeter probe has two parts. What are they?
WHAT DOES A PULSE OXIMETER MEASURE?
There are TWO numerical values obtained from the pulse oximeter monitor:
- The oxygen saturation of haemoglobin in arterial blood. The value of the oxygen saturation is given together with an audible signal that varies in pitch depending on the oxygen saturation. A falling pitch indicates falling oxygen saturation. Since the oximeter detects the saturation peripherally on a finger, toe or ear, the result is recorded as the peripheral oxygen saturation described as SpO2.
- The pulse rate in beats per minute, averaged over 5 to 20 seconds. Some oximeters display a pulse waveform or indicator that illustrates the strength of the pulse being detected. This display indicates that the tissues are well perfused. The signal strength and the waveform fall if the circulation becomes inadequate.
THE PULSE OXIMETER:
A pulse oximeter is made up of the monitor containing the batteries and display, and the probe that senses the pulse.
This photo shows a typical pulse oximeter. The screen shows that the Sp02 is 98% and the pulse rate is 72 beats per minute.

The Pulse Oximeter Monitor
The monitor contains the microprocessor and display. The display shows the oxygen saturation, the pulse rate and the waveform (or pulse indicator) detected by the sensor. The monitor is connected to the patient via the probe.
During use, the monitor updates its calculations regularly to give an immediate reading of oxygen saturation and pulse rate. The waveform is continuously displayed to give information about the circulation. The audible beep changes pitch with the value of oxygen saturation and is an important safety feature. The pitch drops as the saturation falls and rises as it recovers. This allows you to hear changes in the oxygen saturation immediately, without having to look at the monitor all the time.
The monitor is delicate. It is sensitive to rough handling and excessive heat and can be damaged by spilling fluids on it. The monitor can be cleaned by gently wiping with a damp cloth. When not in use, it should be connected to an electricity supply to ensure that the battery is fully charged.
The Pulse Oximeter Probe
The oximeter probe consists of two parts, the light emitting diodes (LED’s) and a light detector (called a photo-detector). Beams of light are shone through the tissues from one side of the probe to the other. The blood and tissues absorb some of the light emitted by the probe. The light absorbed by the blood varies with the oxygen saturation of haemoglobin. The photo-detector detects the light transmitted as the blood pulses through the tissues and the microprocessor calculates a value for the oxygen saturation (SpO2).
In order for the pulse oximeter to function, the probe must be placed where a pulse can be detected. The LED’s must face the light detector in order to detect the light as it passes through the tissues. The probe emits a red light when the machine is switched on; check that you can see this light to make sure the probe is working properly.
Probes are designed for use on the finger, toe or ear lobe. They are of different types as shown in the photo. Hinged probes are the most popular, but are easily damaged. Rubber probes are the most robust. The wrap around design may constrict the blood flow through the finger if put on too tightly. Ear probes are lightweight and are useful in children or if the patient is very vasoconstricted. Small probes have been designed for children but an adult hinged probe may be used on the thumb or big toe of a child. For finger or toe probes, the correct orientation of the nail bed is marked on the probe by the manufacturer.
The oximeter probe is the most delicate part of a pulse oximeter and is easily damaged. Handle the probe carefully and never leave it in a place where it could be dropped on the floor. The probe connects to the oximeter using a connector with a series of very fine pins that can be easily damaged – see photo. Always align the connector correctly before attempting to insert it into the monitor. Never pull the probe from the machine by pulling on the cable; always grasp the connector firmly between finger and thumb.

Hinged finger probe showing connector that can only be connected to the oximeter one way by aligning the gap on the probe connector with the corresponding notch on the machine.
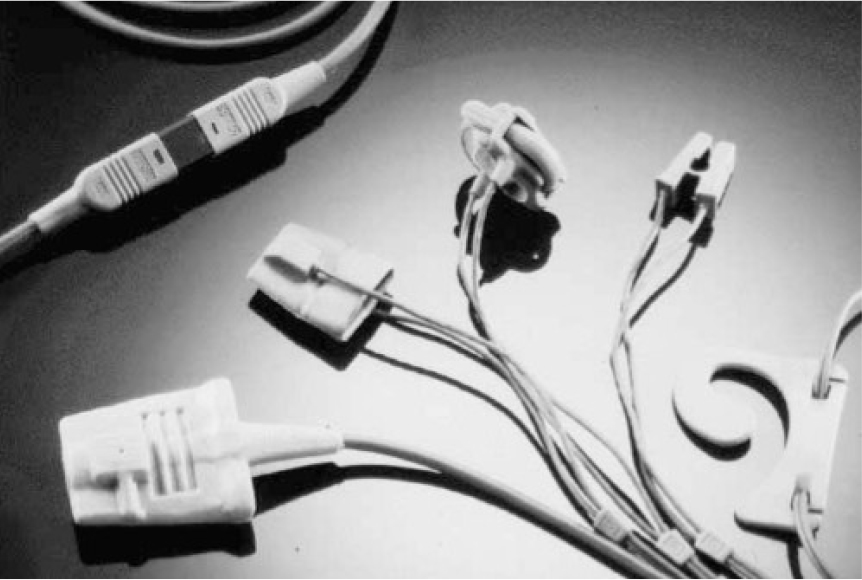
Rubber finger probes and ear sensor
When not in use, the oximeter probe cable may be loosely coiled for storage or carrying, but should not be coiled too tightly as this will damage the wires inside the cable. The lens and detector should be kept clean. Use soapy water or an alcohol soaked swab to gently clean dust, dirt or blood from the probe.
Learning point: In order to get a satisfactory reading the probe must be emitting a red light and must be correctly positioned to detect pulsatile blood flow.
Practical use of the pulse oximeter
- Turn the pulse oximeter on: it will go through internal calibration and checks.
- Select the appropriate probe with particular attention to correct sizing and where it will go (usually finger, toe or ear). If used on a finger or toe, make sure the area is clean. Remove any nail varnish.
- Position the probe carefully; make sure it fits easily without being too loose or too tight. Normally avoid the arm being used for blood pressure monitoring.
- Allow several seconds for the pulse oximeter to detect the pulse and calculate the oxygen saturation.
- Look for the displayed waveform or pulse indicator indicating that the machine has detected a pulse. Without a pulse signal, any readings are meaningless.
- Once the unit has detected a good pulse, the oxygen saturation and pulse rate will be displayed.
- Like all machines, oximeters may occasionally give a false reading – if in doubt, rely on your clinical judgement, rather than the machine.
- The function of the oximeter probe can be checked by placing it on your own finger.
- Adjust the volume of the audible pulse beep to a comfortable level for your theatre – never use on silent.
- Always make sure the alarms are on.
If no signal is obtained on the oximeter after the probe has been placed on a finger, check the following:
- Is the probe working and correctly positioned? Try another location.
- Does the patient have poor perfusion?
- Check for low cardiac output especially due to hypovolemia, cardiac problems or septic shock. If hypotension is present, resuscitation of the patient is required immediately. The signal will improve when the clinical condition of the patient improves.
- Check the temperature of the patient. If the patient or the limb is cold, gentle rubbing of the digit or ear lobe may restore a signal.
Tip: If you are uncertain that the probe is working properly, check it by testing it on your own finger.
What do the alarms on a pulse oximeter tell you?
Alarms alert the anaesthetist to clinical problems. The alarms are as follows:
- Low saturation emergency (hypoxia) i.e. SpO2 <90%
- No pulse detected
- Low heart rate
- High heart rate
The oxygen saturation in healthy patients of any age should be 95% or above.
Learning point: During anaesthesia the SpO2 should be 95% or above. If SpO2 is 94% or below, the patient must be assessed quickly to identify and treat the cause.
SpO2 OF ≤ 90% IS A CLINICAL EMERGENCY AND SHOULD BE TREATED URGENTLY.
‘No pulse detected’ alarm is commonly caused by the probe coming off the finger, but it may also be triggered if the patient is hypotensive, hypovolaemic, or has suffered a cardiac arrest. Check the probe site quickly and then assess the patient – ABC.
Heart rate alarms are useful to let the anaesthetist know that the heart is beating too fast or too slow. However, alert anaesthetists will have already noticed the abnormal heart rate before the alarms sound. Children normally have higher heart rates than adults, but the same oxygen saturation – see table below.
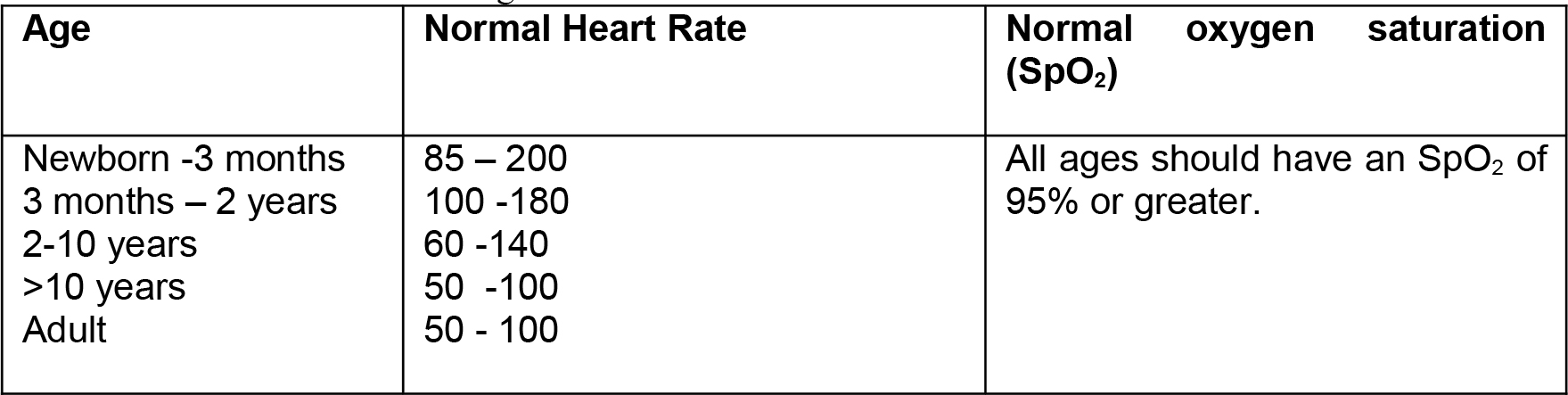
Table 1: Paediatric heart rate ranges
The high pulse alarm may be triggered by light anaesthesia, inadequate pain relief, atropine, ketamine, hypovolaemia, fever, or arrhythmia. The low pulse alarm may be triggered by bradycardia secondary to vagal stimulation due to e.g. peritoneal retraction, the oculocardiac reflex or intubation (particularly in babies) or from deep anaesthesia (particularly halothane) or severe hypoxia. A highly trained athlete or a patient who is taking ß-blockers may have a slow pulse rate.
What factors can interfere with the pulse oximeter reading?
Several factors can interfere with the correct function of a pulse oximeter including:
- Ambient light – bright light (such as the operating theatre light or sunlight) directly on the probe may affect the reading. Shield the probe from direct light.
- Shivering – movement may make it difficult for the probe to pick up a signal.
- Pulse volume – the oximeter only detects pulsatile flow. When the blood pressure is low due to hypovolaemic shock or the cardiac output is low or the patient has an arrhythmia, the pulse may be very weak and the oximeter may not be able to detect a signal.
- Vasoconstriction reduces blood flow to the peripheries. The oximeter may fail to detect a signal if the patient is very cold and peripherally vasoconstricted.
- Carbon monoxide poisoning gives a falsely high saturation reading. Carbon monoxide binds very well to haemoglobin and displaces oxygen to form a bright red compound called carboxyhaemoglobin. This is misinterpreted by the oximeter as oxyhaemoglobin and the oximeter may read 100%, even though the true oxygen saturation is very low and the patient may be very hypoxic. This is only an issue in patients following smoke inhalation from a fire.
Learning point: Hypovolaemia is the most common cause of a weak pulse oximeter signal during anaesthesia. Hypothermia should also be considered.
What is not measured by a pulse oximeter?
A pulse oximeter does not give direct information about respiratory rate, tidal volume, cardiac output or blood pressure. However, it does so indirectly and if these factors lead to desaturation, this will be detected by the pulse oximeter.
Learning point: Supplemental oxygen is often essential during anaesthesia. However, be aware that it can mask the effects of hypoventilation. Clinical vigilance will be necessary to ensure that ventilation is adequate especially if a capnograph is not available.
Pulse oximeters function normally in anaemic patients. In an extremely anaemic patient, the oxygen saturation will still be normal (95%-100%), but there may not be enough haemoglobin to carry sufficient oxygen to the tissues. During anaesthesia the patient should be given 100% oxygen to breathe to try to improve tissue oxygen delivery by increasing the amount of dissolved oxygen in the blood.
PART 2 to this tutorial will be published later this year.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/