Basic Sciences

The Autonomic Nervous System
Part II – Basic Pharmacology
In the first of our autonomic nervous system tutorials, we saw that:
- The autonomic nervous system (ANS) reflexes are instrumental in the control of most of the body’s organ systems
- The afferent limb of these reflexes can be from the ANS or central nervous system (CNS). The efferent limb is mediated by the sympathetic (SNS) or parasympathetic (PNS) divisions, which are functionally and structurally distinct.
- The observed physiological effect will depend upon which neurotransmitter and types of receptors are involved.
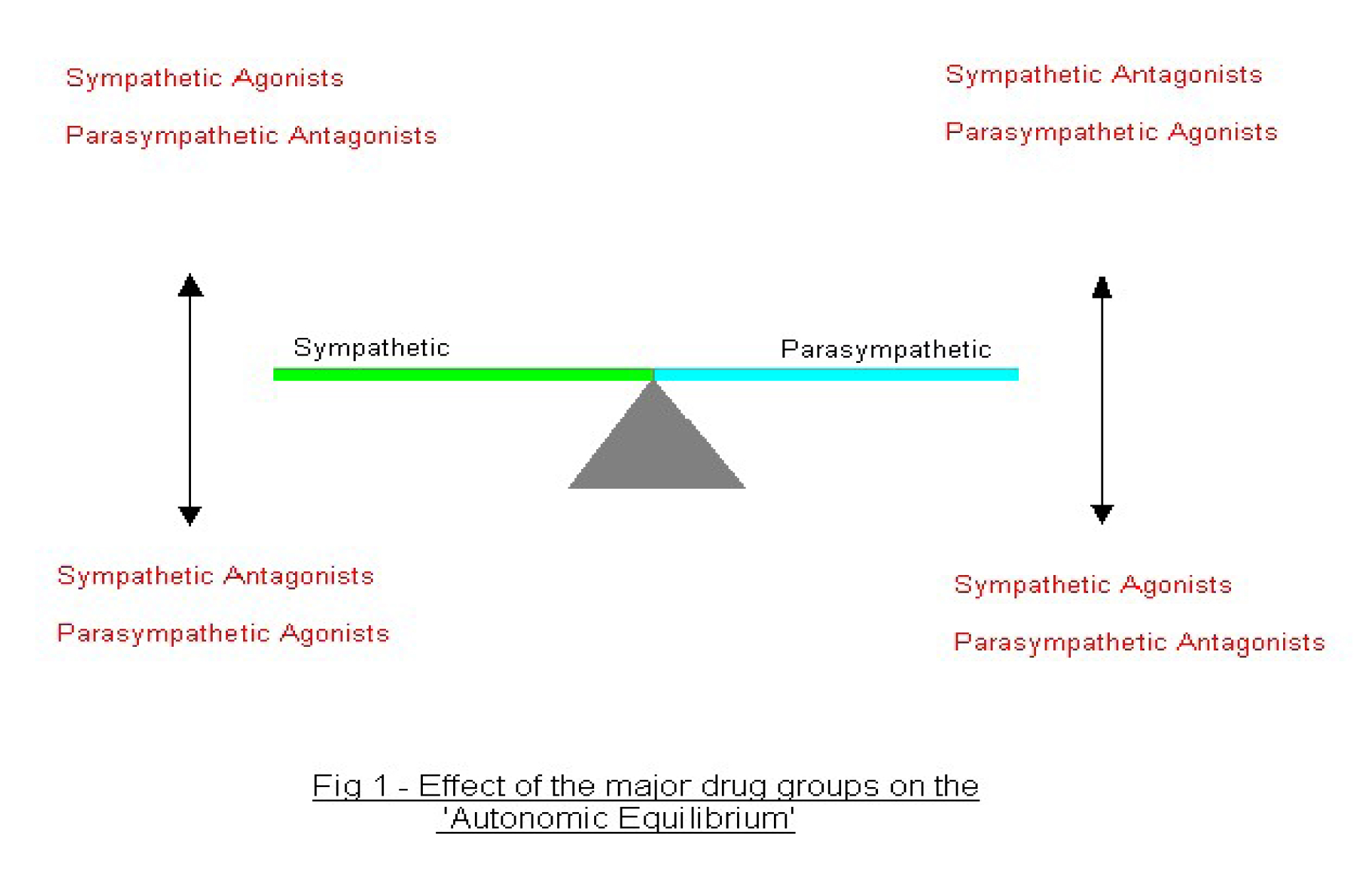
In the normal, resting situation equilibrium exists between sympathetic and parasympathetic activity. Drugs that stimulate or inhibit activity of either the parasympathetic or sympathetic division affect this balance.
Terminology
Some common terminology is used to describe the action of drugs on the autonomic nervous system.
Sympathomimetics are drugs with similar actions to the postganglionic fibres of the SNS. They resemble adrenaline (epinephrine) in their actions and are also referred to as adrenergics. (Sometimes called sympathetic agonists).
Sympatholytics are drugs that oppose the actions of the postganglionic fibres of the SNS. They are also referred to as antiadrenergics or sympathetic (adrenergic) antagonists. Both groups are subdivided further depending on their actions on either alpha or beta- receptors.
Parasympathomimetics are drugs that stimulate postsynaptic muscarinic receptors. Their actions resemble acetylcholine and they are also referred to as cholinergics or parasympathetic agonists.
Parasympatholytics are drugs that oppose the actions of the PNS at the muscarinic receptors by blocking the actions of acetylcholine. They are also referred to as anticholinergics, parasympathetic antagonists or occasionally vagolytics.
The autonomic effects of a drug may be the primary intended action – for example the sympathomimetic actions of dobutamine or secondary effects – for example the parasympathomimetic action of repeated doses of succinylcholine.
In the remainder of this tutorial, we will give an overview of the major groups of drugs that act on the autonomic nervous system and examine a few “special cases” – drugs that are commonly used in anaesthetic practice.
Pharmacology of the Sympathetic Nervous System
In our first tutorial, we saw that most of the effects of the sympathetic nervous system are mediated by catecholamines (most commonly noradrenaline) acting at alpha or beta- adrenoreceptors. All adrenoreceptors are similar in structure and belong to the family of G-protein-coupled receptors.
- Alpha-1 receptors activate phospholipase C and have their actions mainly by increasing release of intracellular calcium.
- Alpha-2 receptors inhibit adenylate cyclase, reducing cAMP formation.
- Beta-1 and -2 receptors stimulate adenylate cyclase, increasing cAMP formation.
The main actions of these receptors includes:
- Alpha-1: vasoconstriction, gut smooth muscle relaxation, salivary secretion, glycogenolysis in the liver, contraction of gut sphincters and uterus.
- Alpha-2: vasodilatation (central), vasoconstriction (peripheral), gut smooth muscle relaxation.
- Beta-1: positive inotropy and chronotropy.
- Beta-2: vasodilatation in muscle, gut and kidneys, bronchodilatation, pupillary dilatation, glycogenolysis.
Drugs with agonist or antagonist effects at both types of adrenoreceptor are commonly encountered in anaesthetic practice, and the most important are discussed below.
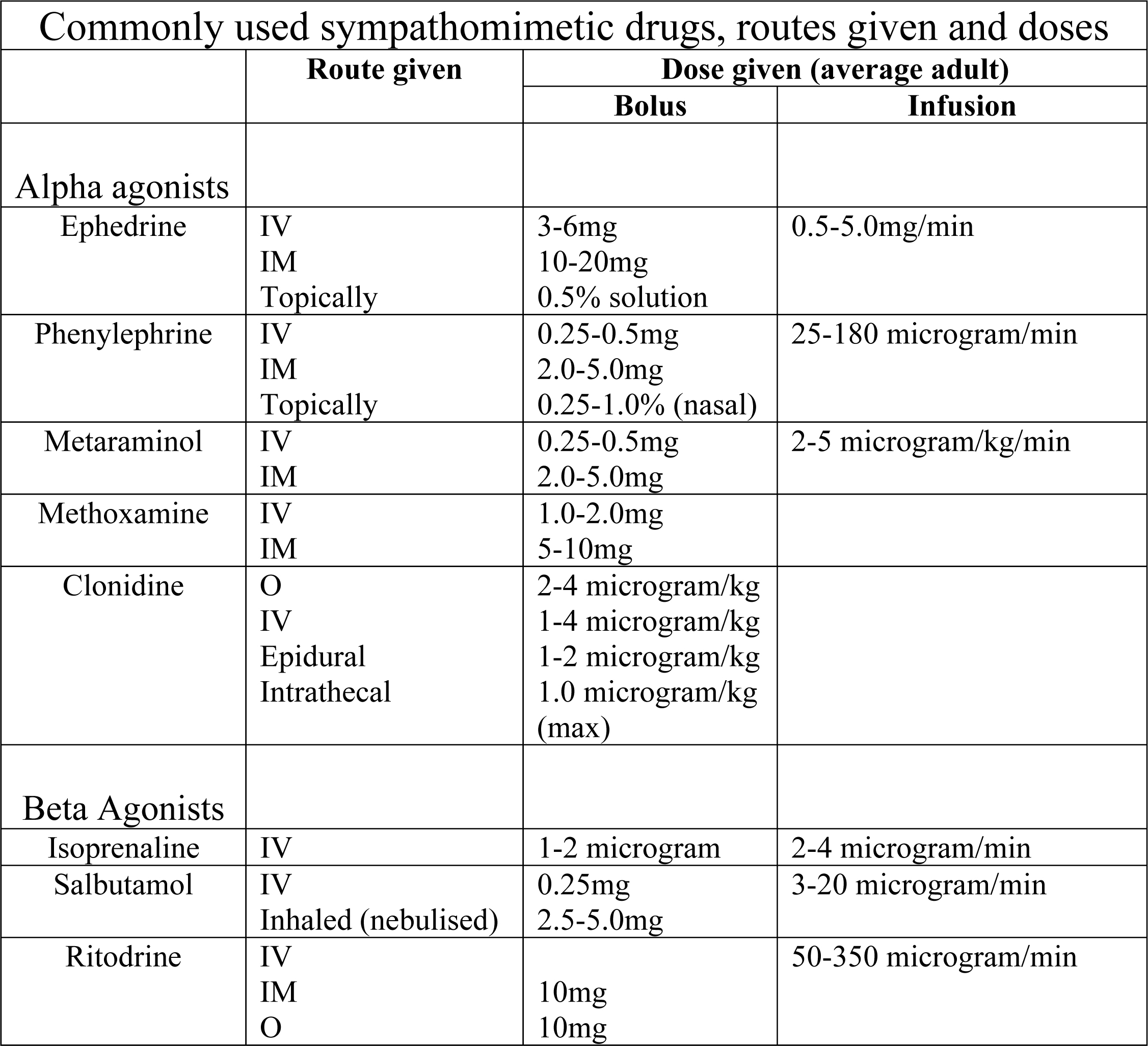
Sympathomimetics
These drugs can be classified or grouped in a number of different ways, but perhaps the easiest is to classify them according to their actions on adrenoreceptors. They either work by directly stimulating alpha and/or beta-receptors, or indirectly by stimulating the release of noradrenaline (norepinephrine) by acting presynaptically. A further class of drugs, the phosphodiesterase inhibitors have a postsynaptic action.
Alpha-1 receptor agonists
Ephedrine: an indirectly acting sympathomimetic. It is taken up into presynaptic nerve terminals, thereby displacing noradrenaline resulting in alpha mediated vasoconstriction. Ephedrine also has a direct beta agonist effect increasing heart rate and cardiac output, the overall effect increasing blood pressure. These actions last for 10-15 minutes and repeated doses have a gradually decreasing effect (tachyphylaxis). Commonly used to treat the hypotension associated with subarachnoid (spinal) block.
Amphetamine: causes CNS stimulation by releasing and blocking uptake of neurotransmitters. Also has peripheral indirect sympathomimetic activity causing acute rises in blood pressure. Currently, minimal therapeutic uses but derivatives of amphetamines are used as recreational drugs, for example ecstasy.
Phenylephrine acts directly almost totally on alpha-1 receptors causing vasoconstriction and increasing blood pressure, coronary and cerebral perfusion pressure. Heart rate usually slows due to reflex bradycardia. Cerebral and coronary blood flow is minimally affected. Used to treat hypotension associated with spinal and epidural anaesthesia and topically to provide vasoconstriction in the eye or nose before surgery. Large topical doses have been reported to cause significant CVS side effects including cardiac arrest.
Metaraminol: predominantly a direct alpha agonist causing peripheral vasoconstriction. Also has indirect sympathomimetic actions caused by the release of noradrenaline and adrenaline. When used in the treatment of acute hypotension, a baroreceptor mediated bradycardia is frequently seen.
Methoxamine: pharmacologically similar to phenylephrine, but much longer acting. Large doses may have a beta antagonist effect causing a bradycardia.
Xylometazoline, oxymetazoline: topically active vasoconstrictors used on mucous membranes, with low systemic absorption.
Alpha-2 receptor agonists
Alpha-2 receptors are found in the presynaptic membranes of adrenergic synapses and are widely distributed throughout the body including the CNS. They can be subdivided into three subtypes; alpha 2A (sedation, analgesia and sympatholysis), alpha 2B (vasoconstriction) and alpha 2C (CNS actions). Despite being agonists, their actions are generally more like sympatholytic drugs, but they are included here on the basis of their receptor activity.
Clonidine: a potent alpha-2 adrenergic agonist acting on the receptors in the spinal cord. When given orally or iv results in dose dependent sedation, reduces the dose of induction drug needed, reduces the MAC of volatile anaesthetics and provides a degree of analgesia. It increases haemodynamic stability during surgery, at recovery from anaesthesia and may reduce cardiac morbidity in high-risk cases. It reduces shivering and oxygen consumption at recovery.
When given epidurally, clonidine increases the quality and duration of block and provides a degree of postoperative analgesia. This practice has proved particularly popular in caudal epidurals in children. When used with local anaesthetics in spinals, it increases the duration and quality of block, but may increase the degree of hypotension. The need for a urinary catheter is reduced when compared to the use of intrathecal opioids. Clonidine has been used in critical care for sedation, analgesia for invasive procedures and to assist in reducing drug withdrawal symptoms after prolonged sedation.
Dexmedetomidine: has an even greater affinity for alpha-2 receptors than clonidine. Many effects are similar to clonidine but there is less clinical experience.
Beta receptor agonists
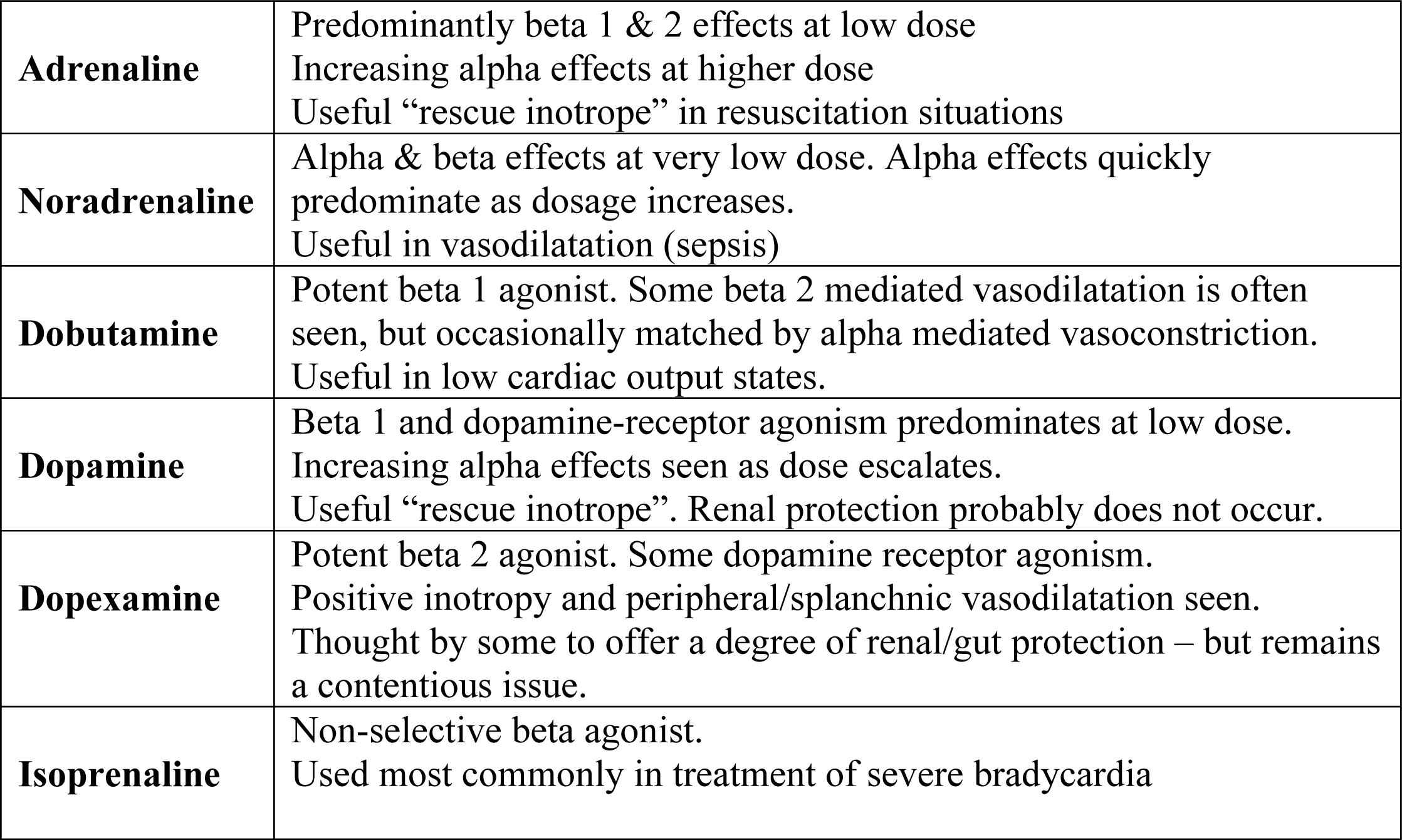
The main drugs in this group are the naturally occurring catecholamines, adrenaline (epinephrine) and noradrenaline (norepinephrine). Adrenaline is an agonist at alpha and beta receptors, noradrenaline has predominantly alpha agonist actions with minor beta-1 agonist activity. They will not be considered further here, but details of some of the catecholamines can be seen in appendix 1.
Isoprenaline: the first synthetic beta receptor agonist for clinical use, stimulating both beta-1 and -2 receptors. Usually given as an infusion because of its short duration of action. Used mainly to treat bradyarrhythmias and as a bronchodilator. Now largely replaced as a bronchodilator by beta-2 selective drugs because of the risk of cardiac arrhythmias.
Salbutamol: predominantly a beta-2 agonist used in the treatment of asthma, both intravenously and by inhalation. Also slows peristalsis and causes muscle tremor in large doses. Alternatives include terbutaline, and salmeterol and formoterol that are longer lasting.
Ritodrine: a beta-2 agonist used as a uterine relaxant (tocolytic) to prevent premature labour. Given i.v. initially followed by oral maintenance therapy. Salbutamol is also used for the same effect.
Phosphodiesterase Inhibitors
Phosphodiesterase is the enzyme responsible for breakdown of the cAMP produced by beta receptor activation. Inhibition of phosphodiesterase leads to accumulation of cAMP, which acts to amplify a beta-mediated sympathetic nervous system response. Various subtypes of phosphodiesterase are predominant in different cells and tissues and a number of different drugs exist which will predominantly inhibit the various subtypes. Whilst a full description is beyond the scope of this tutorial, 2 of the most common drugs are mentioned below.
Theophylline/aminophylline: Theophylline is a methylxanthine derivative, which is a non-specific inhibitor of all the phosphodiesterase subtypes. Aminophylline is a mixture of theophylline and ethylenediamine, which improves solubility and hence allows intravenous administration. These drugs are predominantly used as bronchodilators, but other actions include weak positive inotropy, peripheral and coronary vasodilation, and a degree of CNS stimulation. Theophyllines have a narrow therapeutic index, and dosage must be guided by monitoring of serum levels.
Enoximone: a selective inhibitor of phopshodiesterase subtype III, enoximone is a potent inotrope, which also causes marked peripheral vasodilation. It is particularly effective in patients with a high background sympathetic tone, such as that seen in heart failure. Extensive first-pass metabolism means enoximone is only effective when given intravenously.
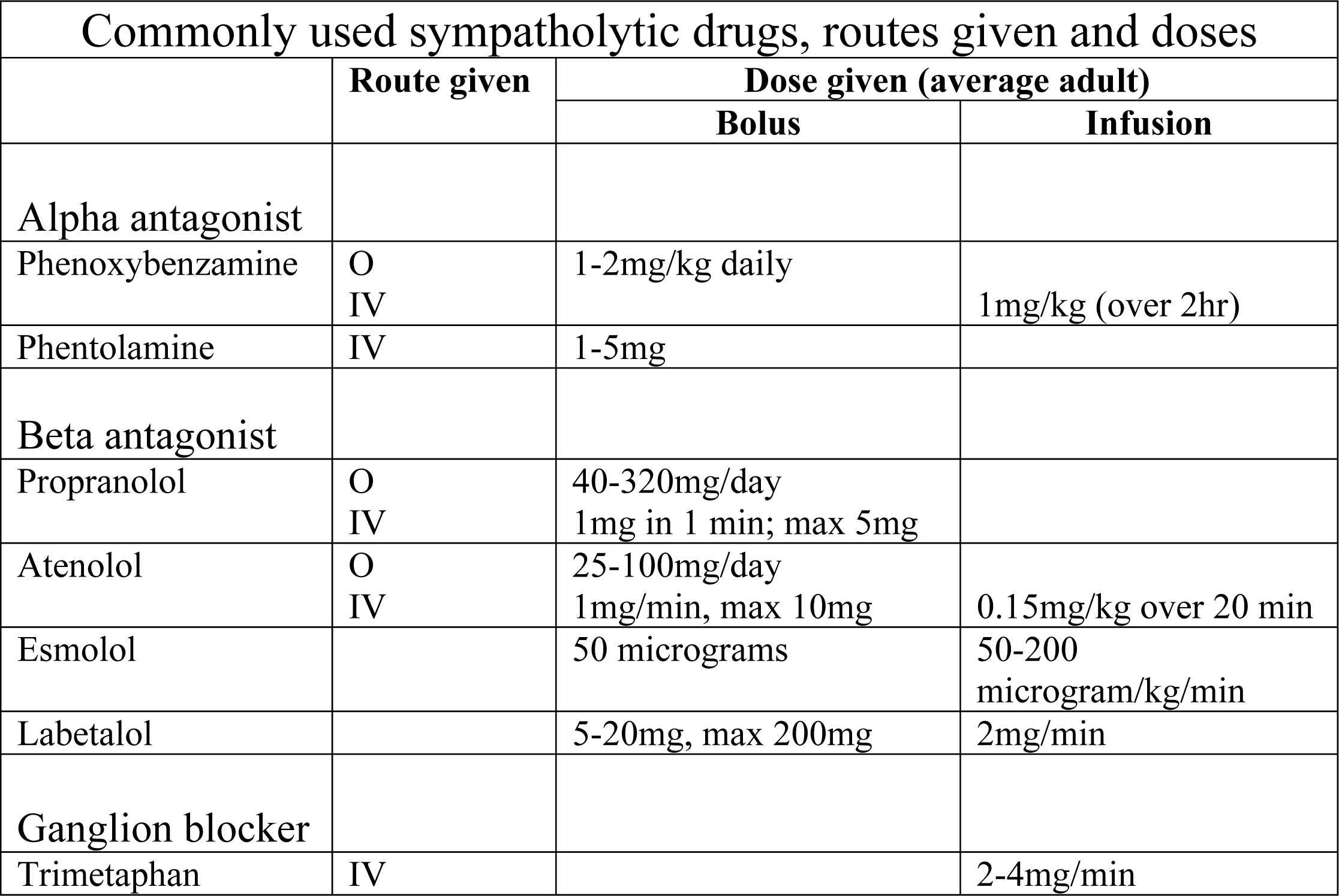
Sympatholytics
These drugs block either alpha or beta adrenergic receptors. It is also possible to have a sympatholytic action by blocking the sympathetic ganglia; only one drug is available to achieve this clinically.
Alpha receptor antagonists (alpha blockers)
Phenoxybenzamine: a non-specific, irreversible alpha-1 and alpha-2 antagonist. The alpha-2 blockade leads to increased noradrenaline release and a beta-receptor mediated compensatory tachycardia. Consequently non-specific alpha-blockers are often given concurrently with a beta adrenoreceptor antagonist to block this effect (see below). Mainly used orally to induce hypotension, particularly in the management of phaeochromocytoma.
Phentolamine: has similar CVS effects to phenoxybenzamine but the alpha blockade is shorter acting and reversible with alpha-agonists.
Tolazoline: mainly used as a pulmonary vasodilator to treat persistent pulmonary hypertension in neonates.
Prazosin and Doxazosin: selective alpha-1 antagonists which cause vasodilation and hypotension, but a lesser degree of compensatory tachycardia. Mainly used as adjuncts in the control of hypertension.
Beta receptor antagonists (beta blockers)
Since they were first synthesized over 50 years ago, “beta blockers” have evolved into a large family of drugs. The ones below are used to illustrate the key features of the differences between members of this family.
Propranolol: relatively non-specific antagonist, blocking both beta-1 and beta-2 receptors. Decreases heart rate, blood pressure and cardiac output. Increases airway resistance in patients with asthma and COPD. Inhibits glucose metabolism and blocks sympathetic mediated “warning sings” of hypoglycaemia in diabetics. May adversely affect lipid profile. Its main use now is in the control of thyrotoxicosis, treatment of essential tremor, migraine and control of the somatic manifestations of stress.
Atenolol, metoprolol: due to their predominance in blocking beta-1 receptors present in the myocardium they are often called “cardioselective”. In reality, although cardioselective beta-blockers have a predilection for beta-1 receptors, at higher doses they become less specific, blocking both beta-1 and 2 receptors. Beta-1 receptor blockade reduces heart rate, cardiac output, blood pressure and thus myocardial oxygen demand. In addition, a lusitropic action (an increase in diastolic time) increases coronary blood flow. Mainly used in the treatment of hypertension and ischaemic heart disease.
Oxprenolol: a relatively non-specific antagonist, blocking both beta-1 and beta-2 receptors but also with some partial beta-2 agonist action (intrinsic sympathomimetic activity). Thought to be therapeutically beneficial. Mainly used as an antihypertensive.
Esmolol: a relatively specific beta-1 antagonist, esmolol is metabolised by red cell esterases and hence has a very short half-life. Its peak effects occur within 6-10 minutes of being given, but have almost completely disappeared by 20 minutes. Esmolol is only available for intravenous use. Useful for rapid control of hypertensive episodes such as those associated with tracheal intubation and for treatment of supraventricular tachycardias.
Sotalol: a non-specific beta antagonist, which also has class III antiarhythmic activity. Used for prophylaxis of paroxysmal supraventricular tachycardias and ventricular ectopics. May induce torsade des pointes in susceptible patients.
Labetalol: a non-specific alpha and beta receptor antagonist. When given intravenously, the ratio of beta to alpha activity is approximately 7:1. Ideal for the control of acute hypertensive episodes, or for hypotensive anaesthesia.
Evidence has been published which suggests peri-operative beta blockade reduces the incidence of cardiac morbidity and mortality in high cardiac risk patients undergoing major surgery. The individual drugs, patient groups, and duration of beta blockade are still debated.
Ganglion blockers
This group of drugs acts by inhibiting the postsynaptic actions of acetylcholine at autonomic ganglia.
Trimetaphan: the only drug in this group still in clinical use today. It causes profound peripheral vasodilatation and hypotension, reduces cardiac output and coronary and renal blood flow. It is very short acting and usually given by slow intravenous infusion to induce controlled hypotension. Causes a reflex tachycardia and tachyphylaxis is common. Not surprisingly, it also causes some degree of non-depolarizing neuromuscular block.
Pharmacology of the Parasympathetic Nervous System
Most of the effects of the parasympathetic nervous system are mediated through acetylcholine released from post-ganglionic nerve terminals and acting at muscarinic receptors. Muscarinic receptors are membrane-spanning protein structures which function as ion-channels. Several subtypes of muscarinic receptor have been identified, numbered M1-M5.
- M1 receptors stimulate gastric acid secretion
- M2 receptors are thought to mediate the negative chronotropic effects of parasympathetic stimulation
- M3 receptors mediate lacrimal and salivary gland secretion, and may also be involved in gut smooth muscle contraction.
- M4 and M5 subtypes are thought to be present mainly in the CNS, though M4 receptors may also mediate adrenaline secretion from the adrenal medulla.
Muscarinic receptors are the main target of drugs that act directly on the parasympathetic nervous system. In general though, both agonists and antagonists show little specificity for the different subtypes of muscarinic receptor.
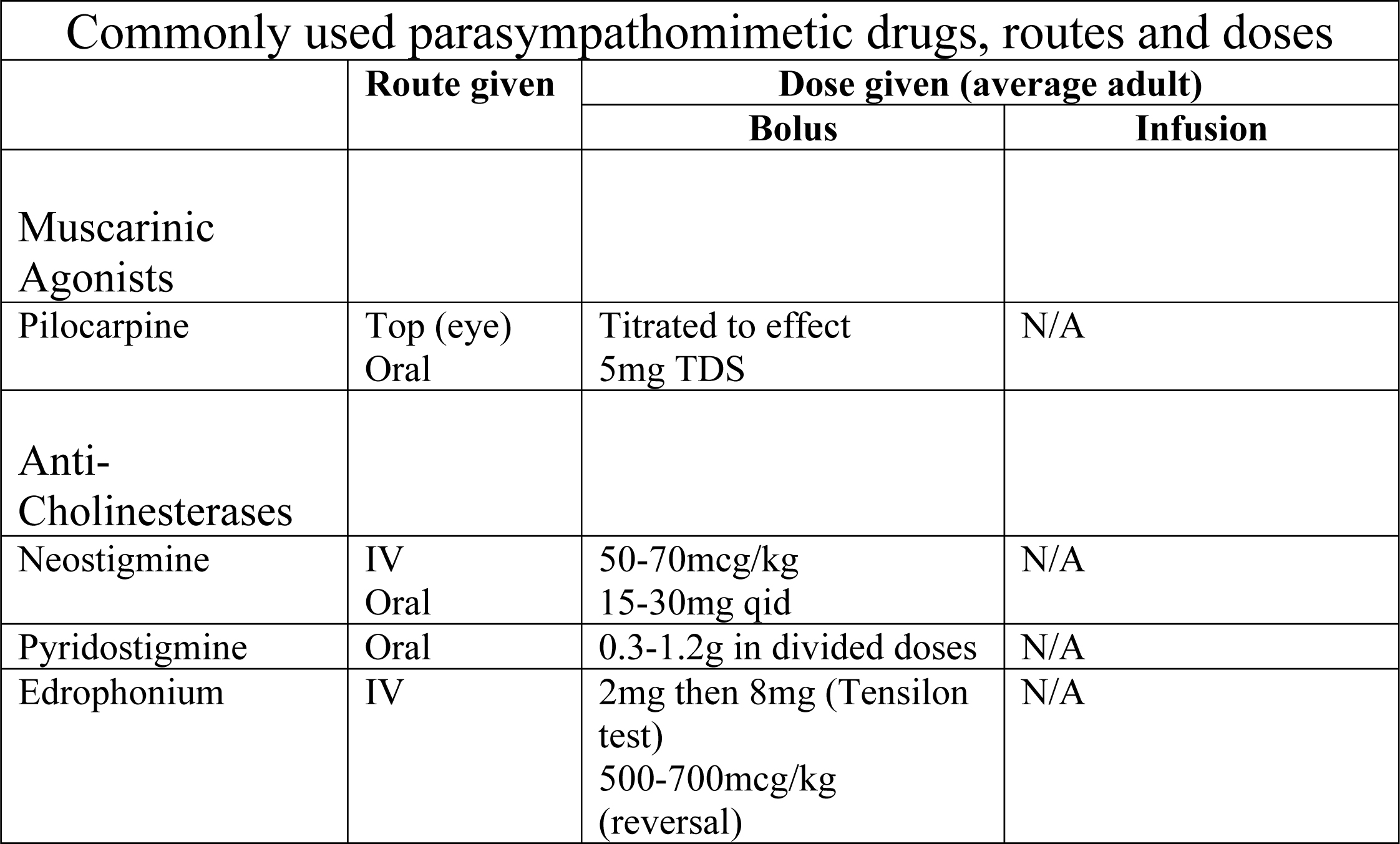
Parasympathomimetics
Muscarinic Receptor Agonists
Direct acting muscarinic agonists are relatively infrequently used in clinical practice, but they are still used in a few specific cases.
Pilocarpine: a semi-synthetic alkaloid, which is a probably the most widely used direct muscarinic agonist. Pilocarpine is mainly used topically in the treatment of glaucoma, but has been used systemically to treat xerostomia. Systemic effects include hypotension and bradycardia, bronchoconstriction, bronchorrhoea and sialorrhoea.
Acetyl-cholinesterase Inhibitors
As anaesthetists, we most commonly see parasympathomimetic actions of drugs following administration of the cholinesterase inhibitors during reversal of neuromuscular blockade. Hence it is appropriate to discuss this group of drugs (also known as anti-cholinesterases) here. By non-specifically inhibiting the breakdown of acetylcholine in synapses, anti-cholinesterases will cause the desired improvement in neuromuscular transmission, but also widespread muscarinic receptor activation. This manifests itself as relative bradycardia, hypersalivation, increased gut smooth muscle activity and meiosis. These effects are usually counteracted by concurrent administration of a muscarinic antagonist, such as atropine or glycopyrrolate (see below).
Neostigmine: the most commonly used anti-cholinesterase. Neostigmine is a carbamate ester, which reversibly inhibits acetyl cholinesterase by itself acting as a substrate. During this process, the acetyl cholinesterase molecule becomes carbamylated, and consequently inactive. Regeneration of the active enzyme occurs, but much slower than following hydrolysis of acetylcholine. A single dose of neostigmine has a peak effect at 7-10 minutes, and the effect will last for up to 1 hour. Neostigmine is available in a preparation combined with glycopyrrolate to minimise the muscarinic side effects.
Pyridostimine: shares its mode of action with neostigmine. It has a slower onset of action, and a longer duration of action than neostigmine. It can be given orally, and is consequently useful in the treatment of myaesthenia gravis.
Edrophonium bromide: or “Tensilon” is most commonly used in the diagnosis of myaesthenia gravis. It is a reversible competitive inhibitor of acetyl-cholinesterase, which prevents acetylcholine gaining access to the active site of the enzyme. The onset and duration of action of edrophonium are both significantly shorter than neostigmine (duration approximately 10 minutes).
Parasympatholytics
Muscarinic Receptor Antagonists
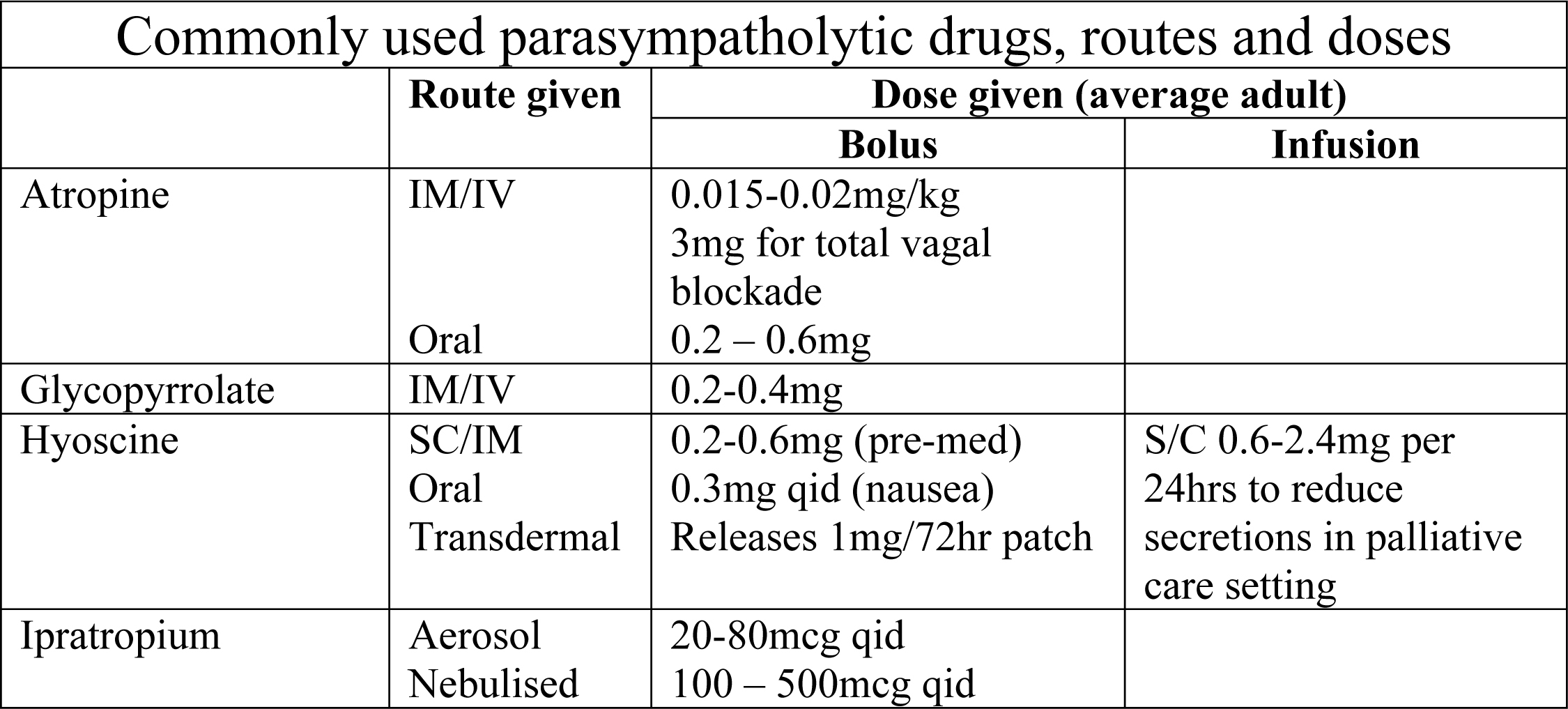
Muscarinic receptor antagonists are the drugs with a direct action on the parasympathetic nervous system, which are most frequently used in the anaesthetic setting. They are used both intra-operatively and as premedication, to treat symptomatic bradycardia and to reduce oropharyngeal and respiratory secretions.
The most commonly used agents are atropine, glycopyrrolate and hyoscine. These are all competitive, reversible, non-specific antagonists, which produce dose dependant effects. At low dose, reduced salivation, sweating & bronchial secretion predominate. At higher doses, pupillary dilatation and tachycardia are seen. Still higher doses reduce gut motility, gastric secretion & bladder muscle function.
Atropine: this naturally occurring tertiary amine is derived from the deadly nightshade plant (Atropa Belladonna). It is lipid soluble and can therefore cross the blood brain barrier, causing central as well as peripheral effects. Peripheral effects tend to predominate and include tachycardia, bronchodilation and inhibition of sweating and salivation. Atropine is commonly used in an intravenous dose of 10-20mcg/kg to treat bradycardia during anaesthesia. A dose of 3mg will produce complete vagal blockade in an adult, but such a dose is generally restricted for use in resuscitation algorithms. Smaller doses are used as an anti-sialogogue. Atropine has been linked to post-operative confusion in the elderly, probably a result of its central actions.
Hyoscine: is also a tertiary amine, and is particularly lipid soluble. Central effects thus tend to predominate – including drowsiness, amnesia and analgesia. It is also a powerful anti-sialogogue. These properties have seen hyoscine used frequently as premedication, but perhaps its most common use today is as an anti-emetic. It is particularly common in many proprietary travel sickness remedies.
Glycopyrrolate: a synthetic quaternary amine. Glycopyrrolate is strongly ionised and therefore unable to cross the blood-brain barrier. Consequently it has no central effects, and is thus an alternative to atropine in the elderly patient. It is a more potent antisialogogue than atropine, but has slightly weaker cardiac effects. This makes it an ideal agent to be used in conjunction with the anti-cholinesterases, when salivation can be controlled without precipitating potentially harmful tachycardia.
Ipratropium: a synthetic derivative of atropine, administered by nebulisation, or metered dose aerosol inhaler in the treatment of asthma. Competitive inhibition at muscarinic receptors on bronchial smooth muscle cells reduces bronchospasm, and there may also be a secondary effect reducing mast cell degranulation (which is muscarinic receptor mediated). Some systemic absorption may lead to mild tachycardia and increased cardiac output.
Pirenzepine: an unusual drug, in that it is a relatively specific inhibitor of M1 receptors. Pirenzepine reduces gastric acid secretion and reduces gut smooth muscle activity. It is used in the treatment of peptic ulcer disease, but it’s use is not widespread.
Summary
- A balance exists between sympathetic and parasympathetic outflow. Many common pathologies and surgical procedures can affect this balance, leading to disturbances in the function of organ systems.
- Drugs can contribute to autonomic disturbance, but drugs can also be used to redress the balance.
- Drugs which act on the ANS, tend to be agonists or antagonists at one or more of the various receptors, and this determines their clinical effects.
- Some drugs have slightly different modes of action (such as the anticholinesterases or phosphodiesterase inhibitors) but still have marked effects on the ANS.
Appendix 1: Commonly Used Inotropes
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/