Obstetrics Anaesthesia

QUESTIONS
Before continuing, try to answer the following questions. Statements may either be true or false. The answers can be found at the end of the article.
- Regarding the causes of death in the UK 2006-2008 Confidential Enquiry into Maternal Deaths:
a. Sepsis was the most common cause of death
b. Overall mortality decreased compared with the 2003-2005 triennium
c. Health inequalities in both ethnic and socioeconomic groups were reduced
d. Suicide was the most common cause of indirect deaths - Regarding the direct causes of maternal mortality in the 2006-2008 report:
a. Improved maternal mortality was predominantly due to a reduction in deaths from thromboembolism
b. Staphylococcus was isolated in 50% of sepsis-related deaths
c. Prompt perimortem caesarean section following maternal collapse was a contributor to the reduced mortality from amniotic fluid embolism
d. The majority of deaths from haemorrhage occurred in the postpartum period - Regarding pre-eclampsia:
a. Mortality from pre-eclampsia improved in the UK compared with the 2003-2005 triennium
b. Patients with a systolic BP of >150mmHg require immediate treatment
c. A systolic BP >180mmHg constitutes a medical emergency and requires expedient treatment
d. Ergometrine is safe for active management of the third stage of labour - Regarding the following statements, which are true and which are false?
a. Previous history is the greatest risk factor for thromboembolism
b. Following decision to operate, if time allows, a functioning epidural established in labour should be topped-up without delay to provide surgical anaesthesia
c. Orogastric tube placement to reduce gastric volume is not recommended in women undergoing caesarean section under general anaesthesia
d. Women with placenta accreta who decline blood and blood products should be delivered in major maternity units
This tutorial highlights the key findings and recommendations from the 2006-2008 report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. Anaesthesia related issues are explored in more detail and important lessons discussed.
THE CONFIDENTIAL ENQUIRIES INTO MATERNAL DEATHS
The Confidential Enquiries into Maternal Deaths was established in 1952 and is the world’s longest running clinical audit. The most recent report covers the 2006-2008 triennium and was administered by the independent charity, the Centre for Maternal and Child Enquiries (CMACE) 1. CMACE superseded the Confidential Enquiry into Maternal and Child Health (CEMACH) in 2009, which itself had replaced other bodies responsible for reviewing maternal deaths within the UK.
Maternal death is defined according to the tenth revision of the International Classification of Diseases, Injuries and Causes of Death (ICD 10) as:
‘‘the death of a woman while pregnant or within 42 days of termination of pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes”.
Maternal deaths are classified as direct, indirect or late 1.
- Direct maternal death – death resulting from conditions or complications or their management that are unique to pregnancy, occurring during the antenatal, intra-partum and postnatal periods
- Indirect maternal death – death resulting from previously existing disease, or disease that develops during pregnancy not as the result of direct obstetric causes, but which were aggravated by the physiological effects of pregnancy.
- Late maternal death – death due to direct or indirect cause occurring more than 42 days but less than one year after the end of pregnancy.
The Confidential Enquiry is both a quantitative and qualitative analysis of maternal deaths within the UK. It aims to reduce maternal morbidity and mortality through identification of preventable factors associated with patient harm. It works closely with the UK Obstetric Surveillance System (UKOSS), which surveys a range of uncommon disorders of pregnancy that do not necessarily result in maternal death. The current report makes recommendations to improve patient safety and bring about beneficial changes to the way maternity services are organised.
KEY FINDINGS
In the 2006-2008 triennium, 261 women in the UK died directly or indirectly as a result of pregnancy. The overall maternal mortality rate was 11.39 per 100 000 maternities – an improvement from the previous report due largely to a reduction in maternal deaths from thromboembolic disease and to a lesser extent haemorrhage. The report also found, for the first time, a reduction in the health inequalities gap of both ethnic and socioeconomic groups. Despite these improvements, the report warns against complacency, noting that substandard care is still too common.
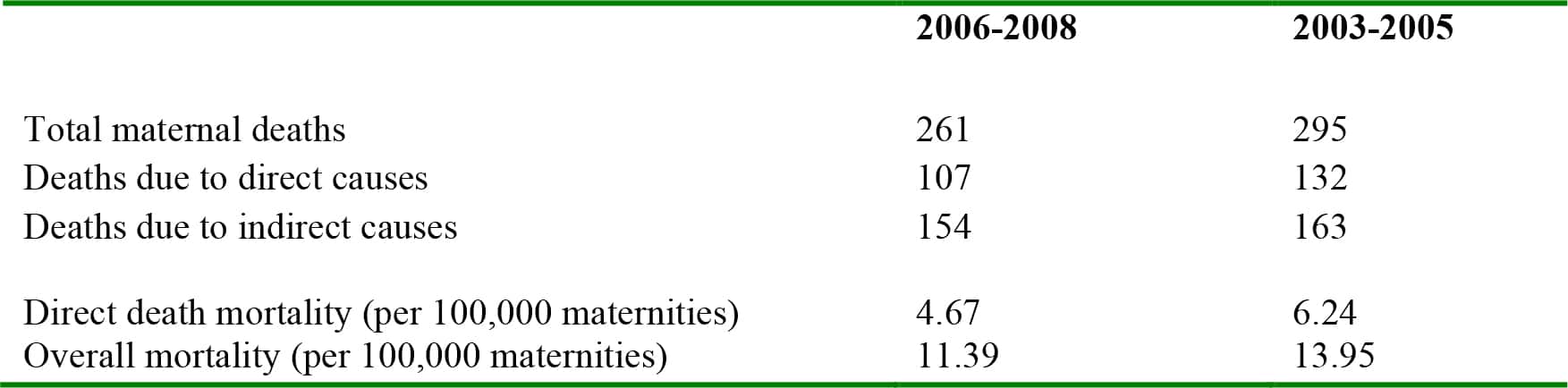
Table 1. Key mortality data from the last two Confidential Enquiries
TOP TEN RECOMMENDATIONS
The report makes several recommendations and prioritises the implementation of the ‘Top Ten’ recommendations to ensure the UK maternal mortality rate continues to decline. These are:
- Pre-pregnancy counseling: women with potentially serious pre-existing medical conditions should be offered counseling prior to pregnancy and a plan made for management of their pregnancy.
- Professional interpretation services: non-English speaking women should be offered interpretation services.
- Communications and referrals: referral of pregnant women for specialist review should be prioritised. Trainee doctors and midwives should have a low threshold to refer women to senior clinicians and must receive an immediate response to avoid inappropriately long waiting times for specialist review.
- Women with potentially serious medical conditions require immediate and appropriate multidisciplinary specialist care: referral to an appropriate specialist centre should be made early if pregnancy is likely to be complicated by serious medical or mental health conditions. Likewise, if a serious condition develops during pregnancy, referral to an appropriate specialist centre should be made.
- Clinical skills and training: clinical staff should undertake regular, written, documented and audited training to aid early identification and initial management of serious obstetric conditions or emerging obstetric emergencies.
- Specialist clinical care – identifying and managing very sick women: a national modified early obstetric warning score (MEOWS) chart should be routinely used for sick pregnant and postnatal women to enable timely recognition, treatment and referral of women with critical illness. This observation chart should be used for sick pregnant women cared for outside the maternity unit, e.g. the Emergency Department. A team approach should be employed to identify and manage acutely unwell women and those with significant co-morbidities.
- Systolic hypertension requires treatment: women with pre-eclampsia whose systolic BP is 150 – 160 mmHg or more require urgent treatment.
- Genital tract infection/sepsis: all women should be offered information on the risks, signs and symptoms of genital tract infection and how to reduce infection risk through good personal hygiene. Maternity staff should be aware of the signs, symptoms and management of maternal sepsis. If sepsis is suspected, high-dose intravenous broad spectrum antibiotics should be administered early.
- Serious incident reporting and maternal deaths: a high-quality local review should be undertaken following a maternal death involving clinicians from relevant disciplines, including those not directly involved with the death. The findings of the review should be disseminated to clinical staff, risk managers and administrators and steps taken to implement recommendations that should be regularly audited.
- Pathology: the standard of the maternal death autopsy must improve. A maternal autopsy may be complex and should be performed by specialist pathologists.
DIRECT DEATHS
Deaths due to sepsis have increased and replace thromboembolic disease as the most common cause of direct maternal death. Substandard care was identified in 70% of direct deaths.
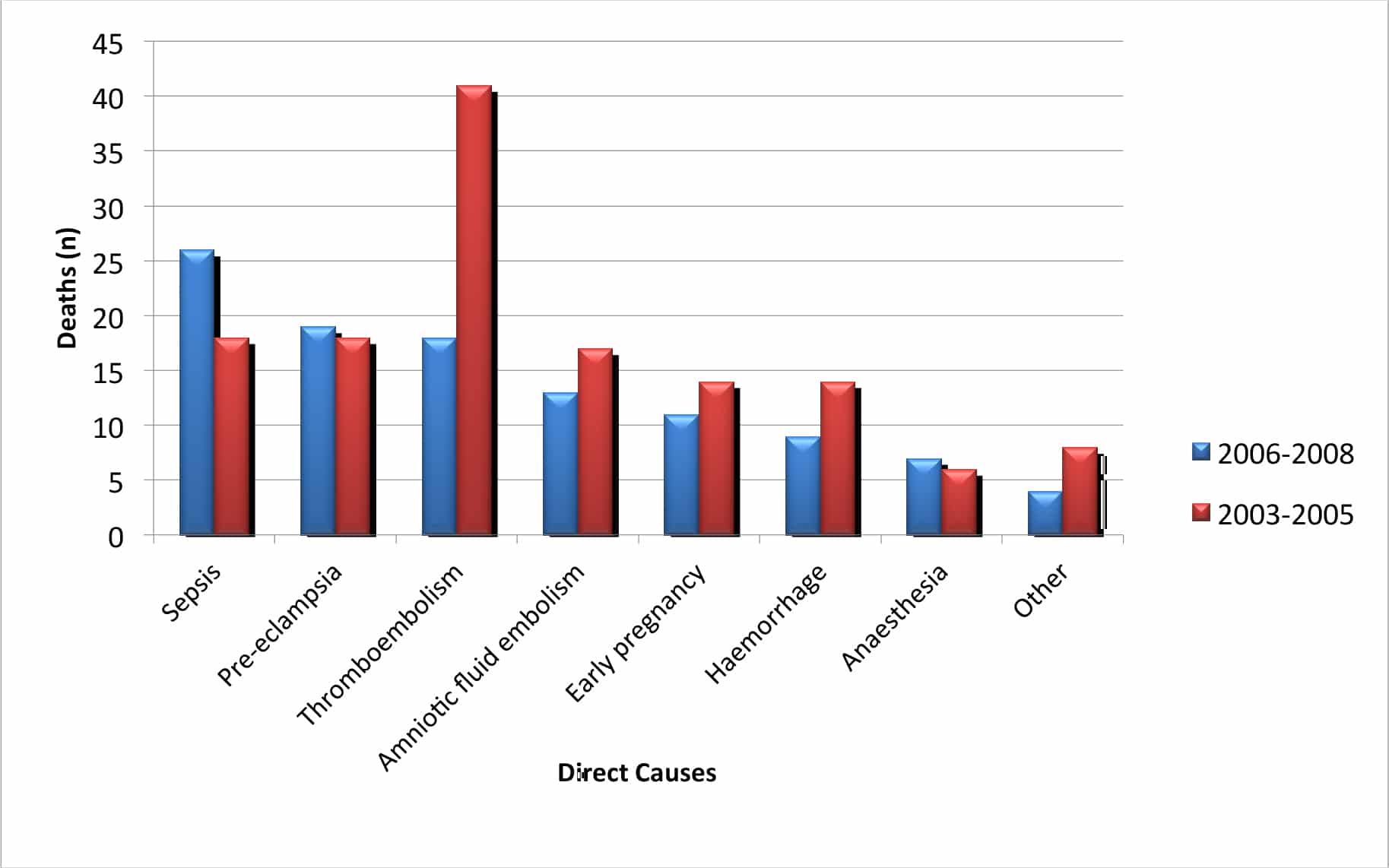
Figure 1. Direct causes of maternal death in the 2003-2005 & 2006-2008 triennia
Sepsis
Sepsis accounted for 26 deaths in this triennium – a maternal mortality rate of 1.13 per 100,000 compared to 0.85 per 100,000 in 2003-5. The increase is predominantly due to genital tract sepsis (24% of total direct deaths) chiefly a result of community acquired Group A streptococcal disease (isolated in half the women who died from sepsis). Nine women died following caesarean section and this highlighted the need for timely administration of prophylactic antibiotics. There were identifiable delays in seeking senior help or advice from anaesthetists and critical care specialists in six deaths from sepsis. Click here to view ATOTW 235 on Maternal Sepsis.
Pre-eclampsia
Of the 19 deaths, 14 died from intracranial haemorrhage and five from anoxia as a result of cardiac arrest following eclamptic seizures. Worryingly, 14 were considered to have received major substandard care due to inadequate antihypertensive therapy and failure of referral from the community for specialist care. It is unclear from this report whether failure to obtund the pressor response to larnyngoscopy following induction of general anaesthesia contributed to any of the deaths; however, such measures should always be undertaken in women with severe pre-eclampsia who require general anaesthesia. Click here to view ATOTW 158, ‘Pre-eclampsia a Case Based Discussion’
Thromboembolism
The number of women dying from thromboembolism (0.79 per 100,000 maternities) has fallen by more than 50% from the previous triennium and is the lowest since 1985. The reduced mortality was mainly observed in the antenatal period and in women who delivered vaginally. Obesity remains the most important risk factor. Fourteen women were overweight (BMI ≥ 25 kg/m2), of whom 11 had a BMI ≥ 30, and three had a BMI ≥ 40. Sixteen women died from pulmonary embolism and two from cerebral venous thrombosis. Click here to view ATOTW 207 on Venous Thromboembolic disease and Obstetric Anaesthesia
Amniotic Fluid Embolism
Deaths due to amniotic fluid embolism fell from 17 to 13 in this triennium probably due to improved resuscitation, prompt perimortem caesarean section and high-quality supportive care following collapse. The median age of those that died was 36. Eight women (62%) were parous, seven (54%) had pre-existing medical or psychiatric conditions and 16 (46%) were black African or Asian. Presenting features varied, however all were characterised by sudden and unexpected collapse. In 10 women (77%) the critical event occurred before or at delivery. Click here to view ATOTW 197 on Amniotic Fluid Embolism
Haemorrhage
Fewer women died as a result of haemorrhage compared to the previous triennium, but due to small numbers, it is not possible to confirm if this is a statistically relevant reduction. Of the nine women who died, six (66%) were considered to have received substandard care. Postpartum haemorrhage accounted for more than half the deaths and lack of postpartum observations were implicated in the majority. The management of both expected major haemorrhage in women with known placenta accreta and unexpected excessive intraoperative blood loss has improved. The importance of diagnosing and treating antenatal anaemia is highlighted as is the early involvement of senior multidisciplinary staff in cases of major obstetric haemorrhage. Click here to view ATOTW 41 on management of Obstetric Haemorrhage.
INDIRECT DEATHS
The mortality rate from heart disease (2.31 per 100,000 maternities) and suicide remains largely unchanged from the previous triennium. Substandard care was identified in 55% of indirect deaths.
Cardiac disease
Cardiac disease is the single most common cause of maternal death. Fifty of the 53 deaths were due to acquired heart disease – the leading causes being: sudden adult death syndrome (SADS), myocardial infarction, thoracic aortic dissection and cardiomyopathy. Death from SADS is presumed to result from an arrhythmia when other causes are excluded and is increasing in number. Half the women who died from cardiac disease had a BMI of >30 kg/m2. A degree of substandard care was identified in 27 (51%) deaths. Cases were identified in which there were failures to promptly diagnose, investigate or refer to appropriate specialists. The report emphasised the importance of a low threshold for investigation of women who complain of chest pain, especially if they have other risk factors including obesity, hypertension and a history of smoking. The report drew attention to the value of arterial blood gas analysis in women with known or potential underlying cardiac disease. Hypoxaemia may be a feature of pulmonary oedema and a metabolic acidosis may occur as a result of reduced cardiac output.
Opioid analgesia may mask cardiac symptoms. Consequently some women with cardiac disease, impending aortic dissection and other causes of death were not identified. Pregnant or recently delivered women with unexplained pain severe enough to require opioids should undergo urgent senior assessment.
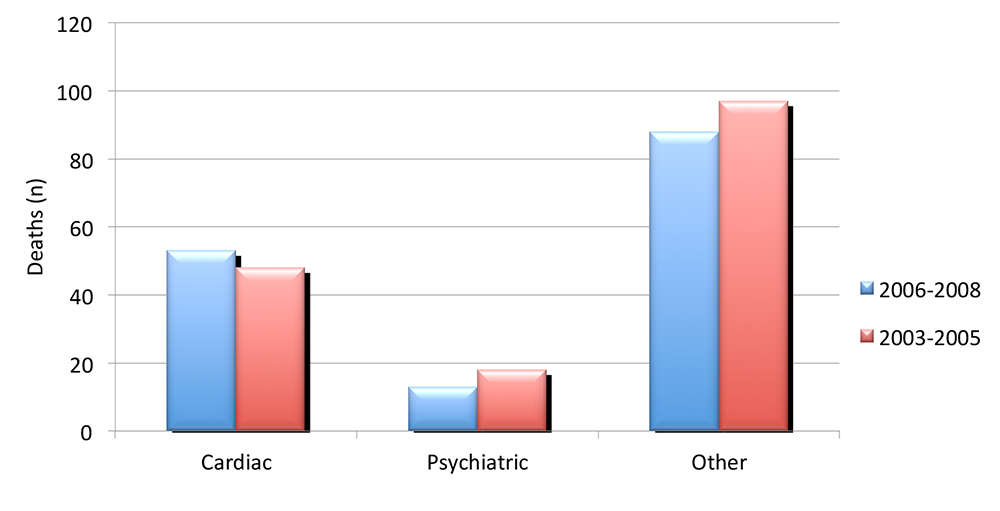
Figure 2. Indirect causes of maternal death in the 2003-2005 & 2006-2008 triennia
ANAESTHESIA RELATED DEATHS
Deaths relating to anaesthesia were the seventh leading cause of direct maternal death. There were seven direct deaths. Three were considered to have received major substandard care and three minor substandard care. All clinical staff involved in maternity care should appreciate and understand the risks of anaesthesia.
Failure to ventilate – two deaths
- A death occurred following induction of general anaesthesia. There were repeated attempts at intubation despite adequate oxygenation following insertion of an Intubating Laryngeal Mask Airway. The woman was coughing but was not allowed to wake up. A second dose of thiopental and a long-acting neuromuscular blocking agent were administered though capnography indicated the woman’s lungs were not being ventilated. A surgical airway was not attempted. This case was initially classed as a ‘Category 2’ caesarean section and the woman had a working epidural. The decision was made to top-up the epidural when the woman arrived in theatre, presumably, because of the anticipated time available to do this. However, following a sustained fetal bradycardia in theatre, an immediate caesarean section was required and general anaesthesia was provided and the events described above occurred. The report considered that general anaesthesia and the resulting complications may have been avoided had the epidural been topped-up immediately following the decision for delivery by caesarean section.
- A death occurred due to a dislodged tracheostomy tube in the Critical Care Unit. This occurred on turning the patient who had known airway problems and difficulties with her tracheostomy.
Post-operative complications –four deaths
- Opioid toxicity in a women using patient-controlled analgesia (PCA). Details of the death are limited and the cause was unspecified. PCA equipment and syringes were not retained for inspection.
- Acute circulatory failure possibly related to blood transfusion incompatibility.
- Cardiac arrest following general anaesthesia for surgical abortion. The patient was a regular substance abuser and intravenous syntometrine may have exacerbated underlying cardiac irritability.
- Probable aspiration of regurgitated gastric contents at emergence from general anaesthesia following a Category 1 caesarean section for a woman with known placenta praevia and antepartum haemorrhage.
Other – one death
Acute haemorrhagic leucoencephalitis. This is a rare form of acute disseminated encephalomyelitis with cross-reactivity between myelin and infectious agents. A woman died some days after an uneventful spinal for caesarean section. A spinal canal empyema was found at autopsy and it was considered that this may have triggered this rare condition. This highlights the importance of strict asepsis when performing neuraxial procedures.
ANAESTHESIA AS A CONTRIBUTORY FACTOR
In a further 18 maternal deaths, anaesthetic management was considered to have played a part or important lessons for the anaesthetist could be learned. A common contributory factor was the pressure of managing acutely unwell women or women with significant co-morbidities, on a busy maternity unit. Contingency plans should be in place to deal with times of excessive workload.
Specific issues included:
- Failure to consult with an anaesthetist or critical care specialist early (12 cases)
- Failure to recognise serious acute illness (10 cases).
- Obesity >30 kg/m2 (9 cases)
- Poor management of pre-eclampsia/ eclampsia (8 cases)
- Poor management of sepsis (6 cases)
- Poor management of postpartum haemorrhage (5 cases)
- Poor management of haemorrhage in early pregnancy (5 cases)
- Anaphylaxis (1 case)
- Thromboprophylaxis (1 case)
LESSONS FOR ANAESTHETISTS
The report identified a number of useful lessons from maternal deaths directly due to anaesthesia and from maternal deaths in which anaesthesia contributed. These include:
- Clinical skills
- Failed tracheal intubation is a core skill that should be rehearsed and assessed regularly. Failed intubation drills should be simple, readily available and well practiced.
- Improving basic, immediate and advanced life support skills should be an important part of multidisciplinary workforce training.
- Undertaking non-technical skills training, such as situational awareness, should help reduce human error and enhance communication within the team.
- Recognition of acute severe illness
- This involves a multidisciplinary approach with consultant level care and early anaesthetic involvement.
- The significant physiological reserve of healthy, pregnant women may mask the early signs of critical illness.
- Guidelines should be developed through local maternity networks to specify which medical conditions mandate consultant review in early pregnancy.
- There should be a protocol for rapid access to critical care specialists.
- Epidural anaesthesia for operative delivery
- A functioning epidural established in labour should be topped-up without delay to provide surgical anaesthesia.
- If there is delay in transfer to the operating theatre and the woman has a working epidural, it can be topped-up in the room to provide surgical anaesthesia, providing the anaesthetist and resuscitation equipment are immediately available and appropriate monitoring is provided.
- Full stomach
- Patients with a potentially full stomach undergoing general anaesthesia should be fully awake and able to protect their airway before extubation.
- In those known to have a full stomach, reducing the gastric volume and pressure by gentle ‘in and out’ insertion of a wide-bore orogastric tube before tracheal extubation should be considered.
- Severe pre-eclampsia
- All pregnant women with pre-eclampsia and a systolic BP of 150 – 160 mmHg or more require hospital admission and immediate anti-hypertensive treatment. The target systolic BP of 150mmHg is in line with recent National Institute for Health and Clinical Excellence (NICE) guidelines 2.
- These patients should undergo frequent and regular BP monitoring.
- A systolic BP >180mmHg constitutes a medical emergency and requires rapid treatment. These patients have an increased risk of fatal intracranial haemorrhage and aortic dissection.
- In patients with systolic BP <150mmHg, early treatment should be considered if progressive hypertension or clinical deterioration is anticipated. Examining trends in BP rather than absolute values is important. Early invasive arterial BP monitoring should be considered.
- Ergometrine should be avoided in the third stage of labour as this is known to worsen hypertension. The report recommends that intramuscular oxytocin and not Syntometrine should be used in these patients.
- Sepsis
- The management of sepsis and septic shock should be multidisciplinary with prompt diagnosis and early treatment.
- Surviving sepsis guidelines should be followed. This includes early administration of high-dose broad-spectrum intravenous antibiotics, careful fluid resuscitation, inotropic support and cardiovascular monitoring in a critical care environment 3.
- Early blood analysis, including blood culture, arterial gas and plasma lactate measurement should be performed.
- Surgery may be necessary to remove the source of the sepsis.
- Haemorrhage
- The recognition of postpartum haemorrhage may be impaired by a lack of monitoring in the early postpartum period.
- The symptoms and signs of hypovolaemia are difficult to recognise with any of the following: language difficulty, obesity, pre-eclampsia, brown/ black skin and beta-blockade.
- Those known to be at risk of major haemorrhage, e.g. women with placenta accreta or whom decline blood and blood products, should be delivered in maternity units with access to critical care, interventional radiology and cell salvage.
- The management of haemorrhagic shock should be multidisciplinary and led by senior staff.
Management includes surgery, intravenous fluid, blood and blood products and cardiovascular monitoring. - In cases of suspected uterine atony there should be a step-wise administration of uterotonics, escalating through syntocinon, ergometrine, prostaglandin F2α and misoprostol.
- Fluid resuscitation and inotropic support should be used cautiously before surgical control of haemorrhage has been achieved.
- Anaphylaxis
- A clear and easy to follow guideline that describes the management of acute anaphylaxis should be immediately available in all clinical areas.
- Thromboembolism
- Risk assessment in early pregnancy continues to be a key factor in reducing mortality.
- Inadequate thromboprophylaxis increases patient risk. Pharmacological thromboembolic prophylaxis dosage should be calculated on the basis of patient weight.
- Increased use of antenatal thromboprophylaxis, particularly in obese women, will have implications for neuraxial analgesia and anaesthesia.
- Vigilance is important. Chest symptoms occurring in pregnancy or following delivery demands careful assessment and a low threshold for investigation.
- Obesity
- Obesity is a significant problem and is increasing. Almost half the women that died from direct causes were overweight or obese. Around 40% of women who died from direct anaesthetic related causes were overweight of which two were obese.
- Being overweight or obese was associated with a greater risk of death from thromboembolism (78%) and cardiac disease (61%). In addition, obesity increases the risks of pre-eclampsia, gestational diabetes and critical care admission 4.
THE FUTURE OF THE CONFIDENTIAL ENQUIRIES
In April 2011, an Oxford-based group, Mothers and Babies: Reducing Risk through Audit and Confidential Enquiries across the UK (MBRRACE-UK) was due to take over the Confidential Enquiries from CMACE. However, in March 2011 this takeover was halted leading to confusion and uncertainty regarding the long term future of the project. A review at the end of 2011 reported that funding would continue and the Healthcare Quality Improvement Partnership (HQIP) will act as the body responsible for commissioning future reviews. It is likely that inclusion of morbidity as well as mortality will occur and, importantly, data from deaths occurring since the period covered by the current report would not be lost.
ANSWERS TO MCQs
- a. F
b. T
c. T
d. F
Cardiac disease related mortality was the most common cause of death. Sepsis was the leading direct cause of death. - a. T
b. F
c. T
d. T
Community acquired Group A streptococcal disease was the most common pathogen isolated in sepsis related deaths. - a. F
b. T
c. T
d. F
Ergometrine and Syntometrine (oxytocin and ergometrine) may worsen hypertension and increase the risk of adverse events including cerebral haemorrhage. They are contraindicated in hypertensive women. - a. F
b. T
c. F
d. T
78% of women who died as a result of thromboembolism were overweight or obese and this was the most significant risk factor
REFERENCES
- Centre for Maternal and Child Enquiries (CMACE). Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer: 2006–08. The Eighth Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG 2011;118 (Suppl. 1):1–203
- National Collaborating Centre for Women’s and Children’s Health. Hypertension in pregnancy: The management of hypertensive disorders during pregnancy. London (UK): National Institute for Health and Clinical Excellence (NICE); 2010 Aug. (Clinical guideline; no 107). [http://guidance. nice.org.uk/CG107]. Accessed 12 February 2012
- Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008 [published correction appears in Crit Care Med 2008; 36: 1394 –1396]. Crit Care Med 2008; 36: 296 –32
- Knight M, Kurinczuk JJ, Spark P, Brocklehurst P. Extreme obesity in pregnancy in the United Kingdom. Obstet Gynecol 2010; 115: 989– 97
FURTHER READING
UK Obstetric Surveillance System (UKOSS) https://www.npeu.ox.ac.uk/ukoss
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/