General Topics

KEY POINTS
- Cigarette smoking increases the risk of perioperative morbidity and
- Surgery represents a ‘teachable moment’ for smoking cessation when patients may be more motivated to quit smoking to reduce their perioperative risk.
- Anaesthetists should ask every patient of their smoking status, advise smoking cessation as soon as possible preoperatively and support patients through referral to trained clinicians for smoking cessation.
- There are a range of effective pharmacologic and nonpharmacologic smoking cessation methods available for which anaesthetists should be familiar.
- There is insufficient evidence to support the safety or effectiveness of e-cigarettes in smoking cessation
INTRODUCTION
Tobacco smoking is a leading cause of preventable morbidity and premature death worldwide, eventually killing half of all smokers and contributing to an estimated 8 million deaths annually.1 In Australia, there are approximately 21,000 deaths related to tobacco use annually, with the total burden of disease costing the economy an estimated $31.5 billion in tangible costs.2 Through successful public health policies, many high-income countries have experienced a significant decline in the rate of tobacco use.1
Most smokers regret their habit and want to quit smoking, but due to the addictive nature of nicotine, only 2% to 3% of smokers are able to quit without additional support.3 The perioperative period represents a vital opportunity for anaesthetists to promote and support smoking cessation, with surgery being a strong motivator to quit smoking. Many patients will quit smoking briefly during the perioperative period, but permanent cessation without ongoing assistance is rare.4 Patients should be aware that smoking increases their risk of postoperative pulmonary, cardiovascular, neurologic and wound complications; general infections; and postoperative pain and increases their risk for intensive care unit (ICU) admission and prolonged hospitalisation.5 Many professional societies or associations including the Australian and New Zealand College of Anaesthetists, Royal College of Anaesthetists and American Society of Anesthesiologists recommend that anaesthetists use the perioperative period as a ‘teachable moment’ to promote smoking cessation before surgery. A Cochrane review3 has demonstrated that even brief advice provided by doctors increases the likelihood of sustained smoking cessation. Despite this, an Australian study demonstrated that of 133 elective surgical patients surveyed, 22.6% did not receive any advice preoperatively about smoking cessation, and only 9% of patients reported receiving specific advice from their anaesthetist.4
Barriers to clinicians initiating interventions perioperatively may include insufficient knowledge or training on this topic, time constraints, lack of multidisciplinary support or funding and limited ability to provide follow-up.6
In this article, we will update the information provided in tutorial 221 (from 2011) by discussing the pathophysiological effects of smoking on perioperative morbidity and mortality as well as review the efficacy of the main interventions used to support smoking cessation.
CONSTITUENTS OF CIGARETTE SMOKE
Tobacco smoke consists of particulate matter suspended in a gaseous phase of nitrogen, oxygen, carbon monoxide and carbon dioxide and contains more than 7000 chemicals, of which more than 70 are known carcinogens.7 The main component of the gaseous phase is carbon monoxide, whilst the particulate phase is predominantly nicotine.8 Nicotine is responsible for the main physiological and addictive qualities of cigarettes through its agonism of the nicotinic acetylcholine receptor. Haemoglobin combines with carbon monoxide with an affinity 250-fold greater than that for oxygen to form carboxyhaemo- globin, which has a half-life of approximately 4 hours.9 This creates a left shift in the oxyhaemoglobin dissociation curve, reducing oxygen delivery to the tissues. Carboxyhaemoglobin levels in smokers are up to 15% of total haemoglobin compared with ,1% in nonsmokers.
PATHOPHYSIOLOGICAL EFFECTS OF SMOKING AND CONSIDERATIONS FOR ANAESTHESIA
Cardiovascular
Smoking is a major modifiable risk factor for cardiovascular disease and is the greatest preventable cause of cardiovascular morbidity and mortality, with smokers having a 3-fold greater risk of cardiovascular death than never-smokers do.10 Nicotine promotes resetting of the carotid and aortic baroreceptors, increasing sympathetic tone and resulting in hypertension, tachycardia, increased systemic vascular resistance and myocardial contractility.9 The increase in heart rate, contractility and afterload combined with reduced oxygen delivery caused by carboxyhaemoglobin impairs the myocardial oxygen supply- demand relationship and may precipitate myocardial ischaemia and arrhythmias. Smoking promotes polycythaemia, thrombocytosis, enhanced platelet reactivity and atherosclerosis, which increases the risk of thromboembolic events such as stroke and myocardial infarction.9 Patients who smoke have an increased risk of cardiovascular complications perioperatively, including myocardial infarction (odds ratio [OR] 1.80, 95% confidence interval [CI] 1.11-2.92), stroke (OR 1.73, 95% CI 1.18-2.53) and cardiac arrest (OR 1.57, 95% CI 1.10-2.25).5 Passive smokers are also at increased risk of cardiovascular morbidity and mortality.
Respiratory
The respiratory system is exposed to the greatest concentration of toxic substances from cigarette smoke, resulting in damage and disease to the entire respiratory system including lung cancer and chronic obstructive pulmonary disease (COPD). Ninety percent of lung cancer deaths, and 60% of all pulmonary deaths, are related to active or passive smoking.10 Cigarette smoke impairs mucociliary clearance by damaging cilia and causing thickening of mucous, resulting in chronic mucous retention and chronic cough.10 Smoking impairs the innate immune defences, causes chronic inflammation and predisposes smokers to respiratory tract infections, including pneumonia.10 Toxins in cigarette smoke cause parenchymal lung damage through oxidative damage and release of proteinases, which promote destruction of the extracellular matrix and apoptosis of pneumocytes, resulting in COPD in 30% of smokers.2,10
Active and passive smokers have an increased risk of perioperative adverse respiratory events including coughing, apnoeas, laryngospasm, bronchospasm, hypoxia and perioperative respiratory failure requiring ICU admission.5,9,11 Smokers are predisposed to hypoxaemia perioperatively due to
- Reduction in functional residual capacity
- Atelectasis
- Increased closing capacity
- Impaired ventilation-perfusion (V/Q) matching with shunt
The anaesthetist must be cognisant of the increased risk of respiratory complications in smokers on induction and emergence from general anaesthesia. The risk of adverse events is influenced by the patient’s pack-year smoking history. The greater the number of pack-years smoked, the greater the likelihood of smoking-related disease and the greater the risk of adverse perioperative events.5 Avoidance of general anaesthesia in preference for regional anaesthesia should be considered where possible, particularly in heavy smokers. Prior to induction of general anaesthesia, the anaesthetist should ensure appropriate positioning for induction and effective preoxygenation and be prepared to manage bronchospasm and hypoxia. It is important to ensure that effective multimodal analgesia is prescribed, including regional analgesia where possible, to improve ventilation postoperatively and facilitate early mobilisation.
Metabolic
Cigarette smoke induces the cytochrome P450 (CYP450) enzyme system, principally through effects of polycyclic aromatic hydrocarbons on CYP1A1, CYP1A2 and CYP2E1 as well as the phase 2 enzyme UGT2B7.8 Enzymatic induction occurs maximally within 24 hours of smoking. Metabolism of many drugs including codeine, theophylline, caffeine, haloperidol and volatile anaesthetics are altered.8Pharmacokinetically important drug effects of cigarette smoking for the anaesthetist that may result in an increased dose requirement include the following8:
- Fentanyl and sufentanil: CYP3A4 induction
- Rocuronium and vecuronium: CYP1A2 and possibly CYP3A4 induction
- Theophylline: CYP1A2 induction
- Ropivacaine: CYP1A2 induction
Dose requirements for rocuronium and vecuronium may be increased by up to 25% in smokers. This is likely multifactorial, due to both enzymatic induction and nicotine-induced changes in the sensitivity of the neuromuscular junction to acetylcholine in smokers.8 Further research into the clinical relevance of these changes is required, and no change to the dosing of aminosteroid muscle relaxants is needed.
Smoking is associated with a reduced risk of postoperative nausea and vomiting (PONV). The mechanism of this reduction is multifactorial but may include enhanced metabolism of volatile anaesthetics by CYP2E1 and reduced sensitivity to the emetogenic effects of surgery and anaesthesia.8,9 Needless to say, a reduction in PONV should not be used as a reason to continue smoking perioperatively, and smokers should be encouraged to quit as early as possible before surgery.
Neurologic
Smoking is a modifiable risk factor for poor postoperative pain control (OR 1.33, 95% CI 1.09-1.61), with smokers consistently demonstrating higher pain scores and greater opioid requirements than nonsmokers do.12 Although cigarette smoke induces UGT enzymes, higher opioid requirements in smokers likely reflects altered pain thresholds and pharmacodynamic changes in receptor sensitivity to opioids, rather than enhanced elimination.8,9
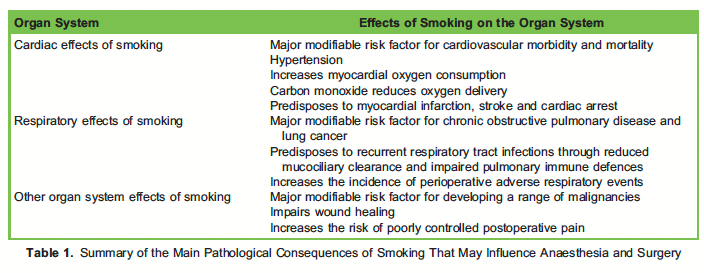
Smoking has been identified as a major modifiable risk factor for developing dementia, and there is growing evidence that smokers are more likely than never-smokers to develop postoperative delirium.10 Table 1 summarises the pathophysiological effects of smoking.
ASSISTING PATIENTS TO QUIT SMOKING BEFORE SURGERY
Anaesthetists should use surgery as a teachable moment to promote smoking cessation by motivating patients to quit and referring them to an appropriate expert such as their general practitioner or quit counsellor. The American Society of Anesthesiologists’ Smoking Cessation Initiative Taskforce 3-point cessation strategy is a quick and simple tool that anaesthetists and surgeons can use preoperatively to promote smoking cessation.13 The key elements include
- Ask: Ask every patient about their smoking status
- Advise: Advise smokers of the specific perioperative risks of smoking as outlined above, in addition to the general risks of smoking to their long-term Patients are more likely to quit smoking preoperatively if they understand the risks smoking poses to their health in the perioperative period and the reduction in risk associated with smoking cessation.
- Refer: Refer patients to their general practitioner, addiction specialist, quit helpline, smoking cessation counsellor or pharmacist for further assessment and management. Pharmacologic and nonpharmacologic support increases long-term smoking cessation rates.
Timing of Smoking Cessation
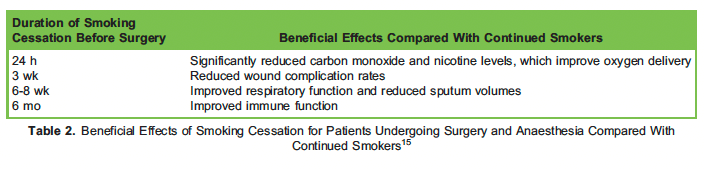
Patients who smoke should be encouraged to quit smoking as early as possible before planned surgery. Smokers who quit 4 weeks prior to planned surgery have a lower risk of wound complications and reduced postoperative opioid consumption.10,14 The ideal cessation time varies depending on the specific complication and the type of surgery.14 It is not clear whether smoking cessation hours to days before surgery reduces complications; however, there is also no evidence that recent cessation increases the risk of any complication compared with continued smokers.10,14 The benefits of preoperative smoking cessation that may be discussed with the patient are outlined in Table 2.
Nonpharmacologic Support
In addition to pharmacologic measures, all smokers should be provided with access to counselling services to maximise their chance of permanent smoking cessation. The cornerstone of nonpharmacologic management is individual or group counselling.
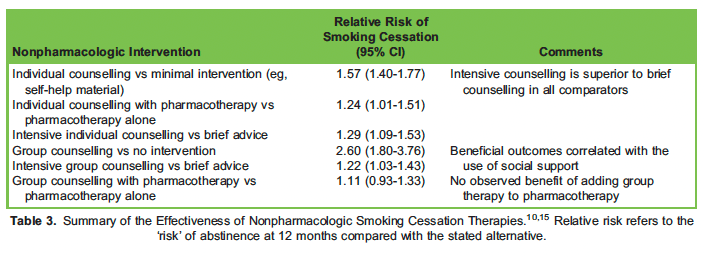
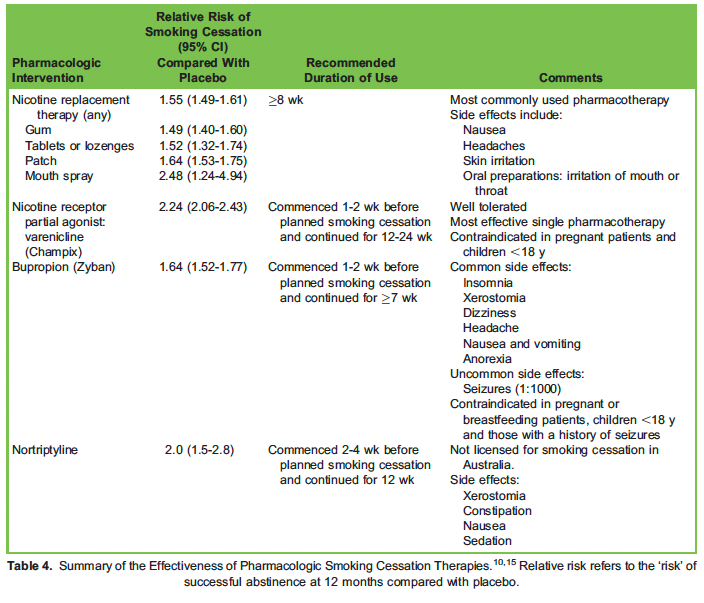
Table 3 demonstrates that both individual and group counselling are independently effective in increasing the likelihood of smoking cessation, with intensive therapies being more effective than brief counselling. Individual counselling was shown to further augment smoking cessation rates when combined with pharmacotherapies outlined in Table 4, although this same effect was not seen with group therapy plus pharmacotherapy. Counselling is best conducted by a trained psychologist or quit counsellor. Examples of counselling techniques include the following10:
- Cognitive behavioural therapy: addresses the emotional, cognitive and situational aspects of smoking through behavioural and cognitive strategies.
- Acceptance and commitment therapy: teaches acceptance and tolerance of cravings whilst maintaining a commitment to smoking abstinence through value-focused behavioural change.
- Motivational interviewing: explores a patient’s ambivalence, motivations and confidence to quit smoking and aims to strengthen their resolve to quit through goal-oriented counselling.
- Mindfulness: focuses on meditation to reduce cravings and promote enhanced self-
Smoking aversive therapy involves pairing smoking with unpleasant stimuli such as electric shocks, unpleasant odours, imagining unpleasant situations or rapid smoking (taking a puff every few seconds). At present, there is insufficient evidence to support smoking aversive therapies as mainstream therapy.10
Acupuncture techniques including needling, acupressure and laser therapy have demonstrated weak short-term effects but no beneficial long-term effects on smoking cessation. The need for weekly acupuncture sessions for several months may reduce treatment compliance and thus long-term efficacy.10
Pharmacologic Support
Several cessation pharmacotherapies are independently effective in achieving sustained smoking cessation and are more effective than self-help materials or no treatment.10 Table 4 demonstrates the effectiveness of first-line smoking cessation medications.
[table id=14 /]
[table id=15 /]
[table id=16 /]
Nicotine Replacement Therapy
Nicotine replacement therapies (NRTs) are used to partially replace nicotine from cigarettes, reducing withdrawal symptoms and increasing smoking cessation rates. NRTs are available as sustained-release patches that reduce background cravings and immediate-release forms (tablets or lozenges, mouth sprays, nasal sprays and inhalers) that are suitable to attenuate sudden cravings. Combined patch and fast-acting NRTs are superior to single-form NRTs.10
Varenicline (Champix)
Varenicline is a nicotinic acetylcholine receptor (nAChR) partial agonist that inhibits nicotine binding to the nAChR to reduce the effect of nicotine and promotes dopamine release to reduce withdrawal symptoms.10 Varenicline is the most effective single pharmacotherapy for smoking cessation and is as effective as combination nicotine replacement therapy (fast-acting form plus patch).
Bupropion (Zyban)
Bupropion is a selective reuptake inhibitor of noradrenaline and dopamine that is commonly prescribed as an antidepressant but is also used as a nonnicotine-based medication for smoking cessation. The exact mechanism of action in supporting smoking cessation is not known, but its use is associated with reduced cravings and withdrawal symptoms and potential reduction in depressed mood. Bupropion appears to be as efficacious as standalone NRT but inferior to varenicline or combination NRT.
Electronic cigarettes
E-cigarettes are increasingly used by smokers for cessation therapy. Users of e-cigarettes inhale a vaporised solvent containing nicotine, water, glycerine, propylene glycol and flavouring in aerosol form, rather than smoke.16 E-cigarettes are likely to be less harmful than cigarettes but should not be considered as a safe alternative to the pharmacologic smoking cessation therapies listed in Table 4. There is insufficient evidence to determine whether e-cigarettes improve smoking cessation rates and reduce harm for users, and there is no evidence to support their long-term safety.10 There is also public health concern that the ready availability of e-cigarettes may promote nonsmokers or ex-smokers to commence e-cigarette use and potentially develop nicotine addiction. As such, the Australian government has restricted e-cigarette access, with users requiring a prescription from their medical practitioner to access e-cigarette products.
SUMMARY
Tobacco smoking significantly increases the risk of perioperative morbidity and mortality, and patients should be encouraged to quit smoking as soon as possible prior to their planned operation. Surgery represents a teachable moment for smoking cessation when patients may be more motivated to quit smoking to reduce their perioperative risk. Anaesthetists play a vital role as perioperative clinicians to assess smoking status and support cessation and thus require knowledge of the available cessation therapies and referral pathways. There are a range of effective pharmacologic and nonpharmacologic cessation strategies available to support smoking cessation.
REFERENCES
- World Health WHO Report on the Global Tobacco Epidemic, 2021: Addressing New and Emerging Products. Geneva, Switzerland: World Health Organisation; 2021.
- Australian Institute of Health and Welfare. Tobacco smoking. 2021. Accessed November 8, 2021. https://www.aihw.gov. au/reports/australias-health/tobacco-smoking
- Stead LF, Buitrago D, Preciado N, et Physician advice for smoking cessation. Cochrane Database Syst Rev. 2013(5):CD000165.
- Webb AR, Robertson N, Sparrow Smokers know little of their increased surgical risks and may quit on surgical advice.
ANZ J Surg. 2013;83(10):753-757. - Turan A, Mascha EJ, Roberman D, et Smoking and perioperative outcomes. Anesthesiology. 2011;114(4):837-846.
- Sharpe T, Alsahlanee A, Ward KD, Doyle Systematic review of clinician-reported barriers to provision of smoking cessation interventions in hospital inpatient settings. J Smoking Cess. 2018;13(4):233-243.
- Centers for Disease Control and Prevention (US); National Center for Chronic Disease Prevention and Health Promotion (US); Office on Smoking and Health (US). How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Atlanta (GA): Centers for Disease Control and Prevention (US); 2010. Available from: https://www.ncbi.nlm.nih.gov/books/NBK53017/ (Accessed 18th March 2022)
- Sweeney BP, Grayling Smoking and anaesthesia: the pharmacological implications. Anaesthesia. 2009;64(2):179-186.
- Nariani J, Palmer Effects of smoking on health and anaesthesia. Anaesth Intensive Care. 2010;11(4):129-130.
- Greenhalgh E, Scollo M, Winstanley M. Smoking cessation. Tobacco in Australia: Facts and issues. 2020. Accessed November 12, 2021. http://www.tobaccoinaustralia.org.au/chapter-7-cessation
- Grønkjær M, Eliasen M, Skov-Ettrup LS, et Preoperative smoking status and postoperative complications: a systematic review and meta-analysis. Ann Surg. 2014;259(1):52-71.
- Schug S, Palmer GM, Scott DA, Alcock M, Halliwell R, Mott JF. Acute pain management: scientific evidence. 2020. Accessed December 1, 2021. https://www.anzca.edu.au/resources/college-publications/acute-pain-management/apmse5. pdf
- Warner DO. Feasibility of tobacco interventions in anesthesiology practices: a pilot study. Anesthesiology. 2009;110(6):1223-1228.
- Yoong S, Tursan d’Espaignet E, Wiggers J, et al. WHO tobacco knowledge summaries: tobacco and postsurgical outcome. Accessed November 13, 2021. https://apps.who.int/iris/bitstream/handle/10665/330485/9789240000360- eng.pdf
- Australian and New Zealand College of Guideline on smoking as related to the perioperative period. PG12. 2014. Accessed November 13, 2021. https://www.anzca.edu.au/getattachment/a3591188-1d7d-41cf-807a-b3b2f0226109/ PG12(POM)BP-Guideline-on-smoking-as-related-to-the-perioperative-period-Background-Paper-(PS12BP)
- Krusemann EJZ, Havermans A, Pennings JLA, et al. Comprehensive overview of common e-liquid ingredients and how they can be used to predict an e-liquid’s flavour category. Tob Control. 2021(30):185-191.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
WFSA Disclaimer
The material and content provided has been set out in good faith for information and educational purposes only and is not intended as a substitute for the active involvement and judgement of appropriate professional medical and technical personnel. Neither we, the authors, nor other parties involved in its production make any representations or give any warranties with respect to its accuracy, applicability, or completeness nor is any responsibility accepted for any adverse effects arising as a result of your reading or viewing this material and content. Any and all liability directly or indirectly arising from the use of this material and content is disclaimed without reservation.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/