Neuroanaesthesia

Key Points
- The scalp block can be used for surgical and pain-management purposes
- Branches of the trigeminal and the cervical nerves are blocked
- The scalp is highly vascular, hence negative aspiration is needed before every injection to avoid intravascular injection
- Complications include direct nerve damage and injection into blood vessels which closely accompany the nerves
Introduction
The scalp is the soft tissue which covers the cranial vault excluding the facial bones. It is made of 5 layers and has a generous vascular and sensory nervous supply. Blocking these nerves can provide effective anaesthesia of the scalp.
A scalp block is a regional anaesthetic technique targeting the nerves that innervate the scalp. Scalp block is used for head and neck procedures, in surgery (such as neurosurgery, plastic surgery) and in acute and chronic pain management.
In neurosurgery, supplementing general anaesthesia with a scalp block can blunt painful response to pin application and scalp incision, and can reduce opioid requirements, promoting early emergence for neurological assessment. Modern advances in neurosurgery, especially awake craniotomy, have brought a resurgence in the use of this block.
This review presents the anatomy, technique, advantages, indications, contraindications, and complications of the scalp block.
Indications and Contraindications
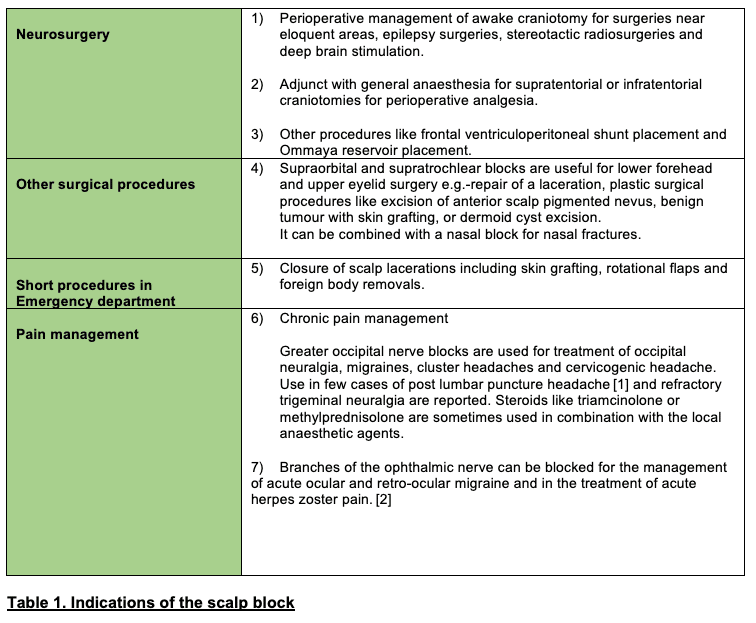
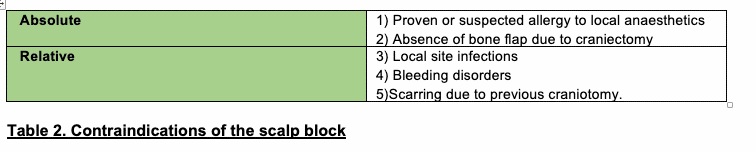
See Tables 1 and 2 for indications and contraindications, respectively.
Anatomy
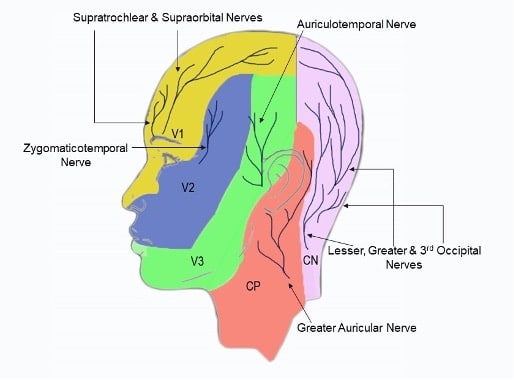
Figure 1. Dermatomes of the head and scalp . V1,V2,V3- Divisions of the Trigeminal nerve, CP- Cervical plexus, CN- Cervical spinal nerves.
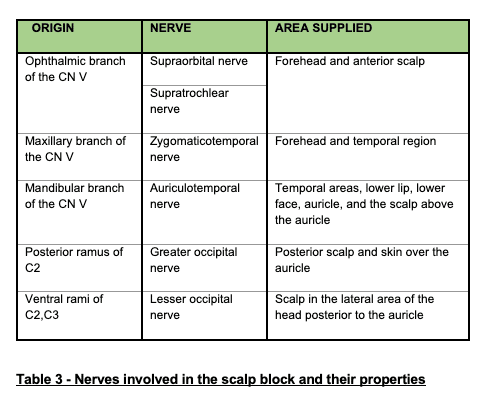
The frontal nerve enters the orbit through the superomedial aspect of the superior orbital fissure and divides into a larger lateral supraorbital nerve and a smaller medial supratrochlear nerve. Both these nerves supply the forehead and the anterior scalp. The supraorbital nerve travels anteriorly above the levator palpebrae superioris and exits the orbit through the supraorbital notch lateral to the supratrochlear nerve. The supratrochlear nerve leaves the orbit between the supraorbital notch and the trochlea, passing in a superior direction over the forehead.4
The zygomaticotemporal nerve innervates a small area of the forehead and the temporal region. It originates from the maxillary branch of thetrigeminal nerve. It passes through a small canal in the zygomatic bone and then arrives into the temporal fossa, where it passes superiorly between the bone and the temporalis muscle.4 It arises midway between the supraorbital and the auriculotemporal nerves and passes through the temporalis muscle to enter the temporalis fascia.
The auriculotemporal nerve innervates the temporal areas, lower lip, lower face, auricle, and the scalp above the auricle. It arises as 2 roots from the posterior division of the mandibular branch of the trigeminal nerve. This nerve crosses over the root of the zygomatic process of the temporal bone and lies posterior to the superficial temporal artery.5
The occipital nerves are a collection of nerves that originate from the cervical spinal nerves C2 and C3. They are located in the posterior neck and scalp regions and are interconnected through communicating branches. The greater occipital nerve runs between theobliquus capitis inferior and semispinalis capitis muscles. It then pierces the semispinalis capitis muscle and runs alongside the occipitalartery to innervate the posterior scalp and skin over the auricle. The lesser occipital nerve runs superiorly towards the skull along the posterior aspect of the sternocleidomastoid muscle, then piercing the deep cervical fascia to emerge onto the posterior aspect of theoccipital bone.6 It ascends along the posterior border of the sternocleidomastoid muscle innervating the scalp in the lateral area of thehead posterior to the auricle.
The scalp block has been reported to include an additional nerve, the great auricular nerve. It is the largest of the ascending branches of thecervical plexus. It arises from the C2 and C3 nerves, and its posterior branches supply the skin of the mastoid process and part of the back of theauricle. Minor contributions from the greater auricular nerve and third occipital nerve rarely encroach into the surgical field. While the landmarks where these nerves exit the skull are well defined, the dermatomal distribution exhibits enormous variability.
Technique
Equipment
The equipment needed for a scalp block includes the following: topical chlorhexidine 2% skin disinfectant solution, sterile gloves, gauze pieces, 25 gauge needle for injection, 20 mL syringe, and local anaesthesia (LA) drugs.
Drugs Used
Long-acting LA agents (0.25% bupivacaine, 0.75% ropivacaine, or 0.25% levobupivacaine) are administered with or without 5 μg/mL of 1:200,000 epinephrine. The addition of epinephrine serves to cause vasoconstriction and limit systemic absorption of local anaesthetic in intenselyvascularised areas like the scalp. The volume of LA administered at each injection site can vary from 2 to 5 mL.7
Additives to LA such as clonidine 2 μg/kg or dexmedetomidine 1 μg/kg8 have also been described, although such uses are unlicensed in some countries such as the United Kingdom.
Technique of Block7,9
Take the following precautions as preliminary steps:
- The technique of the block should be explained to the patient and informed consent obtained
- A ‘‘stop before you block’’ or ‘‘time-out’’ procedure should be performed to ensure correct site and laterality of the intended block.
- For surgical patients, this block can be performed after induction as an adjunct to general anaesthesia or at the end of surgery for postoperative analgesia.
- The injection sites should be disinfected with 2% Care should be taken to protect the eyes during this step.
The patient lies supine on the table while the performing operator usually stands at the head end facing the feet. Sedation is recommendedduring administration of the block as it can be painful. Oxygen can be provided by a nasal cannula with moderate sedation and capnometry shouldbe used. A combination of propofol and/or remifentanil or dexmedetomidine can be used for sedation. Doses of sedatives should be titrated to achieve a Ramsay sedation score of 2 to 3 to prevent oversedation and hypoventilation, especially in elderly patients and those with neurological deficits.
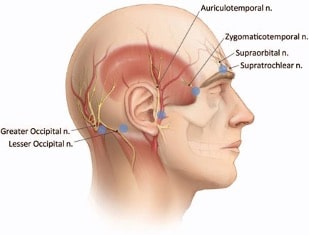
Fig 2. Injection points for nerves of the scalp block shown by blue dots.
Source: Kemp 3rd WJ et al. under the creative commons attribution 2.5 license 2006
Most of the injections are superficial subcutaneous injections and should produce a wheal on injection. Gentle massage after injection with a piece of gauze helps in the spread of LA. Figure 2 depicts the injection sites, described below.
Supraorbital Nerve
This block is performed with the patient’s head facing forward and eyes closed. The supraorbital nerve can be blocked as it exits through the orbit. The supraorbital notch is located by palpation, and the needle is introduced perpendicularly 1 cm medial to the notch. About 2 to 3 mL of LA is injected just superficial to the periosteum.
Supratrochlear Nerve
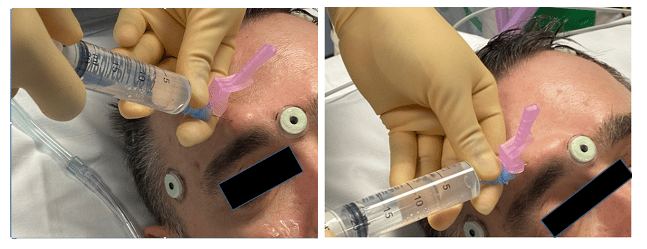
Figure 3 – Conduct of the suprorbital (left) and the supratrochlear (right) nerve block. The supratrochlear block is a medial extension of the supraorbital block
The position for this block is similar to the supraorbital block. The supratrochlear nerve runs parallel to the supraorbital nerve about 1 fingerbreadth medial to it above the eyebrow. Once the supraorbital nerve is blocked, the needle is directed medially through the same insertionpoint and a subcutaneous injection of 2 to 3 mL here will block the supratrochlear nerve (Figure 3).
Zygomaticotemporal Nerve
This block is performed with the patient’s head turned to one side so that the side to be blocked faces upward. The zygomaticotemporal nerve ramifies as it pierces the temporalis fascia, hence both subcutaneous and deep injections are needed to block this nerve. Infiltration begins with 5mL of LA at the lateral edge of the supraorbital margin and continues to the

Figure 4 – Conduct of the zygomaticotemporal block. The dotted lines show the supraorbital margin and the zygomatic arch.
distal aspect of the zygomatic arch. The injection point is at the outermost edge of the supraorbital margin (the concave portion of the lateral orbitalrim). The angle of the needle should be 90 degrees till bone is contacted, where the operator can deposit 1 to 2 mL of LA here as a deep injection.The needle is then redirected laterally to reach the outermost aspect of the zygomatic arch, and another 3 to 4 mL of LA is deposited along this trajectory (the supraorbital margin and zygomatic arch are marked with dotted lines in Figure 4).
Auriculotemporal Nerve
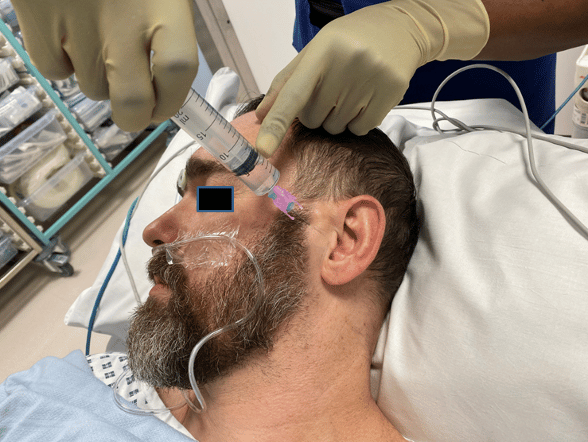
Figure 5 – Conduct of the auriculotemporal block.
Position for this block is similar to the zygomaticotemporal block. This nerve can be blocked by injecting approximately 3ml of LA 1 to 1.5 cm anterior to the ear at the level of the tragus above the level of the temporomandibular joint (Figure 5). The superficial temporal artery should be palpated to avoid intra-arterial injection. Negative aspiration is a must for this block. The injection is superficial and subcutaneous as a deep plane injection can cause a facial nerve block.
Greater Occipital Nerve
This block can be performed by turning the head to the side or with the patient sitting up. The greater occipital nerve can be blocked by infiltrating LA subcutaneously halfway between the occipital protuberance and the mastoid process, 2.5 cm lateral to the nuchal median line (Figure 6). The best landmark is to palpate the occipital artery (found about 3 to 4 cm lateral to the
external occipital protuberance along the superior nuchal line), and inject medial to the artery after careful aspiration. This should avoid potentialintra-arterial injection. The needle is inserted at a 90 degree angle towards the occiput until bony contact is obtained, then withdrawn to make a subcutaneous injection here with 5 mL of LA to block the greater occipital nerve.
Lesser Occipital Nerve
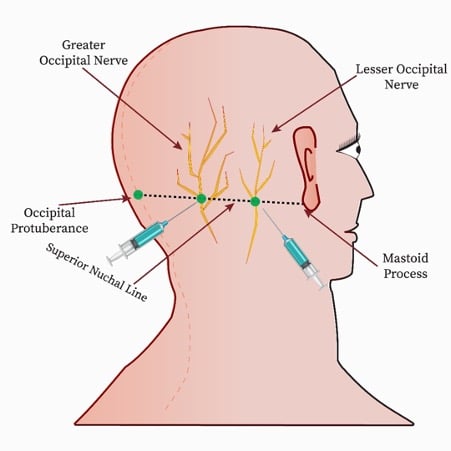
Figure 6- Conduct of the greater and lesser occipital nerve blocks.
The position for this block is similar to the greater occipital nerve. The block is made subcutaneously by injecting 5 mL of LA 2.5 cm lateral to the greater occipital nerve along the superior nuchal line (Figure 6).
Great Auricular Nerve
The postauricular branches of the great auricular nerve may be blocked with an injection of 3 to 5 mL of LA subcutaneously between the skin and bone, 1.5 cm posterior to the ear at the level of the tragus. The needle is inserted at 90 degrees till bony contact is made, upon which it is withdrawn and subcutaneous injection is performed.
Complications
- Anaphylaxis in response to LA
- Toxicity of LA. Epinephrine as an additive can lessen systemic absorption of LA and hence limit the acute rises in its plasma level. The anaesthetist must adhere to the maximum recommended LA dose and be vigilant in the first 15 minutes after the block to detect signs of toxicity.
- Haemodynamic changes and arrhythmias due to systemic absorption of epinephrine. Caution is advised in patients with coronary heart disease and negative aspiration recommended to avoid inadvertent intravascular injection.
- Vascular injury and hematoma formation due to proximity of nerves to blood vessels. (Note that the auriculotemporal nerve and the greater occipital nerve are adjacent to the superficial temporal and occipital arteries, respectively.)
- Pain. Intraneural injection may cause immediate severe pain. This risk is especially significant in the case of the supraorbital nerve block due to its anatomical position. A major advantage of the scalp block is that most of the nerves that innervate the scalp are superficial terminal sensory branches, and the risk of nerve damage is less than that for the deeper motor nerves.10
- Facial nerve palsy. This is a relatively rare complication and can occur during the auriculotemporal or zygomaticotemporal injections due to their proximity to the facial nerve. This is usually transient, due to blockade of the facial nerve by the LA rather than a permanent injury to the nerve. Causes range from deep injections, compression from a haematoma, oedema, or the pressure of an LA injection and vasoconstriction-induced neural ischaemia due to epinephrine. Facial palsy occurs at a rate of 8.6% after an auriculotemporal block.11
- Intracerebral or subarachnoid injection. This has been reported in patients with bony defects or previous craniectomies.12
- Bradycardia and hypotension. A trigeminocardiac reflex during the scalp block can present as severe bradycardia and hypotension. It can be provoked by mechanical, electrical, or chemical stimulation of any sensory branch of cranial nerve V. This has been described with peripheral branches involved in the scalp block as well. Caution is advised while anaesthetizing the trigeminalnerve as rapid LA infiltration can compress or stretch the nerve, thus triggering this reflex.13
- Unilateral ptosis. This may occur due to excessive LA infiltration, leading to injury or oedema in the muscles responsible for eyelid retraction.
- Infection. This is possible, though rare.
Discussion
Scalp Block in Paediatric Patients
The technique is similar to that used for adults, but lower doses and volumes are advised. Usual choice of LA includes 0.25% bupivacaine orlevobupivacaine (2 mg/kg) with 2.5 μg/mL of epinephrine.14 Care is taken to not exceed the maximum LA dose according to the weight of the child.
Scalp Infiltration Versus Scalp Block
A scalp block is targeted at the nerves supplying the scalp and hence a lesser volume of drug is needed compared to scalp infiltration. A scalp block also has a longer duration of action.
Alternate Approach
In 2016, an alternate approach describing the use of a maxillary block along with greater and lesser occipital nerve blocks found better analgesiacompared to a regional scalp block in craniotomy patients. This approach relies on the retrograde spread of the anaesthetic along the maxillary nerve, leading finally to a complete block of all branches of the ipsilateral trigeminal nerve.15
Summary
- The scalp block is a safe and easy technique having many advantages for intra and postoperative pain relief in various surgeries.
- Nerves supplying the scalp are targeted in a systematic manner on each side.
- Complications include direct nerve damage and injection into blood vessels which closely accompany the nerves.
References
- Matute Bilateral greater occipital nerve block for post-dural puncture headache. Anaesthesia. 2008;63(5):557-558.
- Countryman NB, Hanke Practical review of peripheral nerve blocks in dermatologic surgery of the face. Curr Dermatol Rep. 2012;1(2):49-54.
- Kemp WJ 3rd, Tubbs RS, Cohen-Gadol AA. The innervation of the scalp: a comprehensive review including anatomy, pathology, and neurosurgical correlates. Surg Neurol Int. 2011;2:178.
- Rea Essential Clinically Applied Anatomy of the Peripheral Nervous System in the Head and Neck. 1st ed. Cambridge, MA: Academic Press; 2016.
- Komarnitki I, Andrzejczak-Sobocin´ska A, Tomczyk J, et Clinical anatomy of the auriculotemporal nerve in the area of the infratemporal fossa. Folia Morphol. 2012;71(3):187-193.
- Netter, Atlas of Human Anatomy.7th ed. Philadelphia, PA: Saunders; 2019.
- Pinosky ML, Fishman RL, Reeves ST, et al. The effect of bupivacaine skull block on the hemodynamic response to craniotomy. Anesth Analg. 1996;83(6):1256-1261.
- Vallapu S, Panda NB, Samagh N, et Efficacy of dexmedetomidine as an adjuvant to local anesthetic agent in scalp block and scalpinfiltration to control postcraniotomy pain: a double-blind randomized trial. J Neurosci Rural Pract. 2018;9(1):73- 79.
- Costello TG, Cormack Anaesthesia for awake craniotomy: a modern approach. J Clin Neurosci. 2004;11(1):16-19.
- Osborn I, Sebeo ‘‘Scalp block’’ during craniotomy: a classic technique revisited. J Neurosurg Anesthesiol. 2010;22(3):187-194.
- Liguori GA. Complications of regional anesthesia: nerve injury and peripheral neural blockade. J Neurosurg Anesthesiol. 2004;16(1):84-86.
- Okuda Y, Matsumoto T, Shinohara M, et Sudden unconsciousness during a lesser occipital nerve block in a patient with the occipital bone defect. Eur J Anaesthesiol. 2001;18(12):829-832.
- Schaller B, Cornelius JF, Prabhakar H, et The trigemino-cardiac reflex: an update of the current knowledge. J Neurosurg Anesthesiol. 2009;21(3):187-195.
- Suresh S, Voronov Head and neck blocks in children: an anatomical and procedural review. Pediatr Anaesth. 2006;16(9):910-918.
- Jayaram K, Srilata M, Kulkarni D, et Regional anesthesia to scalp for craniotomy: innovation with innervation. J Neurosurg Anesthesiol. 2016;28(1):32-37.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
WFSA Disclaimer
The material and content provided has been set out in good faith for information and educational purposes only and is not intended as a substitute for theactive involvement and judgement of appropriate professional medical and technical personnel. Neither we, the authors, nor other parties involved in its production make any representations or give any warranties with respect to its accuracy, applicability, or com- pleteness nor is any responsibility accepted forany adverse effects arising as a result of your reading or viewing this material and content. Any and all liability directly or indirectly arising from the use of this material and content is disclaimed without reservation.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/