Intensive Care Medicine

KEY POINTS
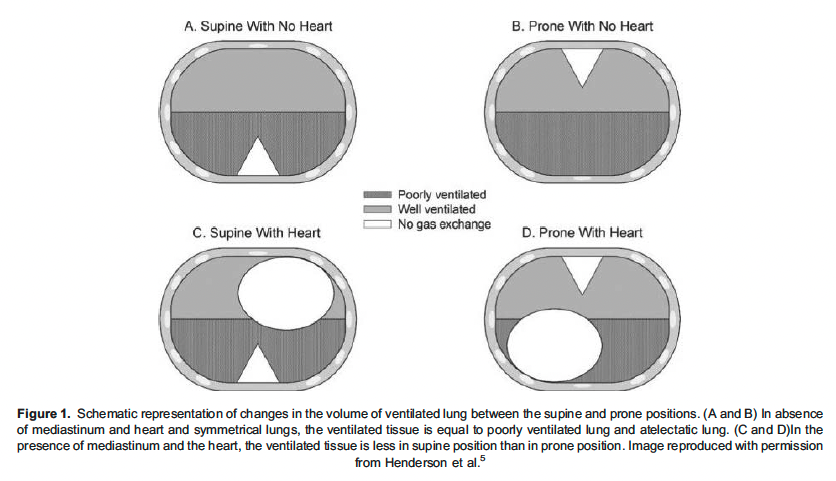
- In a prone position, overall lung compliance improves due to recruitment of the dorsal lung mass, which is anatomically greater than the ventral lung mass.
- There is a homogeneous distribution of transpulmonary pressures in the prone position due to improved dimension matching between chest wall and lung.
- Prone positioning may improve right heart function by facilitating unloading of the right ventricle.
- In the prone position, pulmonary blood flow is minimally altered and remains preferentially in dorsal regions.
- Although prone ventilation improves oxygenation, it does not necessarily improve carbon dioxide elimination.
INTRODUCTION
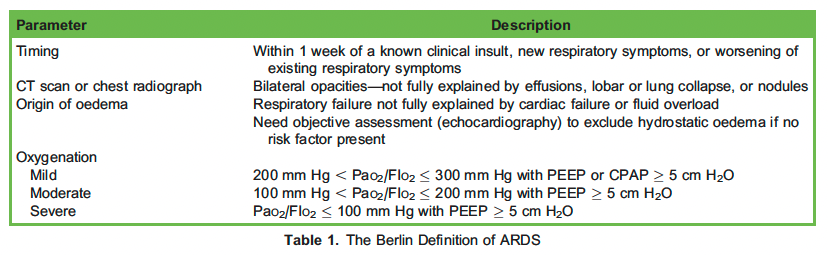
Acute respiratory distress syndrome (ARDS) was initially defined in 1994 by the American-European Consensus Conference. This definition saw several changes culminating in the Berlin Definition in 20111 (Table 1). The existence of a definition helps to standardise clinical care and research. The Faculty of Intensive Care Medicine and Intensive Care Society Guideline Development Group have provided recommendations for managing patients with ARDS. Prone positioning (PP) is recommended if oxygenation does not improve [PaO2/FIO2 (P/F) ratio , 150 ] in the first 48hours.2
PP has been used since the 1970s as an effective method of improving gas exchange in patients with ARDS. The first published paper was by AC Bryan in 1974,3 who suggested that prone ventilation in an anaesthetized and paralyzed patient could lead to more homogenous lung inflation, improving oxygenation when compared to a supine position. Later, in 1977, Douglas et al4 used prone positioning to improve oxygenation in 4 mechanically ventilated patients with bilateral infiltrates on chest radiograph and hypoxemic respiratory failure. They performed awake PP in the fifth patient and successfully avoided intubation.4
PRONE POSITIONING IN A MECHANICALLY VENTILATED PATIENT
Physiology
The acute pulmonary hypertension in ARDS is multifactorial. It could be due to several factors including hypoxemia, hypercapnia, acidosis, orpulmonary vascular obstruction from interstitial oedema and microvascular embolization. The acute cor pulmonale in ARDS is due to increased RV afterload. There are several mechanisms through which PP helps in improving RV function. The proposed mechanisms are reduction in hypoxic pulmonary vasoconstriction leading to a decrease in pulmonary vascular tone and RV afterload and reduction in ventilatory driving pressure, which reduces pulmonary vessel compression and pulmonary vascular resistance. The PP increases the central blood volume which reduces pulmonary vascular resistance and RV afterload and leads to improved pulmonary blood flow by homogenous ventilation and thus improves oxygenation.6
The PROSEVA study (PROne ventilation in SEVere acute respiratory distress syndrome) was a multicentre prospective randomised controlled trial which showed that prone positioning decreased 28-day and 90-day mortality and increased the rate of successful extubation. Other secondary outcomes, such as time to successful extubation, barotrauma, and tracheostomy at days 28 and 90 showed no difference. Based on these data, early ventilation in the prone position is recommended in moderate to severe ARDS patients.7
Clinical Aspects
Prone positioning is just one modality used to improve gas exchange in ARDS. Other supportive management, such as positive end-expiratory pressure (PEEP), recruitment manoeuvres, fluid restriction, corticosteroids, and inhaled vasodilators such as nitric oxide can be used in addition and irrespective of patient position.
Based on recent studies, the decision to prone a patient with ARDS should be contemplated once the P/F ratio is less than 150. At least 16 hours of proning is recommended, which can be increased to 24 hours.8
As before any potentially complicated airway procedure, preoxygenation with 100% oxygen is advisable. The fraction of inspired oxygen (FIO2) can be gradually decreased after proning has been successfully completed.
Based on the recommendations from the PROSEVA trial, prone positioning can be discontinued once PaO2/FIO2 remained. 150 mm Hg 4 hours after supinating (PEEP , 10 cm H2O and FIO2 , 0.6). For initiating PP in a ventilated patient and later supination from PP, 3 to 5 caregivers are required.9
Semiprone Position
When complete prone positioning is logistically impossible or difficult or if there is a relative contraindication (eg, intra- abdominal hypertensionor recent laparotomy), a semiprone position can be adopted. TM Schmitz (1991)10 published an article describing 5 case studies involving ventilation in the semiprone position in patients with ARDS. The semiprone position was easy to adopt and required less personnel to do so.Although there was improvement in oxygenation in this position, it was not substantial when compared to the complete PP.
Use of Neuromuscular Blockers
Use of neuromuscular blocking agents (NMBA) during PP improves oxygenation but not until 48 hours and was associated with lower volutrauma and barotrauma as its use avoids high regional transpulmonary pressures. The ACURASYS (ARDS et Curarisation Systematique) trial demonstrated that rate of pneumothorax was lower in than neuromuscular blocking agent group than placebo.11 The trial also demonstrated that death at 90 days was less with neuromuscular blocking agent use than with placebo after adjusting for confounding variables like PaO2/FIO2 ratio, SAPS II (Simplified Acute Physiology Score), and end-inspiratory plateau airway pressure levels. The Faculty of Intensive Care Medicine and Intensive Care Society Guideline Development Group suggests use of cisatracurium besylate as an infusion for48 hours in moderate to severe ARDS and this is recommended during prone ventilation. 12
Enteral Feeding
Enteral feeding is generally continued safely while the patient is prone, although there are few studies to guide this aspect of care. Asystematic review and meta-analysis by Machado et al,13 suggests that the available evidence for the effect of enteral nutrition administered in the prone position for critically ill patients, in terms of gastrointestinal tolerance and clinical outcomes, is scarce. Therefore, the benefits and safety cannot be commented upon in detail.
Surgical Patients
In a surgical setting, it is traditional to use abdomino-pelvic supports (unrestricted proning) to allow free movement of the abdomen. When such supports are not used, the abdomen and chest rest directly on the mattress (restricted proning) which can increase intra-abdominal pressure and impede abdominal wall excursion.
Logistics of Proning
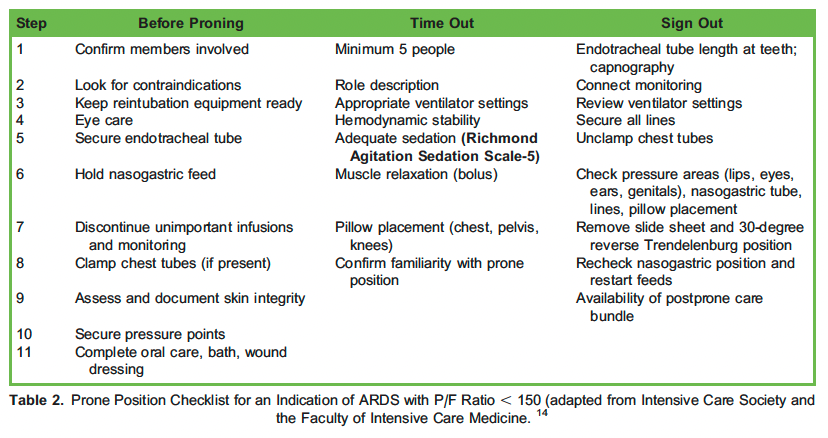
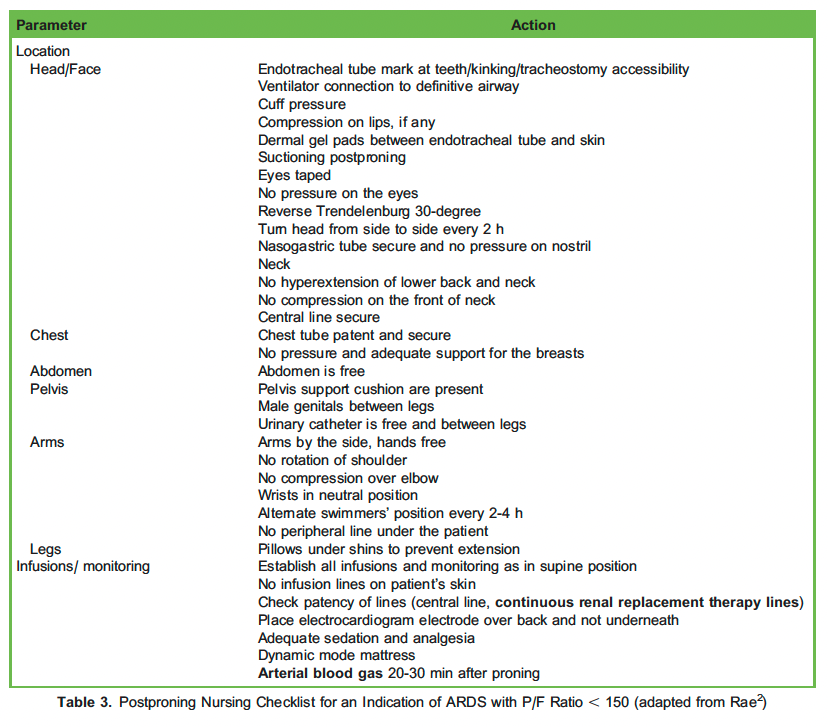
Tables 2 and 3 summarise the ‘algorithm for prone ventilation’. The algorithm has been adapted from the Intensive Care Society and Faculty of Intensive Care Medicine. 14
OTHER CONSIDERATIONS
Carbon Dioxide Elimination
Although PP improves PaO2 it does not necessarily improve carbon dioxide clearance despite homogenous aeration. Guerin et al suggested that when PaO2 increases with the initiation of prone ventilation but PaCO2 does not simultaneously decrease, it could be because either cardiac output is lowered or alveolar dead space ventilation is increased by PEEP, which is suggestive of overdistension of the lung. 9 In patients who are PaCO2 responders, the alveoli are more recruitable than in the patients who are not. Persistent hypercapnia has deleterious effects on right heart function which can correlate with poor outcomes.15
PP and Extracorporeal Membrane Oxygenation
In recent years, extracorporeal membrane oxygenation (ECMO) has become an essential tool in the care of adults and children with severe cardiac and pulmonary dysfunction that is refractory to conventional management. Based on the reports of a meta-analysis by Combes et al,16 the 90-day mortality was significantly lower with the use of ECMO than with conventional management. However, ECMO is an invasive procedure that requires arterial and venous cannulation with large-bore catheters and thereafter needs systemic anticoagulation. ECMO, therefore, carries some significant risks.
In a multicentre retrospective cohort study by Chang et al,17 the authors concluded that patients with severe influenza pneumonia-related ARDS who received PP had lower mortality rates than did those receiving ECMO at day 60. However, this was a small sample size study (n ¼ 263) and the authors suggested further studies to investigate the superiority of PP versus ECMO. Meanwhile, they recommended considering PP before initiating ECMO.
PP ventilation can be undertaken whilst simultaneously using ECMO. However, care is clearly needed during positioning to reduce complications such as catheter displacement.
Contraindications for PP
Following are the only absolute contraindications for PP in ARDS:18,19
- Unstable spine fracture
- Open chest post–cardiac surgery/trauma
- Less than 4 hours post–cardiac surgery
- Central cannulation for veno-arterial ECMO or biventricular assist device support
Prone positioning is not contraindicated in head injury patients. In patients with intracranial pressure of less than 20 mm Hg with hemodynamic stability, prone ventilation can be offered. In the absence of an intracranial pressure monitor, prone ventilation should preferably be deferred.
Following are the relative contraindications of PP:
- Hemodynamic instability; ongoing inotropes/vasopressors
- Open abdominal wounds
- Long-bone fractures
- Morbid obesity
- Late-term pregnancy
- Recent tracheostomy
- Ongoing seizures
- Raised intraocular pressure
- Severe facial fractures
Adverse Events Associated With Prone Ventilation20,21
Airway and Breathing
- Facial and airway oedema
- Kinking or displacement of endotracheal tube (accidental extubation or endobronchial intubation)
- Difficulty in endotracheal suctioning
- Barotrauma
- Desaturation (usually transient)
Circulation
- Subconjunctival haemorrhage
- Hypotension
- Arrhythmias
- Difficulty in performing cardiopulmonary resuscitation
Others
- Occlusion or accidental removal of chest tube, nasogastric tube, central lines, urinary catheter, peripheral vascular access
- Deep vein thrombosis
- Peripheral nerve injuries
- Enteral feed intolerance
- Pressure sores on the face, chest wall, and abdomen (utilisation of wound and skin care nurses has shown to reduce the incidence of pressure sores by 97%)
AWAKE PP
Traditionally, PP is employed in patients with moderate to severe ARDS who are mechanically ventilated. However, during the COVID19 pandemic, awake prone positioning was used by many clinicians in patients with moderate ARDS. Many of these patientsshowed marked improvement in P/F ratio and SpO2 with improvement in clinical symptoms and a reduced rate of intubation. These patients received either high-flow nasal oxygenation or noninvasive ventilation.22
These patients were able to tolerate the position well, could pronate and supinate themselves, and could continue oral intake as tolerated. Awake PP is cost effective, requires minimal numbers of caregivers, is easy to perform, can be performed in high- dependency units, and is associated with fewer of the adverse effects mentioned earlier.23
SUMMARY
Based on the current evidence, it is prudent to consider early PP in patients with refractory hypoxemia if not responding in the initial 48 hours in patients with moderate or severe ARDS. The duration of PP should be at least 16 hours followed by a period of supination for 4 hours. Other than improvement in oxygenation, PP can improve secretion clearance, leads to a homogeneous distribution of transpulmonary pressures, and improves right heart function.
References
- ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, et Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526-2533. doi:10.1001/jama.2012.5669
- Rae J. Acute respiratory distress syndrome. Accessed November 2, 2022. https://resources.wfsahq.org/atotw/acute-re spiratory-distress-syndrome/
- Bryan Conference on the scientific basis of respiratory therapy. Pulmonary physiotherapy in the pediatric age group. Comments of a devil’s advocate. Am Rev Respir Dis. 1974;110(6 Pt 2):143-144. doi:10.1164/arrd.1974.110.6P2.143
- Douglas WW, Rehder K, Beynen FM, Sessler AD, Marsh HM. Improved oxygenation in patients with acute respiratory failure: the prone position. Am Rev Respir Dis. 1977;115(4):559-566. doi:10.1164/arrd.1977.115.4.559
- Henderson WR, Griesdale DE, Dominelli P, Ronco Does prone positioning improve oxygenation and reduce mortality in patients with acute respiratory distress syndrome? Can Respir J. 2014;21(4):213-215. doi:10.1155/2014/472136
- Zochios V, Parhar K, Vieillard-Baron Protecting the right ventricle in ARDS: the role of prone ventilation. J Cardiothorac Vasc Anesth. 2018;32(5):2248-2251. doi:10.1053/j.jvca.2018.01.007
- Gue´rin C, Reignier J, Richard JC,. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159-2168. doi:10.1056/NEJMoa1214103
- Gattinoni L, Taccone P, Carlesso E, Marini JJ. Prone position in acute respiratory distress syndrome. Rationale, indications, and limits. Am J Respir Crit Care Med. 2013;188(11):1286-1293. doi:10.1164/rccm.201308-1532CI
- Gue´rin C, Albert RK, Beitler J, et Prone position in ARDS patients: why, when, how and for whom. Intensive Care Med. 2020;46(12):2385-2396. doi:10.1007/s00134-020-06306-w
- Schmitz TM. The semi-prone position in ARDS: five case studies. Crit Care Nurse. 1991;11(5):22, 25-26, 28-30 passim. doi:10.4037/ccn1991.11.5.22
- Papazian L, Forel JM, Gacouin A, et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363(12):1107-1116. doi:10.1056/NEJMoa1005372
- Griffiths MJD, McAuley DF, Perkins GD, et Guidelines on the management of acute respiratory distress syndrome. BMJ Open Respir Res. 2019; 6(1):e000420. doi: 10.1136/bmjresp-2019-000420.
- Machado LS, Rizzi P, Silva Administration of enteral nutrition in the prone position, gastric residual volume and other clinical outcomes in critically ill patients: a systematic review. Rev Bras Ter Intensiva. 2020;32(1):133-142. doi:10.5935/ 0103-507x.20200019.0
- Intensive Care Society, Faculty of Intensive Care Medicine. New guidance for prone positioning in adult critical care. Accessed on November 8th, 2022.. https://ics.ac.uk/resource/new-guidance-for-prone-positioning-in-adult-critical-care. html
- Gattinoni L, Vagginelli F, Carlesso E, et al. Decrease in PaCO2 with prone position is predictive of improved outcome in acute respiratorydistress Crit Care Med. 2003;31(12):2727-2733. doi:10.1097/01.CCM.0000098032.34052.F9
- Combes A, Hajage D, Capellier G, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med. 2018;378(21):1965-1975. doi:10.1056/NEJMoa1800385
- Chang KW, Hu HC, Chiu LC, et Comparison of prone positioning and extracorporeal membrane oxygenation in acute respiratory distress syndrome: a multicenter cohort study and propensity-matched analysis. J Formos Med Assoc. 2022;121(6):1149-1158. doi: 10.1016/j.jfma.2021.10.007
- Bruni A, Garofalo E, Longhini Avoiding complications during prone position ventilation. Intensive Crit Care Nurs. 2021; 66:103064. doi: 10.1016/j.iccn.2021.103064.
- Reinprecht A, Greher M, Wolfsberger S, Dietrich W, Illievich UM, Gruber A. Prone position in subarachnoid hemorrhage patients with acute respiratory distress syndrome: effects on cerebral tissue oxygenation and intracranial pressure. Crit Care Med. 2003;31(6):1831-1838. doi: 10.1097/01.CCM.0000063453.93855.0A
- Gonza´lez-Seguel F, Pinto-Concha JJ, Aranis N, Leppe J. Adverse events of prone positioning in mechanically ventilated adults with ARDS. Respir Care. 2021;66(12):1898-1911. doi:10.4187/respcare.09194
- Johnson C, Giordano NA, Patel L, et Pressure injury outcomes of a prone-positioning protocol in patients with COVID and ARDS. Am J Crit Care. 2022;31(1):34-41.
- Dhrmann S, Li J, Ibarra-Estrada M, et al. Awake prone positioning for COVID-19 acute hypoxaemic respiratory failure: a randomised, controlled, multinational, open-label meta-trial. Lancet Respir Med. 2021;9(12):1387-1395. doi:10.1016/ S2213-2600(21)00356-8
- Singh P, Jain P, Deewan Awake prone positioning in COVID-19 Patients. Indian J Crit Care Med. 2020;24(10):914-918. doi:10.5005/jp-journals-10071-23546
- Pelosi P, Brazzi L, Gattinoni Prone position in acute respiratory distress syndrome. Eur Respir J. 2002; 20(4):1017-28. doi: 10.1183/09031936.02.00401702.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/