General Topics

KEY POINTS
- Preanaesthetic testing is a universal practice with little current scientific support.
- In the United States alone, more than 20 billion US dollars are spent on preanaesthetic testing with questionable indications.
- Preanaesthetic testing should be ordered only if a clinical decision will be influenced by results.
- Several recommendations for routine testing are described, all of which have low levels of evidence of support, which are mainly through expert opinion and retrospective observational studies.
- Every institution should endorse or develop a protocol that highlights judicious use of preanaesthetic testing
INTRODUCTION
Preanaesthetic testing has been routinely performed in most countries around the world for the majority of patients scheduled for surgical procedures. This approach was proposed in the mid-1940s after Adams and Lundy1 speculated that these tests could help decrease the risk of perioperative anaesthetic complications. The implications of ordering routine testing are tremendous with unclear benefits and spiralling costs ranging close to 20 billion US dollars per year in the United States alone.
WHY IS PREANAESTHETIC TESTING PERFORMED?
The rationale for preanaesthetic testing is 2-fold: (1) to identify patients who could develop anaesthetic complications and (2) to provide ‘‘protection’’ for medical malpractice.
The recommendations of Adams and Lundy1 in 1942 were presumed to be clinically sound. As such, preanaesthetic testing has been implemented worldwide without question. Slowly over recent decades, dozens of observational studies have been unable
to show any clinical advantage of using the results of preanaesthetic testing on perioperative outcomes.
An observational study by Narr et al2 in 1997, involving 1044 patients from all age groups in which no tests were ordered preoperatively and who underwent anaesthesia and surgery, found only 1 unplanned admission that would not have been prevented with testing. At our hospital, Clinica Reina Sofia in Colombia, we found no serious adverse outcomes with a large retrospective cohort of 60 909 patients aged 2 months to 96 years, subject to anaesthesia without any preanaesthetic tests (endoscopy was not included in this cohort).3 Serious adverse outcomes were defined as myocardial infarction, pulmonary embolism, intensive care unit admission for medical reasons, central nervous system injury, renal failure and death.
Many similar cohorts have been described in the literature showing similar results. Recently, Ondeck et al4 published an analysis from the National Surgical Quality Improvement Program describing hip arthroplasty. Among 92 093 patients, abnormal sodium and abnormal creatinine levels (to a lesser extent) were correlated with adverse outcomes. Two major questions were raised: (1) Were these abnormal values obtained in patients with a medical history that would have indicated a need for tests anyway? (2) If the abnormal results were known, would the outcomes have changed?
Many clinicians justify routine testing as a malpractice defensive strategy. The American Society of Anesthesiologists (ASA) Closed Claims has not identified preoperative testing as an issue that led to a lawsuit. A similar experience has been described in a Colombian anaesthesia malpractice registry, FEPASDE, in which no malpractice cases related to absence of preanaesthetic testing have been reported.5
A significant proportion of tests results are not reviewed by the medical teams. In a meta-analysis by Callen et al,6 of concern was that 6.8% (79/1163) to 62% (125/202) of abnormal laboratory tests and 1.0% (4/395) to 35.7% (45/126) of abnormal radiology tests were not reviewed. Even when the cause-effect relationship of an abnormal test result and an adverse outcome is weak, the finding of an abnormal result that is not acknowledged in the medical record can become a major liability for the anaesthesiologist involved in the case.
HOW USEFUL IS PREANAESTHETIC TESTING?
Even though preanaesthetic testing is virtually universal, it comes as a surprise to know that only 2 randomised clinical trials (RCTs) have evaluated preanaesthetic testing.
The first RCT was completed in 19 557 patients scheduled for cataract surgery. Participants were randomised to conventional testing or to directed testing (eg, diabetics would have serum glucose ordered). Overall, 31.3 complications per 1000 patients occurred in both groups, which were not preventable with testing (mainly hypertension and bradycardia).7
The other RCT was conducted in 1061 patients scheduled for ambulatory surgery. Participants were randomised to no testing versus protocol-driven testing. There were no significant differences in outcomes between the 2 groups.8
As seen above, only 2 RCTs showed no benefit of nondirected preanaesthetic testing. Likewise, there are multiple retrospective studies showing similar results. A recent analysis of 440 857 Medicare patients subject to cataract surgery concluded that preoperative testing was not related to patient comorbidities but to practitioner preferences, questioning the rationale of preanaesthetic testing.9
When considering symptomatic patients, Hoeks et al10 showed that low adherence (21%) to preanaesthetic testing recommendations of the American College of Cardiology/American Heart Association guidelines for cardiac patients undergoing noncardiac surgery did not result in worse outcomes. This finding questions the impact of recommendations even among patients with significant comorbidities who presumably would benefit.
Consistently, systematic reviews and meta-analyses11 have not shown benefit of preanaesthetic testing for common coexisting diseases, which also supports the notion of avoiding unnecessary screening. Therefore, preanaesthetic testing should be subject to the well-established principle that ‘‘a diagnostic test should be obtained only when its outcome could alter the management of the patient.’’12
Another concept to understand is that even in oncologic patients, the changes in tests are very uncommon even after periods of 1 year or more, as shown by Ramos et al.13 They found a probability of change in at least 1 of the preoperative examinations (including blood work and electrocardiograms and chest X-rays) of 1.7%, 3.6% and 6.4% during the 12-, 24- and 36-month intervals, respectively, for patients aged <50 years and 2.1%, 9.2% and 13.4% respectively, for patients ≥50 years of age.13
COST IMPLICATIONS
In the past decade, all health care stakeholders have endorsed the concept of value in health care. The concept of value is simple: achieve the best possible outcome at the least cost possible. In this scenario, all medical interventions are subject to economic scrutiny to determine their impact of achieving best outcomes.
At more than 20 billion US dollars per year, preanaesthetic testing costs are staggering, in a setting where evidence supporting the impact of this expenditure does not currently exist. At Clinica Reina Sofia, we calculated the impact of streamlining preanaesthetic testing and showed that even when taking into account the cost one anaesthesiology consult per patient, the savings over 10 years in a middle-income country exceeded 151 000 USD.14
After an analysis of Medicare-funded cataract surgery, Chen calculated an expense of ~107 USD per patient, adding to an existing estimate of 45.4 million USD, which did not demonstrate impact on outcomes.15 There is also the ‘‘cascading’’ effect of ordering a test that is not indicated, such as an electrocardiogram (ECG). Ganguli et al16 showed that patients scheduled for cataracts having an ECG ordered had 5 to 10 additional interventions per 100 patients with no impact on outcomes at the expense of 35 million USD additional cost.16
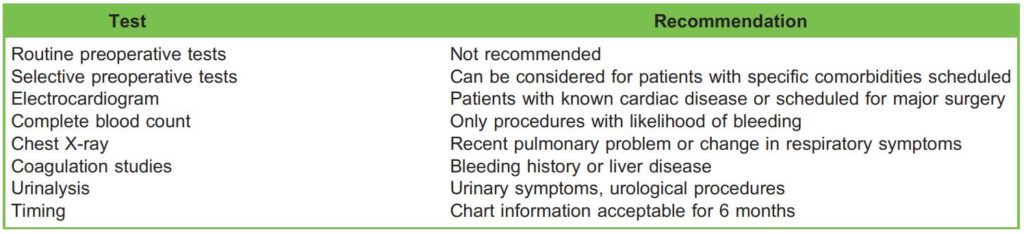
Table 1. Summary of American Society of Anesthesiologists Advisory17
GUIDELINES
There are many guidelines on this topic, among them the ASA Practice Advisory for Preanesthesia Evaluation (Table 1),17 the National Institute for Health and Care Excellence (NICE) routine preoperative tests for elective surgery (Table 2)18 and from a website sponsored by most of the medical specialty societies of the United States, ChoosingWisely.org (Table 3). It is interesting to note that these recommendations are based mainly on expert opinions, as there is a great void of supportive evidence in the field.
The NICE guideline is stratified according to surgery magnitude and comorbidities and is useful to consider for its details.
A concept highlighted in the ASA Advisory is, ‘‘Practice Advisories are not supported by scientific literature to the same degree as standards or guidelines because of the lack of sufficient numbers of adequately controlled studies.’’
HOW TO IMPROVE RECOMMENDATION ADHERENCE?
Guidelines, advisories and recommendations are affected by poor adherence, sometimes because of the complexity of recommendations or challenges to implementation. One such example may be the NICE guidelines, which attempt to be thorough but entail increased complexity. The NICE guidelines can be used as a reference from which to base local approaches.
We can share our experience at the Clinica Reina Sofia where a protocol was adopted after a heuristic process of development based on the data from >160 000 preanaesthetic assessments (Figure 1).19
Our protocol differentiates 2 types of procedures: minor and major surgery. Major defines procedures that carry a strong likelihood of requiring high-dependency care postoperatively in local practice (depending on the local practice in the hospital, some procedures may have poorer outcomes than in other hospitals, so may consider them as major surgery). The remaining procedures are defined as minor. If the patient does not have specific comorbidities (coronary artery disease, renal dysfunction, abnormal coagulation, diabetes, arrhythmias, changes in pulmonary symptoms, etc) that require specific testing, a simple approach is suggested.
Based on an analysis completed in 2015, with this approach we managed to anaesthetise 52% of scheduled hip arthroplasties (n = 2457) without ECGs and 23% with only a complete blood count, and we were able to report 0.43% mortality at 30 days, which was comparable with international registries. Currently, we have evolved to care for more than 500 ambulatory hip arthroplasties in the past 3 years using this protocol. This is a practical example of the protocol; in our hospital, hip and knee arthroplasties very rarely require high-dependency unit admission, so they are not considered major surgeries.
Policy changes, such as adopting no remuneration for routine testing, can also motivate change to preanaesthetic testing. This approach was more effective than that of publishing recommendations according to Henderson et al,20 in which promotion of recommendations against routine ordering vitamin D testing had much less impact (4.5%) than suspending payment for this screening (92.7% reduction).

Figure 1. Clinica Reina Sofia routine preoperative testing protocol based on >163;000 patients.19 (One specific exception: in our practice, neurosurgical patients are not considered major surgery although admitted to a high-dependency unit; this is done mainly for neurological observation.)
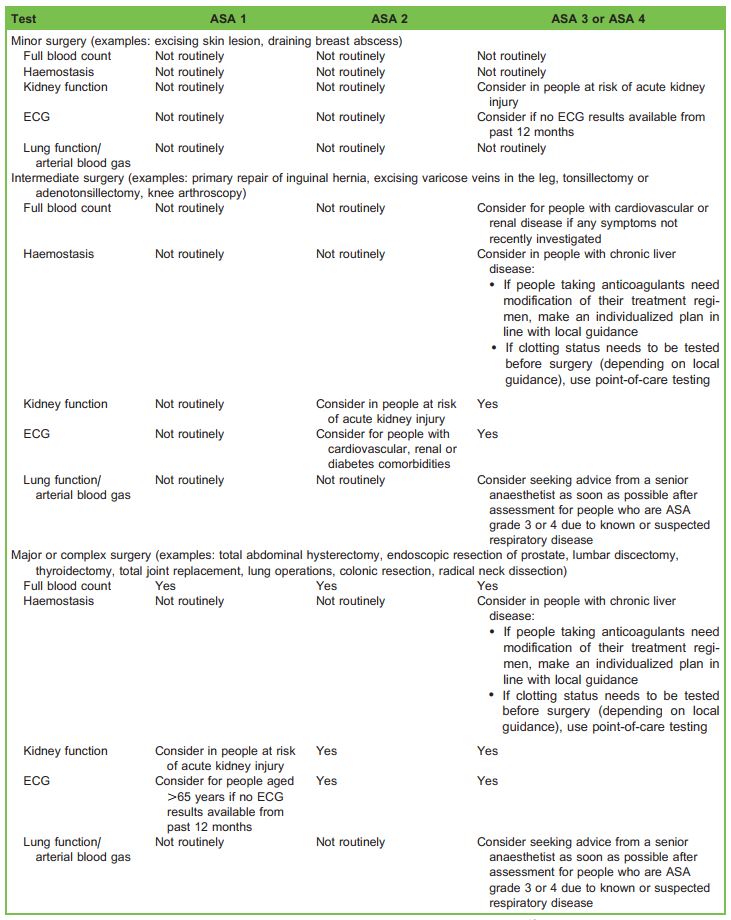
Table 2. Summary of National Institute for Health and Care Excellence Recommendations.18 ASA indicates American Society of Anesthesiologists; ECG, electrocardiogram
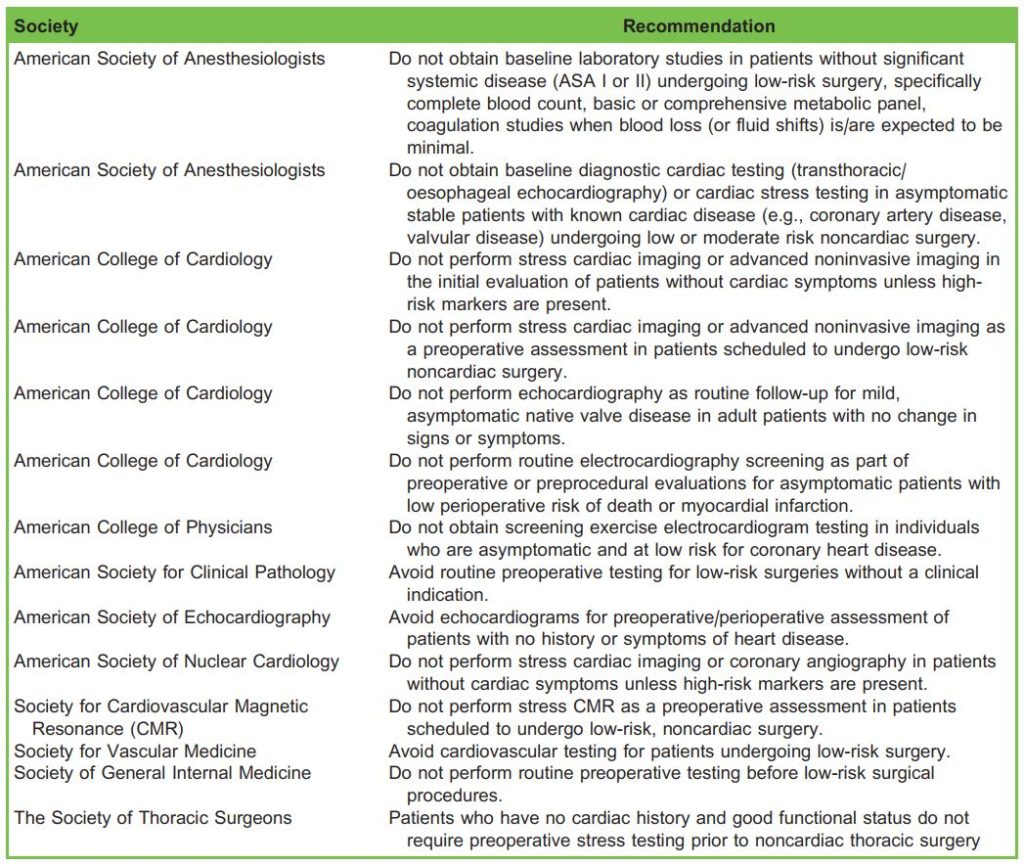
Table 3. Summary of Choosing Wisely Preanaesthetic Testing. ASA indicates American Society of Anesthesiologists
SUMMARY
Preanaesthetic testing is a complex area currently not supported strongly by research. Each institution should approach preanaesthetic testing by adopting existing validated guidelines or produce guidelines of their own that are influenced by current research and seek strong compliance from stakeholders. The goal should be to achieve the ideal balance to minimise testing that is not warranted to save money and avoid unnecessary cancellations of surgery while assuring patient safety.
REFERENCES
- Adam R, Lundy J. Anesthesia in cases of poor risk: Some suggestions for decreasing the risk. Surg Gynecol Obstet. 1942;74(3):1011-1101.
- Narr BJ, Warner ME, Schroeder DR, Warner MA. Outcomes of patients with no laboratory assessment before anesthesia and a surgical procedure. Mayo Clin Proc. 1997;72:505-509
- Ibarra P. Experience of a preanesthetic assessment clinic in Colombia with 163,287 patients: Clinica Reina Sofia. 2020. (Internal presentation, pending publication)
- Ondeck NT, Fu MC, McLynn RP, Bovonratwet P, Malpani R, Grauer JN. Preoperative laboratory testing for total hip arthroplasty: unnecessary tests or a helpful prognosticator. J Orthop Sci. 2020;25:854-860.
- Bocanegra J, Arias J. Characterization and analysis of adverse events in closed liability cases involving anaesthetists who received legal support from the Colombian Society of Anaesthesia and Resuscitation (S.C.A.R.E.), Colombia, 1993-2012. Rev Col Anest. 2016;44:203-210.
- Callen JL, Westbrook JI, Georgiou A, Li J. Failure to follow-up test results for ambulatory patients: a systematic review. J Gen Intern Med. 2012;27:1334-1348.
- Schein OD, Katz J, Bass EB, et al. The value of routine preoperative medical testing before cataract surgery. Study of Medical Testing for Cataract Surgery. N Engl J Med. 2000;342:168-175.
- Chung F, Yuan H, Yin L, Vairavanathan S, Wong DT. Elimination of preoperative testing in ambulatory surgery. Anesth Analg. 2009;108:467-475.
- Chen CL, Lin GA, Bardach NS, et al. Preoperative medical testing in Medicare patients undergoing cataract surgery. N Engl J Med. 2015;372:1530-1538.
- Hoeks SE, Scholte op Reimer WJ, Lenzen MJ, et al. Guidelines for cardiac management in noncardiac surgery are poorly implemented in clinical practice: results from a peripheral vascular survey in the Netherlands. Anesthesiology.
2007;107:537-544. - Saquib N, Saquib J, Ioannidis JP. Does screening for disease save lives in asymptomatic adults? Systematic review of meta-analyses and randomized trials. Int J Epidemiol. 2015;44:264-277.
- Sox H, Stern S, Abrams HB. The use of diagnostic tests: a probabilistic approach. In: Institute of Medicine, ed. Assessment of Diagnostic Technology in Health Care: Rationale, Methods, Problems, and Directions: Monograph of the Council on Health Care Technology. Washington, DC: National Academies Press; 1989.
- Ramos LWF, Souza CF, Dias IWH, et al. Validity time of normal results of preoperative tests for surgical reintervention and the impact on postoperative outcomes [in Portuguese]. Braz J Anesthesiol. 2018;68:154-161.
- Ibarra P. Preanesthetic clinic cost effectiveness. Poster presented at; World Congress of Anaesthesiologists; Paris, France; 2004.
- Chen CL, Clay TH, McLeod S, Chang HP, Gelb AW, Dudley RA. A revised estimate of costs associated with routine preoperative testing in Medicare cataract patients with a procedure-specific indicator. JAMA Ophthalmol. 2018;136:231-238.
- Ganguli I, Lupo C, Mainor AJ, et al. Prevalence and cost of care cascades after low-value preoperative electrocardiogram for cataract surgery in fee-for-service Medicare beneficiaries. JAMA Intern Med. 2019;179(9):1211-1219.
- Apfelbaum JL, Connis RT, Nickinovich DG, et al. Practice advisory for preanesthesia evaluation: an updated report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Anesthesiology. 2012;116:522-538.
- National Institute for Health and Care Excellence. Routine Preoperative Tests for Elective Surgery: NICE Guideline [NG45]. London: National Institute for Health and Care Excellence; 2016.
- Ibarra P. ¿Cuales laboratorios preaneste´ sicos se necesitan en pacientes asintoma´ ticos? Actualizacio´ n del Protocolo del Departamento de Anestesiologı´a de la Clı´nica Reina Sofı´a. Rev Col Anest. 2007;35:301-312.
- Henderson J, Bouck Z, Holleman R, et al. Comparison of payment changes and Choosing Wisely recommendations for use of low-value laboratory tests in the United States and Canada. JAMA Intern Med. 2020;180:524-531.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/