Basic Sciences

KEY POINTS
- Trifascicular block is a type of heart block in which the problem is with infranodal impulse conduction to the ventricles.
- Trifascicular block is an important diagnosis because it can progress to complete heart block.
- It may be asymptomatic or present with symptoms of presyncope or syncope
- It can be easily missed on single-surface electrocardiography recording.
- High doses of atrioventricular nodal blocking agents should be avoided in patients with trifascicular block.
- Anaesthesia should be carefully planned in patients with trifascicular block to avoid increase in vagal tone, which can potentially lead to precipitation of complete heart block, arrhythmias or myocardial infarction.
INTRODUCTION
Trifascicular block is a condition that affects cardiac electrical impulse conduction in the 3 fascicles that carry electrical signals from the atrioventricular node (AVN) to the ventricles. The infranodal fascicles are the right bundle branch (RBB) and the left bundle branch (LBB). The LBB is further divided into the left anterior fascicle (LAF) and the left posterior fascicle (LPF). Electrocardiographic abnormalities can be caused by ‘block’ at any of these levels.1
Trifascicular block is a precursor to complete heart block. Complete heart block complicating acute myocardial infarction (MI), in a patient with trifascicular block, is associated with high mortality from arrhythmia and pump failure.
ANATOMY OF THE CONDUCTION SYSTEM
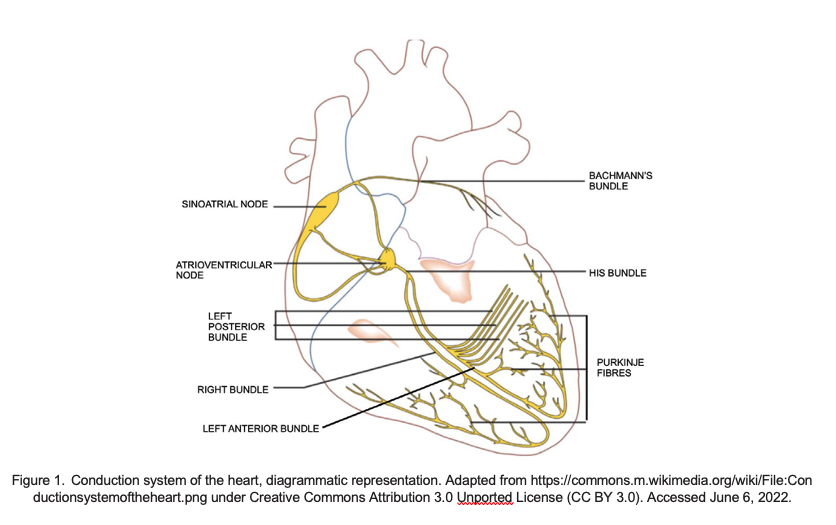
Under normal conditions, electrical signals in the heart are generated spontaneously by the sinoatrial node (the cardiac pacemaker, located in theright atrium) and propagated throughout the right and left atria stimulating the atrial myocardium to contract (seen on electrocardiography [ECG] as the P wave) (Figure 1). The electrical activity travels to the AVN located in the interatrial septum via specialised pathways known as internodaltracts. The AVN is a site of critical delay in impulse conduction from atria to ventricles, which ensures that by not contracting together, effectiveblood flow is maintained from atria to ventricles (seen on ECG as the PR segment).
From the AVN the impulses are conducted via the bundle of His and the left and right bundle branches in the interventricular septum. The LBB further divides into anterior and posterior fascicles. The LPF is shorter and broader and conducts impulses to the posterior and inferior part of theleft ventricle. It has dual blood supply so isolated block of the LPF is rare. The LAF covers the upper and anterior part of the left ventricle. Block of the LAF causes left-axis deviation on ECG.
Electrical impulses are then conducted via Purkinje fibres, which stimulate the ventricles to contract. Ventricular contraction begins at the apex ofthe heart and progresses upwards, ensuring that contraction is more efficient in squeezing blood towards the exit. The rhythmic nature of these signals results in the coordinated contraction and relaxation of the heart.2
TRIFASCICULAR BLOCK
Definition
Trifascicular block is a conduction delay below the AVN in which all 3 fascicles that carry signals from the AVN to the ventricles (ie, RBB, LAF andLPF) are involved. If simultaneous complete block of all 3 fascicles is present, then it is referred to as third- degree (complete) heart block.
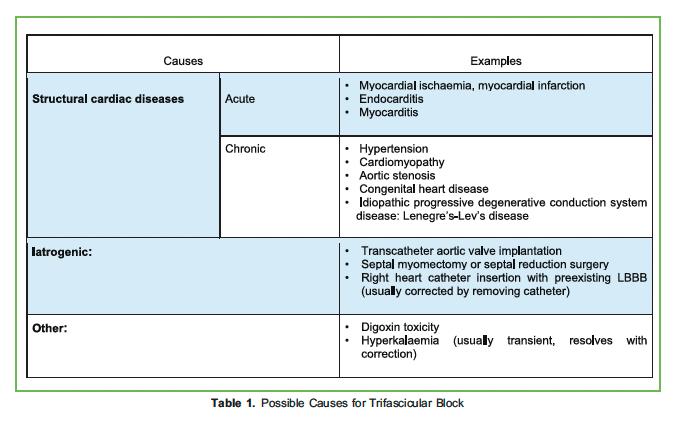
Trifascicular block can manifest as alternating RBB block (RBBB) and LBB block (LBBB), or RBBB with alternating LAF block or LPF block on a beat-to-beat basis. This is an indicator of conduction disturbance existing in all 3 bundles.
Aetiology
Causes of trifascicular block include structural cardiac diseases, iatrogenic causes, dyselectrolytaemia or drug effects.3 Table 1 lists some examples.
Diagnosis
Trifascicular block can be asymptomatic or it can present with symptoms such as tiredness, light-headedness, fainting, shortness of breath orchest pain. Therefore, a detailed history and examination are important and a baseline ECG is prudent. These symptoms may point towards underlying structural heart disease, cardiac dyssynchrony from LBBB or intermittent bradycardia. Ambulatory ECG monitoring is helpful for symptom-rhythm correlation and the choice of rhythm monitor is often dictated by frequency of symptoms. In the presence of symptoms suggestive of conduction disorders with other signs or symptoms of cardiovascular disease, it would be appropriate to assess for any structural heart disease by echocardiography.
Electrophysiological studies (EPS) may be considered in selected patients for diagnosis and elucidation of bradycardia mechanism if initial noninvasive evaluation is nondiagnostic. A definitive diagnosis of trifascicular block can be made by His bundle electrogram (HBE) recording via cardiac EPS.
Commonly used ECG diagnostic criteria for identifying trifascicular block include the following:
- Alternating bundle branch LBBB and RBBB are present in one patient, either on separate ECGs or alternating on the same ECG4 (Figure 2).5
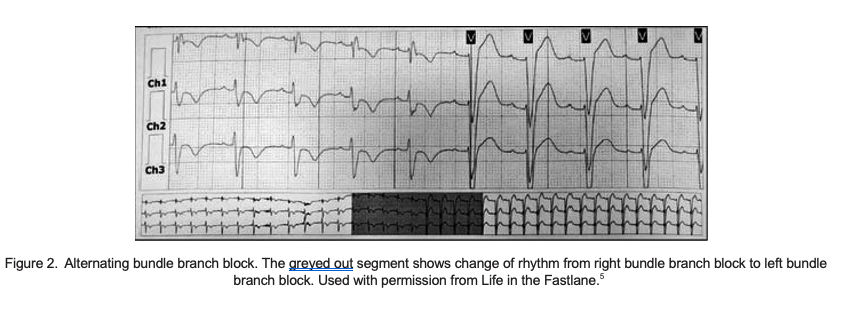
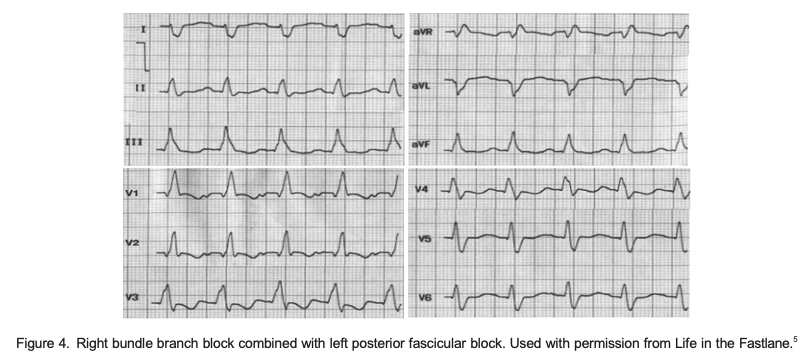
- Permanent block in 1 fascicle and intermittent block in the other For example, a patient with chronic RBBB has a pattern of LAF block and LPF block on different occasions; that is, RBBB with alternating fascicular block (Figures 3 and 4).
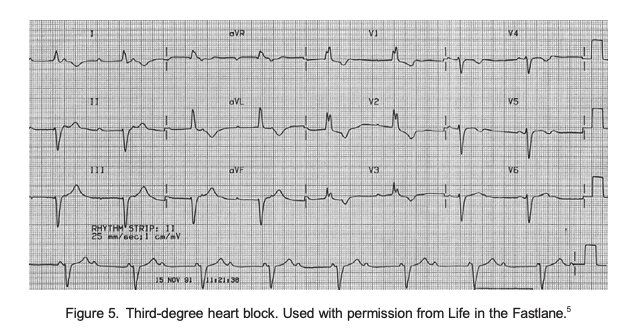
- Complete trifascicular block (complete heart block). All 3 fascicles (RBBB, LAF and LPF) are blocked There is complete dissociation of P waves and QRS complexes (Figure 5).
Difference With a Bifascicular Block
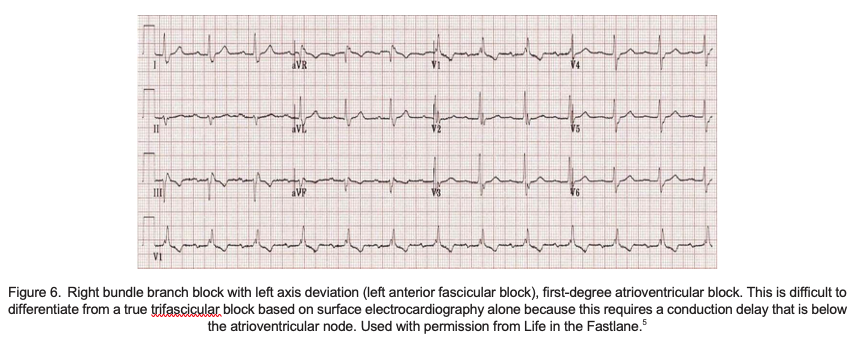
Bifascicular block (RBBB and LAF block or LPF block) with first-degree atrioventricular (AV) block is often referred to as ‘trifascicular block’; however, this is a clinical misnomer because the conduction delay accounting for the long PR interval is usually found at the level of the AVN, notinfranodally.1 A true trifascicular block is where the conduction delay is below the AV node (see Figure 6).
Bifascicular block with AV block can be differentiated from trifascicular block by identifying the site of the block. Intravenous atropine injection orexercise testing is used to facilitate AVN conduction. If the AV block resolves, then the location of block is in the AVN, but if the increase in sinus rate is associated with more advanced degrees of AV block, the location of the block is likely infranodal.1 EPS will be helpful in demonstrating conduction delays in remaining fascicles below the bundle of His.
EPS Analysis
EPS permits a detailed analysis of the site of conduction delay and the mechanism underlying the cardiac arrhythmia. Baseline recordings during typical invasive EPS include several surface and intracardiac electrograms recorded simultaneously. HBE is obtained from a catheter positioned atthe bundle of His and the AVN-His interval, HBE duration and His-ventricle (HV) interval measured from HBE can help in identifying precise location of block.6
- AVN-His This reflects conduction from the low right atrial inputs into the AVN, the AVN proper and the proximal His bundle.
- HBE This reflects conduction through the short length of compact His bundle that penetrates the fibrous septum.
- HV This reflects conduction time through the distal His-Purkinje system. Unlike the AVN, the His-Purkinje system is far less influenced by the autonomic nervous system, and the normal range of the HV interval is narrow (35 to 55 ms). A prolonged HV interval is consistent with diseased distal conduction in all fascicles.
PREOPERATIVE CONSIDERATIONS
Evaluation
The preanaesthetic evaluation should include a thorough review of medical history and an examination, looking for signs and symptoms such as tiredness, light-headedness, fainting, chest pain or shortness of breath.
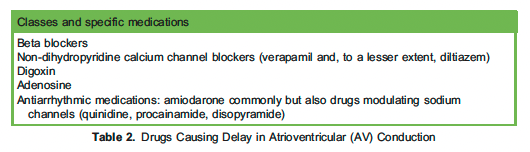
Drug history is important because a variety of drugs can impair AV conduction resulting in an AV block (Table 2). An AV block in patients with preexisting trifascicular block is likely to increase the risk of complete heart block. An individual risk-benefit analysis should be undertaken in consultation with a cardiologist so that a decision can be made to continue or withhold a particular drug that might be contributory to the conduction delay.
A 12-lead ECG is indicated to establish a baseline. Ambulatory ECG monitoring helps establish symptom-rhythm correlation and helps document a previously unknown conduction block. Transthoracic echocardiography can help exclude structural heart disease.
Metabolic and electrolyte homeostasis should be checked and corrected preoperatively, especially in emergency surgery because hyperkalaemia could be a potentially reversible cause of new-onset trifascicular block.
The American College of Cardiology (ACC), American Heart Association (AHA) and Heart Rhythm Society (HRS) recommend that EPS is reasonable for evaluation of conduction disorders. It is particularly important for patients with symptoms suggestive of intermittent bradycardiawith conduction system disease identified by ECG and no demonstrated AV block.
For elective surgery, cardiology consultation is sought to establish cause, assess cardiac function, optimise medications and evaluate suitability for permanent pacemaker (PPM) implantation. There are 2 factors that guide the majority of decisions regarding PPM insertion:
- Association of symptoms with an arrhythmia
- Potential for progression of the rhythm disturbance, which is largely dependent on anatomical location of conduction abnormality. Disease below the AV node, in the His-Purkinje system, is generally considered less stable, so PPM is more likely to be recommended.
Role of Preoperative Cardiac Pacing
The ACC/AHA/HRS 2018 recommendations3 for management of conduction disorders state the following:
- Pacing is indicated in patients with alternating bundle branch block (class 1 recommendation).
- Pacing is indicated in patients with syncope, bundle branch block and HV interval 2:70 ms, or evidence of infranodal block at EPS (class 1 recommendation).
- In patients with acquired second-degree Mobitz type II AV block or third-degree AV block (high-degree heart block) not caused by reversible or physiologic causes, permanent pacing is recommended regardless of symptoms.
INTRAOPERATIVE
Intraoperative vigilance and monitoring is essential due to potential metabolic disturbances, fluid shifts, haemodynamic instability and the use of drugs that can cause myocardial depression and bradycardia. All these factors can have a negative effect on cardiac function. Presence of trifascicular block indicates higher likelihood of significant conduction system disease, which may progress to haemodynamically unstable heart block intraoperatively.
Preparation
- Standard monitoring comprising noninvasive arterial blood pressure, heart rate, continuous ECG (consider 5-lead ECG), pulse oximetry, end-tidal carbon dioxide and body temperature should be established. Need for invasive monitoring should be dictated by patient profile and type of procedure.
- Atropine, beta-adrenergic agonists and intravenous aminophylline should be available prior to induction of anaesthesia.
- Temporary pacemaker equipment (eg, pulse generator, pacing leads, connecting cables) must be readily available. The general availability of transcutaneous pacing has made it an acceptable alternative to temporary transvenous pacing in emergency situations, although poor myocardial capture from transcutaneous leads and patient discomfort necessitating sedation are limitations that should be considered.
Acute Medical Therapy for Bradycardia
After ensuring adequacy of airway, breathing and depth of anaesthesia and removal of possible surgical stimulus (if thought to be a cause of bradycardia), the options for medical management would include the following:
- Atropine (1-mg IV increments up to 3 mg) is usually effective for bradycardia due to excess vagal tone and block at the AVN level. Occasionalreports of worsening block in patients with a block at the His bundle or His-Purkinje level warrants judicious use of atropine in such patients.
- Beta-adrenergic agonists (isoproterenol, dopamine, dobutamine and epinephrine) enhance AVN and His-Purkinje conduction by direct effect and may enhance automaticity of subsidiary ventricular pacemakers in the setting of complete AV block. Adverse effects may include elicitation of ventricular arrhythmias and induction of coronary ischemia.7
- Aminophylline may be considered in atropine-resistant bradycardia in the setting of acute MI because it improves AV conduction, increases ventricular rate and may improve symptoms.3
Important Points
- LBBB, RBBB or fascicular block can occur during anaesthesia. New onset of such blocks usually indicates either intrinsic cardiac disease ormyocardial ischaemia, which should be rapidly Chronic and new conduction abnormality both predict worse outcome but for different reasons. The former suggests more extensive underlying cardiac disease and the latter suggests a larger ischaemic area.
- In patients who have recurrent or severe bradycardia with hemodynamic instability, temporary pacing may be necessary.
- Management and prognosis of high-degree heart block secondary to acute MI differs depending on infarct location. High- degree heart block with anterior MI is more often located distal to the AVN. It is more symptomatic and associated with greater mortality due to greater loss offunctioning myocardium compared with high-degree heart block with inferior MI, which includes the AVN in 90% of patients.8
- Certain perioperative variables increase the likelihood of bradycardia, higher degree heart block and progression of trifascicular to complete heart block due to negative chronotropy or increased vagal tone. Anaesthesia should be carefully titrated to avoid or treat these factors, which include the following:
- Hypoxaemia, hypocapnia, hypercapnia, metabolic and electrolyte disturbances.
- Certain drugs used during general anaesthesia such as propofol, suxamethonium, opioids and
- Vagal response to laryngoscopy and intubation.
- Noncardiac surgical procedures that could activate the vagus nerve; for example, carotid endarterectomy or stenting, peritonealinsufflation during abdominal laparoscopy, eye surgery, cervical or anal dilatation and electroconvulsive therapy.9
- Trifascicular block in the setting of acute MI necessitates immediate pacing and prompt If the trifascicular block persists following revascularization, patients should receive PPM.10
Procedure-Specific Special Considerations
- In the setting of noncardiac surgery, intraoperative bradycardia is commonly due to excess vagal tone and is atropine responsive. It is rarely due to worsening AV conduction, therefore prophylactic transvenous pacing is not recommended.
- Although complete heart block can occur on pulmonary artery catheter insertion in patients with LBBB, the incidence is low, and severalstudies have reported increased risk of ventricular arrhythmias with temporary pacing, so it is not recommended prophylactically.11Nevertheless, clinicians should be prepared to manage this complication with rapid initiation of transvenous or immediate transcutaneous pacing.
- Risk of bradycardia post–cardiac surgery including site of conduction delay is largely related to type of cardiac surgery and anatomic relationto conduction Epicardial pacing wires are routinely placed if patient or procedure is deemed at high risk for conduction disturbances. PPM implantation before discharge is recommended if symptoms or instability do not resolve.
POSTOPERATIVE
All standard monitoring should continue in the postoperative period and the patient should be monitored in a high-dependency setting. Standard postoperative care should include adequate analgesia, maintaining normothermia and control of postoperative nausea and vomiting.
SUMMARY
Trifascicular block is a lesser known but not uncommon phenomenon. If the block is detected during preoperative evaluation, then multidisciplinary consultation should be sought and should include cardiology. These patients require evaluation and consideration for a pacemaker insertion due to the unstable nature of the block and the potential risk of deterioration to complete heart block, especially under general anaesthesia.
REFERENCES
- Olshansky B, Chung MK, Pogwizd SM, Goldschlager N. Arrhythmia Essentials. 2nd ed. Elsevier; 2017 (printed in United States of America).
- Hall JE, Hall Guyton and Hall Textbook of Medical Physiology. 14th ed. Elsevier; 2021 (printed in Canada).
- Kusumoto FM, Schoenfeld MH, Barett C, et al. 2018 ACC/AHA/HRS Guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Rhythm Society. Circulation. 2019;140(8):e382-e482.
- Gregoratos Indications and recommendations for pacemaker therapy. Am Fam Physician. 2005;71(8):1563-1570.
- Life in the ECG library. Accessed January 10, 2022. https://litfl.com/ecg-library/
- Majeed H, Sattar Y. Electrophysiologic study indications and evaluation. Accessed January 11, 2022. https://www.ncbi. nih.gov/books/NBK567719/
- Sidhu S, Marine Evaluating and managing bradycardia. Trends Cardiovasc Med. 2020 Jul;30(5):265-272.
- Brown Cardiac Intensive Care. 3rd ed. Elsevier; 2019:176-177 (printed in China).
- Maddali Cardiac pacing in left bundle branch/bifascicular block patients. Ann Card Anaesth. 2010 Jan-Apr;13(1):7-15.
- Epstein AE, DiMarco JP, Ellenbogen KA, et al. 2012 ACCF/AHA/HRS focused update incorporated into the ACCF/AHA/ HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology Foundation/AmericanHeart Association task force on practice guidelines and the Heart Rhythm J Am Coll Cardiol. 2013;61(3):e6-e75.
- Morris D, Mulvihill Risk of developing complete heart block during bedside pulmonary artery catheterization in patients with left bundle-branch block. Arch Intern Med. 1987;147(11):2005-2010.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/