General Topics

Scenarios and self assessment
Please consider these five scenarios and associated questions below before reading the text of the tutorial.
Scenario A
You are called urgently to review an 8 year old child who, after a GA for manipulation of a forearm fracture, had returned to the ward 15 minutes before. You find him lying on his back with a nurse trying to ventilate him with a mask and bag. There is some respiratory effort but the airway is clearly obstructed. Suctioning the pharynx, putting the patient in the recovery position, insertion of an oral airway and application of jaw thrust corrects the problem, allowing spontaneous ventilation and return of good oxygenation. 30 minutes later the patient is easily roused and seems to be fine.
- a) What may have contributed to this occurrence?
- b) How would you avoid it happening again?
Scenario B
You have agreed to help a small district hospital in western Kenya develop a recovery area to support their twin operating rooms. There is a mains electricity supply to some parts of the hospital but currently no designated space or equipment for recovery. The nurse anaesthetist has sent you a list of 10 items that they want you to provide. Rank this list in order of importance; 1 for the most important 10 for the least important:
- Large tent (9 square metre base)
- Self inflating bag with facemasks and oral airways
- Elevating blocks for the foot of their non-tipping trolley
- DIY manual on electrical wiring
- An oxygen concentrator
- Pulse oximeter
- Sphygmomanometer
- Suction machine and catheters
- Battery operated lamp (torch)
- Hand bell
What are the reasons for your ranking?
Scenario C
The recovery nurse reports a BP of 100/40 mmHg and pulse rate of 90 following a spinal anaesthetic for open prostatectomy in a 70 year old man. She feels that he is a bit confused but appears well perfused. His preoperative BP was 150/90 and he was stable when you handed him over 15 minutes before. You can’t come out of the operating room immediately.
- a) What are the possible causes?
- b) What other information do you require immediately?
- c) What advice will you give the nurse on further management?
Scenario D
You are a patient who is about to have lower abdominal surgery. Rank the following list of 10 possible immediate post-anaesthetic outcomes in the recovery period in order of desirability; 10 for most desirable and 1 for the least desirable
- Nausea
- Recall of surgery without pain
- Gagging on an ET tube
- Shivering
- vomiting
- residual weakness
- somnolence
- sore throat
- normal (no problems)
- pain
How might we prevent and immediately manage your three most undesirable outcomes?
[E] An 18 year old woman has just had an emergency caesarean section under GA following severe foetal distress. The BP had been normal in labour and there were no signs of pre-eclampsia during pregnancy. Because she is neither breathing nor waking up despite reversal of neuromuscular blockade, you have taken her to recovery with an endotracheal tube in place for continuing ventilation. She is pink, warm but a bit sweaty with midsized pupils. Pulse rate is 120 and BP is 180/100.
- a) What are the possible causes of this delayed waking?
- b) How are you going to continue managing the case?
Key points in this tutorial
- Immediate recovery from anaesthesia is a concept of care during not just a place to put the patient after surgery. Responsibility can never be fully delegated by the anaesthetist to others.
- Most problems relate to Airway, Breathing and/or Circulation; with delayed return of consciousness and inadequate analgesia being other common related issues. All these should be anticipated.
- Facilities required are the same as those necessary for anaesthesia where-ever that might be administered. If such facilities cannot be duplicated in a separate location, then the safest place to recover patients is in the operating room.
- The most important monitor is a well informed and skilled person; with immediate access to anaesthetic assistance. Technical support is important but sophisticated electronic monitors are not universally essential
- Discharge to a general ward should only be considered when you have a conscious, co- operative and comfortable patient who is well oxygenated and well perfused; and likely to remain so.
Background
Immediate recovery from anaesthesia should be thought of as a concept rather than a place of care. It is a critical part of postoperative management, and can influence the outcome from surgery. The principles for prevention and management of problems are the same whether you are working in a large city hospital in the UK or a small clinic in rural Africa; but each practitioner will have to apply these principles to suit his/her environment.
Immediate Recovery Issues
Having an awake, co-operative and comfortable patient who is well perfused with adequate amount of oxygenated blood is our aim but there are several possible complications which might undermine our achievement of this objective. Most problems can be anticipated, and detected early through appropriate clinical monitoring
Airway
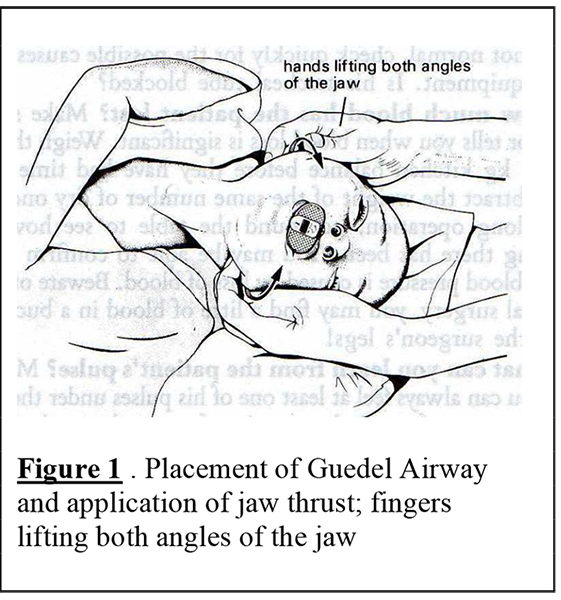
A compromised or obstructed airway is a common problem. This may be purely anatomical with relaxed soft tissues obstructing the pharynx, or due to the presence of secretions, vomitus or blood. The use of oral airways, patient position on the side with the head and neck dependent and manual application of jaw thrust should avoid problems, but we all still get caught out from time to time. “Jaw thrust” (figure 1), rather than “chin pull” is a skill that all anaesthetists and recovery nurses should be able to apply well. Infants and children are at particular risk and you are well advised to personally supervise the early recovery of these cases.
Breathing
Even with a clear airway, ventilation and therefore oxygenation may be inadequate for several reasons. Incomplete reversal of muscle relaxants, abdominal distension and/or pain may be the cause. High concentrations of oxygen will frequently reverse hypoxia but remember: oxygen therapy is only a supportive treatment while you identify and correct the underlying cause of hypoxia.
Circulation
Colour, capillary refill and pulse can tell us so much about a patient’s circulatory state. Measuring blood pressure and urinary output is important but both may mislead us in some situations. A young adult who is awake, orientated, pink and warm with a good volume pulse of 80 bpm and a BP of 80/50 should not worry us. However, if the same patient is pale, sleepy and peripherally cold with a pulse rate of 120 and a normal BP this may indicate hypovolaemia due to blood loss. In the latter case, retention of the patient in the recovery area is essential for further assessment and continuation of oxygen and fluid therapy. Low urinary output during and immediately after major surgery is to be expected and so, in isolation, this measure may not always be helpful.
Delayed return of consciousness
Drugs and metabolic derangements can contribute to this and the cause is often multifactorial. Remember that occasionally a patient who appears comatosed might be conscious and aware of being paralysed; as a result of continuing action of muscle relaxants.
Effective symptom control
Guidance on the appropriate methods of managing pain, nausea, vomiting and shivering will not be dealt with in detail here. If, following a laparotomy, a patient is lying on his side shivering and in pain, then ventilatory function and oxygenation are likely to be seriously impaired. Putting him in a semi- sitting position, giving a slow IV injection of morphine or pethidine titrated to a dose that allows him to cough comfortably, and use of blankets will improve matters significantly.
Standard of recovery facilities
Basically these are the same as those necessary for safe administration of anaesthesia; whether this is in an operating room or other treatment area (e.g. X-ray or accident department). If such facilities and standards cannot be provided in a separate location, then the best place to recover patients is in the operating room or treatment area whatever the effect this might have on a following case in the theatre schedule. In the UK the Association of Anaesthetists offers updated guidance on what should be provided, and the principles behind this guidance (see further reading) can be applied to different environments throughout the world.
Staffing
The most important recovery resource is well informed and skilled staffing (nurse or other) with immediate access to anaesthetic assistance. Sophisticated electronic monitoring devices are desirable but may on occasions be a source of complacency if they are ever seen to be a substitute for clinical assessment. Staff training is essential and in the UK this is increasingly governed by established hospital and national standards. There is also more basic, but nevertheless well established and valuable, guidance available (see further reading below).
Communication
The anaesthetist should formally handover all patients to whom he is delegating the supervision of the recovery; and, even if it is only in the form of a humble hand-bell or whistle, should ensure that an emergency call system exists to summon him if required.
Accommodation
This needs to be large enough to accommodate a bed/trolley and the equipment outlined below with room for staff to work at each end and each side of the patient. Generally this will require 9-10 square metres of floor area for each patient; and this space should be well lit day and night and have a temperature between 20 and 25°C.
Equipment and monitoring
The most important monitoring devices are the eyes, ears and hands of staff. Even an experienced recovery nurse cannot do without some technical support; primarily the close proximity of the anaesthetist. Other essential items are a tipping bed/trolley, suction apparatus with catheters, some means of providing oxygen, a sphygmomanometer; and a self inflating bellows with airways and masks. Pulse oximeters are now considered essential monitors in many parts of the anaesthetic world and clearly provide reassuring early warnings of hypoxia and related events.
Drugs and consumables
Immediate access is required to the same set of basic drugs, IV fluids, syringes and infusion sets that should be available to the anaesthetist in the operating room
Discharge to the ward
All theatre units should have clear criteria for discharge to a general ward
- Awake, responsive and maintaining airway without excessive stimulus
- Adequate analgesia
- Stable cardiovascular system
- Normal respiration and oxygenation
- Temperature within acceptable limits
- No continuing surgical problems (bleeding or drain loss)
- Instructions for the ward communicated to staff (oxygen, drugs and fluid)
Further Reading:
Some of the texts below are available on CD-Rom’s made available through Teaching Aids at Low Cost (TALC); if you have one or both CDs make sure the appropriate disc is in the CD drive before clicking on the link. Others can be found on the internet.
- Pulse oximetry for perioperative monitoring Pedersen T et al; Cochrane Library, Issue 4; 2004 Health Development CD-ROM; Issue 8; TALC; 2006 file:///D|/html/clients/cochrane/html/AB002013.htm
- Immediate Postanaesthetic Recovery Guidelines of the Association of Anaesthetists of Great Britain and Ireland; 2002 visit: www.aagbi.org/publications/guidelines/docs/postanaes02.pdf
- Postoperative care of the patient Paul Foster; in Basic Anaesthetic Training Manual, Chapter 10 Health Development CD-ROM Issue 8; TALC; 2006
file:///D:\html\clients\pfoster\Chapter 10.pdf - Monitoring in the Recovery Room Update in Anaesthesia; 2000; Issue 11; Article 9 Anaesthesia Resource CD 1; TALC 2004; file:///D|/content/WAWFSA/html/u11/u1109_01.htm OR visit: www.nda.ox.ac.uk/wfsa/html/u11/u1109_01.htm
- Safe Recovery from Anaesthesia Maurice King et al; Care before, during and after the operation; in Primary Anaesthesia; Oxford University Press, New York 1986; pages 15 – 22
Additional points arising from the scenario questions
Scenario A
- a) This case was discharged from the recovery area prematurely. Patients may appear to awake and reject a Guedel airway if vigorously stimulated, and will then later revert to the unconscious state with an obstructed airway. If a pre-operative or intra-operative opioid was given, this may be contributing. Once a fracture has been immobilised the patient has little need for continuing opioid analgesia and when left unstimulated will demonstrate the signs of relative overdose.
- b) Good staff training and compliance with appropriate recovery area discharge criteria are required. Any nurse on a ward receiving patients from theatre should be familiar with managing an obstructed airway and a sedated patient. But they are unlikely to be as skilled as a trained and experienced recovery nurse in preventing and correcting anatomical airway obstruction.
Scenario B
There is no “right” ranking order but this is my personal ranking in order of importance to me:
- Hand bell
- Bells and whistles are excellent alarm systems as long as the recovery area is close enough to those who are expected to respond.
- Sphygmomanometer
- Essential monitor
- Suction machine and catheters
- Essential equipment
- Self inflating bag with facemasks and oral airways
- Important but requires training on effective use
- Oxygen concentrator
- A very useful investment if you have a reliable electricity supply.
- Pulse oximeter
- A review in 2004 concluded that available evidence “indicates that the value of peri-operative monitoring with pulse oximetry is questionable in relation to improved reliable outcomes, effectiveness and efficiency” (see further reading above).There are indeed acceptable clinical ways of detecting hypoxia but it is unlikely that many anaesthetists or recovery nurses would give up their pulse oximeters on the basis that others have to manage without!
- Battery operated lamp
- The head lamp variety in particular is very useful when there is a power cut; and this is much safer than a kerosene lamp in the presence of oxygen and/or ether! Battery replacement might be an issue. If you need one during the day near the equator, then you have the wrong location for the recovery area which should have good natural lighting; or you have forgotten to remove your sunglasses!
- Large tent
- If the criteria and standards for safe recovery are best provided in a tent, then so be it. But it might be more practical to obtain one there! 9 square metres is fine for one patient but if two bays are required then double the size.
- Elevating blocks
- This is one way of overcoming the lack of tilting trolleys and can be easily made. But there are other ways to achieve the objective of having the pharynx dependent e.g. a pillow can be placed under the dependent shoulder/thorax
- DIY manual on electrical wiring
- Never mess with somebody else’s electrical wiring however good you think you are at it! This is dangerous. It would be more appropriate to take a basic training manual for recovery nurses (see further reading above).
Scenario C
- a) This man is hypotensive with the likely cause being one or both of the following:
- Hypovolaemia due to continued bleeding.
- Vasodilatation due to continuing sympathetic blockade with reduced venous return that may have been masked earlier if his legs were in the lithotomy position for surgery.
- b) You want to know his pulse rate, what is happening with bladder irrigation and wound drain. And if your recovery nurse is familiar with spinal anaesthesia, she should be able to report on the level of sensory blockade to cold and touch. If not, you will have to teach her later.
- c) Immediate management is administration of oxygen, leg elevation and an IV fluid challenge with 500 mls saline/Ringers lactate. Ask her to report back within 15 minutes, but you must try to review the patient yourself before that time.
NB: patients who have had spinal anaesthesia have as many recovery needs as those who have had general anaesthesia.
Scenario D
Some occurrences after anaesthesia are more disturbing than others but most can be anticipated and prevented. A study in 1999 involved asking 101 patients to rank 10 possible immediate postoperative outcomes. Here is their combined response to that question with 1 for the least desirable and 10 for the most desirable:
- Vomiting
- Gagging on the ET tube
- Pain
- Nausea
- Recall of surgery without pain
- Residual weakness
- Shivering
- Sore throat
- Somnolence
- Normal (no problems)
I will not deal here with all these issues but it is important to think about how you could:
- a) Prevent the most undesirable problems
- b) Guide recovery staff in appropriate management when they do occur.
More information on this study can be found at: www.jr2.ox.ac.uk/bandolier/booth/operations/anaespat.html
Scenario E
- a) There are several causes of delayed wakening with apnoea after anaesthesia but the most likely possibilities here are:
- A post-ictal state following an eclamptic seizure under anaesthesia; the lack of preoperative signs might put this low on your list. In addition one would expect to see good muscle tone.
- Hypocapnoea following hyperventilation during surgery.
- Overdose of opioids; this would be associated with other signs such as pinpoint pupils.
- The patient may in fact be awake but paralysed with inadequate reversal of non-depolarising muscle relaxant or suxamethonium apnoea (unusual but likely in this case). Awareness would explain tachycardia and hypertension. A nerve stimulator will help here if you have one.
- b) Ventilation may be required for some hours and you must ensure that sedation and analgesia are given on a continuous or regular and generous basis until spontaneous recovery from paralysis occurs. You clearly need to supervise this case personally in the recovery area, particularly if you do not have a critical care unit to which she can be transferred.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/