Patient Safety

KEY POINTS
- Every member of the operating theatre team should feel empowered to speak up when a potential error may occur.
- Education on strategies for speaking up among team members should be encouraged.
- Assertiveness and speaking up must be coupled for effective communication in the clinical environment.
INTRODUCTION
Communication in the operating room (OR) is challenging: there is a flux of many specialties; complex patients; background noise, including monitors and surgical equipment; and a variety of procedures that require prompt decision making. The styles of communication can differ between surgical specialties, anaesthesiologists, specialty trainees, and nursing staff; therefore, working in a psychologically safe environment, where anyone would feel able to raise concerns, is paramount.1
Organizational cultures that promote psychological safety among team members provide safer care for patients.2 This educational environment must be aligned with a nonpunitive response to errors and continuous cultural improvement and organizational learning.3 Speaking up and flattening hierarchy in some urgent scenarios plays an important role in maintaining patient safety. This tutorial presents some definitions,techniques, strategies, and barriers for implementing speaking up in the OR.
DEFINITIONS
Psychological safety is a shared belief that anyone on the care team can speak up and share their opinion respectfully without fear of retribution. In this safe environment staff members should develop positive interpersonal relationships that are perceived as supportive and trusting, where it is okay to share ideas and voice potential concerns.2 Psychological safety empowers core team behaviours, like speaking up.2
Speaking up is explicitly communicating task-relevant observations, or requesting clarification of, or explicitly challenging or correcting, a task-relevant decision or procedure.4 This may be affected by power distance.
Power distance refers to inequity that may exist between ‘high-status’ and ‘low-status’ individuals that could influence team decisions, team cohesion, and dynamics.5
Speaking up is an important way to increase situational awareness, learn from each other, and provide constructive feedback amongst the OR team members.
TECHNIQUES
Several structured communications tools have been designed to reduce the probability of error when one team member recognizes a problem during teamwork. These tools are easy to remember and use incremental actions to challenge colleagues and reduce the potential for error.1

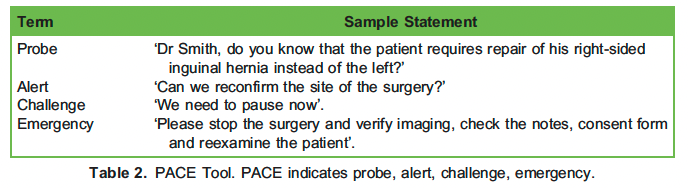
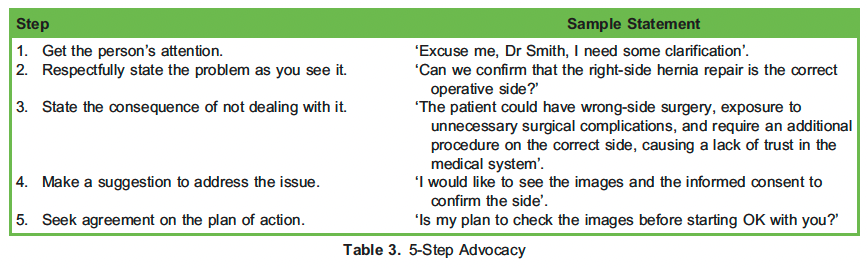
Examples of tools that may applied to express concerns within the team include the concerned–uncomfortable–scared (CUS) model, which was created by United Airlines for their crews; the probe–alert–challenge–emergency (PACE) model; and the 5-step advocacy and inclusive leadership concept.1 These tools are further explained in Tables 1, 2, and 3 using the following example.
Dr Smith is a general surgeon who has been working in an academic hospital for 15 years and is also the program director of the residency program. Dr Harvey is a first-year surgery resident who started his residency 3 months ago. Today is the first time that they are working together, and Dr Harvey is going to assist Dr Smith in the OR in a right open inguinal hernia repair with a mesh. After the induction of the anaesthesia, Dr Harvey noticed that the left side is marked for the operation.
If there is a failure to respond to the above-listed tools, the Agency for Healthcare Research and Quality6 suggests the ‘two- challenge rule’. When an initial assertive statement is ignored, a team member must raise the concern twice and be sure that it has been heard. Following this, if there is still a breach in safety, the team member must address the concern to someone in a leadership position or take another course of action.
Dr Smith replied to Dr Harvey, ‘I marked the side in front of the nurse and we both verified that the hernia is on the left side. I am going to go ahead with the surgery’. Dr Harvey raised his concern again to the whole team and this time he involved the senior surgery resident. Dr Harvey showed the images and notes to the senior resident and they both raised the concern together.
The example also demonstrated how hierarchy in the operating room could prevent or delay a team member from speaking up because of the status and power of senior clinicians. The first-year resident included the senior resident in raising their concern and reduced the power distance between them and the most senior clinician. A more experienced surgical resident raising or sharing the concern may penetrate the hierarchy more effectively in this example.
Leaders who explicitly invite others to share ideas or concerns, or use inclusive language such as ‘we’ (eg, ‘What are we missing?’), promote speaking up and create a psychologically safe environment.7 This is called inclusive leadership, and focuses on building relationships between team members to create a sense of identity where all members work together. It means a team member sharing crucial information about the patient that is missed by the leader can speak up freely and prevent errors.
IMPLEMENTATION STRATEGIES
Although several techniques have been described, an ideal teaching tool for speaking up has not been specifically developed.8 High-fidelity simulation interventions to teach conflict management skills at the undergraduate level, and interprofessional education events in conjunction with interactive presimulation activities, for example, video case studies or virtual games, could be used to practice implementing the tools.8,9 Other educational interventions, such as practicing being assertive, speaking-up rubrics, role-play exercises and debriefing, are not effective in isolation,8 and unless other measures are applied, such as institutional emphasis on speaking up even when uncertainty is present, behaviours are unlikely to change.10
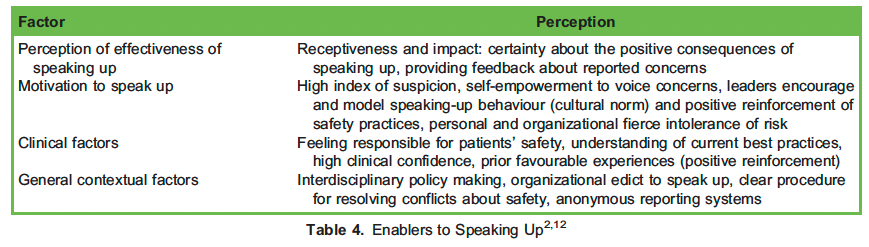
Organizational changes, like building a climate of respect, staff training in the models of speaking up, and/or an internal anonymous reporting system, will help to facilitate speaking up (Table 4).11
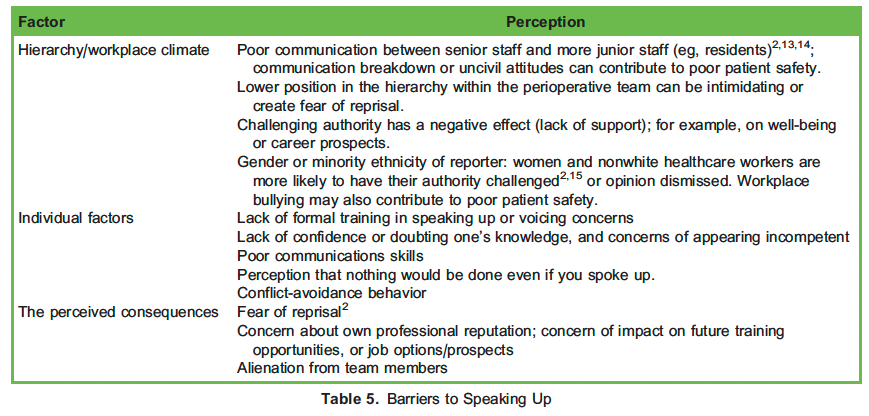
There are also many factors that can prevent people from speaking up. Cultural, professional, and organizational structures can create hurdles to speaking up; people avoid speaking up in hierarchical environments where raising concerns is perceived by team members to be disloyal, disobedient, or disrespectful.10 These factors create barriers to implementing a speaking-up culture, and are listed in Table 5.12
SUMMARY
Adopting a culture of safety around speaking up in the health care environment would promote psychological safety in the workplace, which is especially important when teams face difficult, often critical, situations. For this to happen, cultural, professional, and organizational barriers must be acknowledged and broken down. Furthermore, structured communication tools and anonymous reporting systems should be implemented, and interprofessional simulation of case scenarios should be undertaken regularly to learn skills in, and build confidence in, speaking up among team members.
REFERENCES
- Green B, Oeppen RS, Smith DW, et al. Challenging hierarchy in healthcare teams—ways to flatten gradients to improve teamwork and patient care. Br J Oral Maxillofac Surg. 2017;55(5):449-453.
- Canadian Medical Protective Team communication is critical to safe care. Accessed February 14, 2022. https://www.cmpa-acpm.ca/en/education-events/good-practices/physician-team/team-communication
- Amiri M, Khademian Z, Nikandish R. The effect of nurse empowerment educational program on patient safety culture: a randomized controlled trial. BMC Med Educ. 2018 Jul 3;18(1):158.
- Kolbe M, Burtscher MJ, Wacker J, et Speaking up is related to better team performance in simulated anesthesia inductions: an observational study. Anesth Analg. 2012;115:1099-1108.
- Appelbaum NP, Lockeman KS, Orr S, et Perceived influence of power distance, psychological safety, and team cohesion on team effectiveness. J Interprof Care. 2020;34(1):20-26.
- Agency for Healthcare Research and Quality. Pocket guide: TeamSTEPPS. Accessed February 14, 2022. https://www.gov/teamstepps/instructor/essentials/pocketguide.html#mutual
- Minehart RD, Foldy EG, Long JA, et Challenging gender stereotypes and advancing inclusive leadership in the operating theatre. Br J Anaesth. 2020;124(3):e148-e154.
- Daly Guris RJ, Duarte SS, Miller CR, Schiavi A, Toy S. Training novice anaesthesiology trainees to speak up for patient safety. Br J Anaesth. 2019;122:767-775.
- Oner C, Fisher N, Atallah F, et Simulation-based education to train learners to ‘‘speak up’’ in the clinical environment. Simul Healthc. 2018;13(6):404-412.
- Da Silva C, Peisachovich E, Anyinam CK, et al. Speaking up against hierarchy: a simulation geared towards nursing students. Cureus. 2020;12(12):e11977.
- Raemer DB, Kolbe M, Minehart RD, et al. Improving anesthesiologists’ ability to speak up in the operating room: a randomized controlled experiment of a simulation-based intervention and a qualitative analysis of hurdles and enablers. Acad Med. 2016;91(4):530-539.
- Institute for Safe Medical Speaking up about patient safety requires an observant questioner and a high index of suspicion. Accessed July 22, 2022. https://www.ismp.org/resources/speaking-about-patient-safety-requires-observant-ques tioner-and-high-index-suspicion#:~:text¼Specialty%20Pharmacy-,Speaking%20Up%20About%20Patient%20Safety%20 Requires%20an%20Observant,a%20High%20Index%20of%20Suspicion&text¼Healthcare%20practitioners%20are%20 expected%20to,and%20avoid%20adverse%20patient%20outcomes
- Beament T, Mercer SJ. Speak up! Barriers to challenging erroneous decisions of seniors in anaesthesia. Anaesthesia. 2016, 71, 1332-1340.
- Kobayashi H, Pian-Smith M, Sato M, et al. A cross-cultural survey of residents’ perceived barriers in questioning/ challenging authority. Qual Saf Health Care. 2006;15(4):277-283
- Pattni N, Arzola C, Malavade A, et Challenging authority and speaking up in the operating room environment: a narrative synthesis. Br J Anaesth. 2019;122(2):233-244.
- Pattni N, Bould MD, Hayter MA, et al. Gender, power and leadership: the effect of a superior’s gender on respiratory therapists’ ability to challenge leadership during a life-threatening emergency. Br J Anaesth. 2017;119(4):697-702.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/