General Topics

Before reading the tutorial, please answer the following questions. The answers are contained in the article.
- What are the advantages of a sub-Tenon’s block compared with a retrobulbar or peribulbar block?
- Which patients might be unsuitable for a sub-Tenons’s block?
- Briefly describe the important steps when performing a sub-Tenon’s block.
- Briefly Discuss the different types of anaesthetic mixture which may be used.
- What are the problems with performing a sub-Tenon’s block in a patient who:
- is highly myopic?
- has had previous scleral banding
- What are the complications of sub-Tenon’s anaesthesia and how are they managed?
Today an increasing number of ophthalmic surgical procedures are performed under local anaesthesia. Up until recently both peribulbar and retrobulbar blocks were the technique of choice, and in experienced hands would often produce excellent operating conditions in terms of both analgesia and akinesia. These techniques have, however, been associated with uncommon although potentially serious complications, including retrobulbar haemorrhage, globe perforation, optic nerve damage and inadvertent brainstem anaesthesia. The technique of sub-Tenon’s anaesthesia, using a blunt needle, provides a safe yet reliable alternative, and in the UK has rapidly become the procedure of choice for ophthalmic anaesthetists and surgeons alike. In 1992, Stevens described a single quadrant approach for administering local anaesthetic into the sub-Tenon’s space, and this technique will be described in more detail below.
Anatomy
Tenon’s capsule is a thin layer of connective tissue which surrounds the globe. Anteriorly it lies in close apposition to the conjunctiva and fuses with it at the level of the limbus. It extends posteriorly in all directions around the globe, ultimately fusing with the dura of the optic nerve. At intervals along its course it is pieced by the extra-ocular muscles as they insert into the globe.
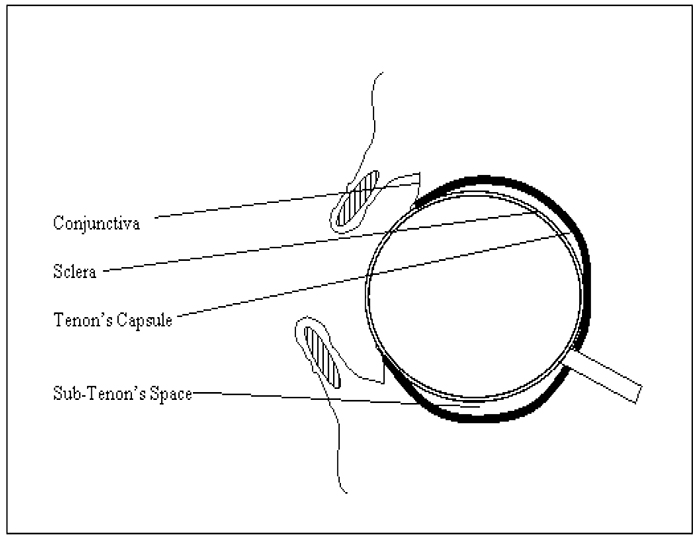
The Sub-Tenon’s space is a potential space between the capsule and the sclera. The instillation of local anaesthetic into this space produces analgesia and akinesia by diffusing posteriorly into the retro-orbital space to block the traversing sensory and motor nerves. There is probably also a direct effect on the sensory nerves within the sclera and the extra-ocular muscles as they breach Tenon’s capsule.
Performing the block
A patient’s suitability for a local anaesthetic technique will need to be established. Many patients undergoing ophthalmic procedures will be elderly and may have significant co-morbidities. As a result a local anaesthetic technique, although highly desirable might, in some circumstances, be wholly inappropriate. For example, patients who have a chronic cough, shortness of breath or severe gastro- intestinal reflux may find lying still for the duration of surgery an impossible task. In addition, patients who are unable to communicate through language difficulties or mental incapacity may also not be suitable. Patients who are very anxious will sometimes require a general anaesthetic, although the administration of careful sedation together with a sub-Tenon’s block might be an option.
Patient refusal or allergy to local anaesthetics would constitute an absolute contraindication. Patients taking anti-coagulant medication such as aspirin, clopidogril or warfarin can still safely receive a sub- Tenon’s block as the risk of significant or problematic bleeding is negligible. The question as to whether the surgical procedure should proceed or not in the face of abnormal clotting will depend on the nature of the surgery and the clinical judgment of the surgeon.
The patient should be placed in the supine position and standard monitoring applied (ECG, pulse oximetry and non-invasive blood pressure). Intravenous access is desirable but not essential. The decision to cannulate will need to take into account a number of factors, including the pre-morbid state of the patient, the need for sedation or iv fluids and the perceived risk of significant arrhythmias resulting from the oculo-cardiac reflex. The conjunctiva will first need to be anaesthetised with a topical anaesthetic solution such as proxymetacaine and amethocaine. The anesthetised conjunctiva should then be cleaned by carefully placing a few drops of povidone iodine beneath the lower eyelid. The rest of the orbital margin can then be cleaned with any remaining solution. An eyelid speculum is inserted to improve access and prevent blinking. Asking the patient to look up and out will assist in exposing the inferonasal quadrant. A well positioned mark or cross on the wall or ceiling will often help in maintaining this line of gaze. A small tent of conjunctiva (together with the underlying Tenon’s capsule) is raised with a pair of blunt, non-toothed forceps approximately 5-10 mm from the infero-nasal limbus (Figure 2). A small incision is made in the tissue using a pair of ophthalmic scissors, exposing the white “marble” like sclera below (Figure 3).

Figure 2
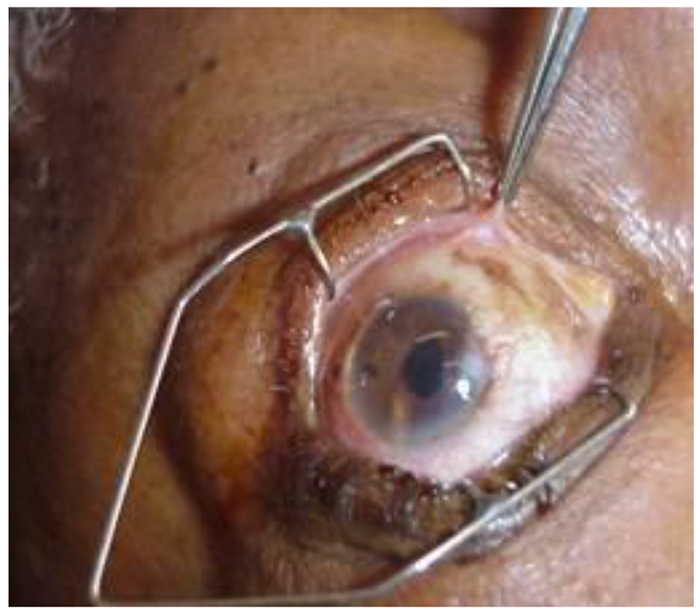
Figure 3
A failure to visualize the sclera often indicates that the Tenon’s capsule has not been breached. Attempting to inject local anaesthetic solution into this tissue plane will almost certainly result in gross conjunctival oedema (chemosis) and produce an inadequate block. In this circumstance a second attempt should be made at picking up the Tenon’s capsule and a further incision made. A blunt cannula (preferably curved – e.g. Stevens needle 19G, 25mm) can then be inserted, with the syringe of local anaesthetic attached, and passed posteriorly, following the curvature of the globe, until its tip is perceived to have passed the equator (Figure 4). If a curved needle is not available, other options include using a straight blunt needle or the plastic portion of an intravenous cannula (20 or 22G).

Figure 4

Figure 5
On injection of the local anaesthetic, little resistance is usually encountered and most of the solution should disappear behind the globe resulting in slight proptosis. If resistance is encountered, the needle can be withdrawn slightly and repositioned. On occasions, there may be a moderate amount of leakage back onto the surface of the eye and mild chemosis is not uncommon. After removal of the cannula, gentle pressure applied to the globe for about one minute may assist in the spread of the local anaesthetic (Figure 5). The onset of analgesia is usually rapid, whereas maximal akinesia may take up to 10 minutes to develop. Should the block not appear to be adequate after 5 minutes, as indicated by the absence of a developing akinesia, a further top up can be given through the pre-existing incision.
Extra caution is required in patients who have extreme myopia (axial length >25mm) as they have thinner and longer globes which are at an increased risk of perforation. Patients who have had previous surgery, notable scleral banding, are frequently difficult in terms of accessing the sub-Tenon’s space. In these patients a peribulbar block or general anaesthetic may be required.
Local anaesthetic mixture
Numerous local anesthetic solutions have been used with varying degrees of efficacy and duration. In the UK, most anaesthetists use a combination of lidocaine (2%) and bupivacaine (0.5%) often in equal proportion, with or without the addition of hyaluronidase (30 – 150 iu/ml). A local anaesthetic mixture volume of 3-5 mls is often sufficient to produce a good quality block, with a duration of surgical anaesthesia exceeding one hour. For surgery of short duration, such as cataract extraction, lidocaine alone may be used. The addition of hyaluronidase is not essential, but is well recognized to increase the spread of local anaesthetic in the retro-orbital compartment. It is, however, expensive and has been associated with severe side effects such as anaphylaxis and sterile abscess formation. An alternative to the lidocaine-bupivacaine mixture is articaine (2%) which has been widely used in dental anaesthesia. Articaine has the advantage of increased tissue perfusion, thus obviating the need for hyaluronidase. It also has a low systemic toxicity.
Complications of sub-Tenon’s Anaesthesia
The sub-Tenon’s block is perceived as a safe alternative to both the retrobulbar and peribulbar blocks, both of which require the use of a sharp needle. The risk of a dural puncture with subsequent brainstem anaesthesia, globe puncture and inadvertent intravascular injection is rare. The main complications seen with this technique is subconjunctival swelling (40%) and subconjunctival haemorrhage (50%), both of which will usually resolve with gentle orbital pressure.
Summary
Sub-Tenon’s anaesthesia has become widely practiced throughout the UK. It is a very safe and reliable block and is very well tolerated by patients. It can provide adequate anaesthesia for a number of ophthalmic procedures ranging from cataract surgery to vitreoretinal surgery. The sensory component of the block is often very effective, however, total akinesia may not always be obtained. Significant complications are rare, but many patients will experience a degree of conjunctival swelling and heamorrhage.
Acknowledgements
I would like to thank Dr Andrew Presland (Consultant Anaesthetist at Moorfields Eye Hospital, London) for allowing me to use his photographs.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/