Obstetrics Anaesthesia

KEY POINTS
- Ambulatory labour epidurals that preserve motor function have several potential advantages, such as lower instrumental delivery rates and higher maternal satisfaction.
- Avoiding high-dose local anaesthetic test doses reduces motor blockade and facilitates ambulatory labour epidurals.
- Programmed intermittent epidural boluses provide greater sensory dermatomal spread with less motor blockade when compared to continuous epidural infusions, so may be a superior maintenance technique for ambulatory labour epidurals.
- Patient selection and education, and establishing appropriate hospital policies are required for safe ‘walking
epidurals’.
INTRODUCTION
Traditionally once a woman receives a labour epidural she is managed in bed in a wedged supine, or lithotomy, position. The ‘walking’ or ‘ambulatory’ epidural first appeared in the early 1990s in an attempt to improve freedom of mobilisation, whilst maintaining effective epidural analgesia.1 The possibilities of being able to walk to the washroom, to sit in a chair, or to have less motor block are desirable to some parturients, and provide additional benefits to the foetus and healthcare workers. Not all women, however, will choose to ambulate once they are comfortable with a labour epidural.
BENEFITS OF AMBULATORY EPIDURAL ANALGESIA
Suggested benefits for the mother include
- Lower instrumental delivery rates2
- Reduced need for urinary catheterisation3,4
- Less motor block5
- Less impact on blood pressure1
- Improved maternal satisfaction5
- Less pain, better uterine contractions and shortened duration of labour if upright during the first stage of labour6,7
Ambulation benefits the foetus by minimising aortocaval compression and facilitating labour progression. Improved patient mobility also benefits bedside staff by reducing the need for manual handling.1
RISKS OF AMBULATORY EPIDURAL ANALGESIA
Elimination of Lidocaine Test Dose
In order to facilitate an ambulatory epidural, there has been an evolution to preserve motor function, and to use low concentration local anaesthetic (eg 5 mL of 0.1% bupivacaine) without epinephrine as an induction dose.8 This may contradict the traditional use of 1.5% to 2% lidocaine with epinephrine as the ‘test dose’ to identify inadvertent intrathecal or intravascular catheter placement. However, epinephrine is unreliable for detecting intravascular injection in a labouring patient as the associated transient tachycardia seen is difficult to distinguish from the tachycardia caused by contraction pain. As always, clinicians should be diligent when bolusing catheters to monitor for inadvertent intrathecal or intravascular injections, and each bolus should be treated as a test dose.
Potential Falls
The concern about falls risk may lead to hesitation in institutions adopting ambulatory epidurals. Falls can potentially result from postural hypotension from vasodilatation. This is minimised by the use of a lower-concentration local anaesthetic solution in the ‘walking epidurals’. Nevertheless, symptomatic postural hypotension should be actively monitored for prior to mobilisation.9 Theoretically, somatosensory perception may be impaired by epidural analgesia, affecting proprioception and balance. However, studies comparing women in labour with and without combined spinal-epidural (CSE) analgesia have shown no differences in balance measured with posturography.10,11
ACHIEVING SAFE AMBULATORY EPIDURAL ANALGESIA FOR LABOUR
Patient Selection
Patients must first be screened for any contraindications to ambulatory epidural analgesia, which include the following:
- Abnormal foetal heart rate
- Hemodynamic instability
- Significant antepartum haemorrhage
- Unstable foetal lie
Neuraxial Insertion
An epidural or CSE technique can be used. If a CSE is chosen, follow these procedures:
- For the intrathecal component, consider an opioid-only technique (eg 10-15 µg fentanyl; 25 µg fentanyl is associated with foetal bradycardia12) or an opioid and low-dose local anaesthetic (eg bupivacaine ≤ 2.5 mg).
- For the epidural component, avoid a 1.5% to 2% lidocaine test dose to reduce the incidence of significant motor or proprioceptive block.
- If a test dose is not performed, the induction dose will be the first bolus delivered via the epidural catheter during ambulatory epidural analgesia. The induction dose should be a low-concentration solution (eg 10 mL bupivacaine ≤ 0.1%) in fractionated doses (eg 5 mLs) with careful monitoring and clinical observation.
Epidural Maintenance
Epidural solution
Consider a low-concentration solution (eg bupivacaine 0.0625%-0.08% bupivacaine) with or without a short-acting opioid (eg 2µg/mL fentanyl or 0.4 µg/mL sufentanil) to preserve motor function.
Continuous Epidural Infusion Versus Programmed Intermittent Epidural Bolus
Programmed intermittent epidural bolus (PIEB) administration (using an appropriate epidural pump) generates greater pressure and spread of solution within the epidural space.13 This results in greater sensory dermatomal spread and less motor blockade when compared to continuous epidural infusion (CEI). A recent systematic review and meta-analysis demonstrated that a PIEB regime leads to less local anaesthetic consumption, shorter duration of second stage of labour, and higher maternal satisfaction.14 Another study found decreased motor blockade (37% versus 2.7%) and fewer subsequent instrumental deliveries (20% versus 7%).5 PIEB increases the likelihood of successful ambulation when compared with CEI (Figure 1).15
PIEB Settings
Infusion pumps such as the CADD Solis Ambulatory Infusion Pump (Smiths Medical, Saint Paul, Minnesota) will deliver PIEB. Although the optimal PIEB regime is not yet known, volumes of 5 to 10 mL every 45 to 60 minutes, with the first bolus 30 to 60 minutes after the induction bolus dose have been suggested.16 See below for published definitions and common settings of PIEB and patient-controlled epidural analgesia (PCEA) parameters (Table 1).
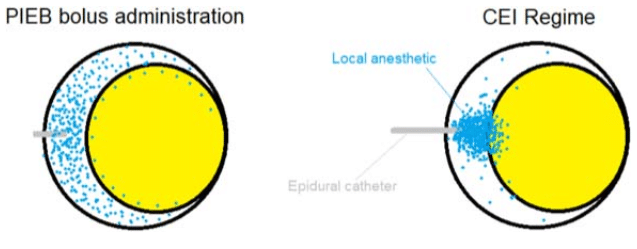
Figure 1. Programmed intermittent epidural bolus PIEB regime distributes local anaesthetic more uniformly with each bolus (delivered at a high infusion rate producing a greater pressure), providing better spread throughout the epidural space when compared to the continuous epidural infusion CEI regime (with a lower infusion rate).
Benefits of PCEA
In addition to regular PIEB, patients may benefit from PCEA, which allows self-administered boluses by the patient for breakthrough pain. PCEA has been shown to increase maternal satisfaction and decrease the need for intervention by the anaesthetist. The combination of PIEB and PCEA techniques have been recommended in the latest practical guidelines for Obstetric Anesthesia by the American Society of Anesthesiology.18
Before Ambulating
Prior to ambulating, women should be routinely assessed for motor block and postural hypotension using the following guidelines:
- Supine and sitting blood pressure readings within 15% of each other
- No dizziness experienced when moving from sitting to standing position
- Sensation in the feet described as normal or near normal
- Successful completion of the step test. During this test, patients are asked to demonstrate motor strength by stepping up onto a stool under close supervision. Ability to complete this task corresponds to a modified Bromage score of 6 (Table 2).
During Ambulation
Once the criteria above are met, women should be encouraged to
- Use the commode or bathroom facilities with assistance
- Sit out of bed in a chair (if sitting for >60 minutes, repeat the prior-to-ambulation assessments)
- Ambulate in the delivery suite with assistance at all times.
If the modified Bromage score is 5 (ie failed step test), the woman may only do the following with close assistance:
- Use the bathroom
- Sit in a chair
- Ambulate in her room
Monitoring should consist of the following:
- Vital signs (blood pressure, heart rate, respirations) every hour
- Fetal heart rate (according to local policy)
Implementation and Hospital Policy
Hospitals should have up-to-date policies in place to allow women to mobilise after receiving an ambulatory labour epidural.1 Prior to implementation, anaesthetists, obstetricians, midwives, nursing staff, and trainees should be educated to understand the terminology and technology as well as the risks and benefits of this technique.
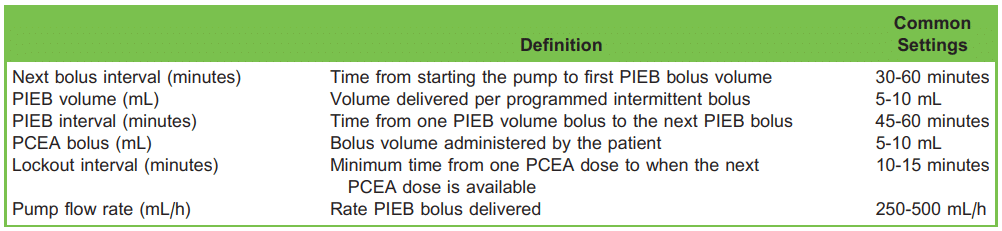
Table 1. Programmed Intermittent Epidural Bolus Parameters and Common Setting.17 PIEB indicates programmed intermittent epidural Bolus; PCEA, patient-controlled epidural analgesia. Bupivacaine: 0.0625% to 0.08%; 2 µg/mL fentanyl or 0.4 µg/mL sufentanil, staying below each patient’s weight-based toxic dose.
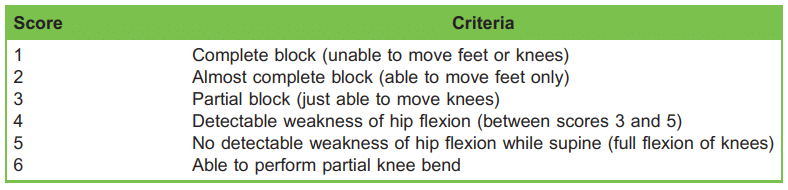
Table 2. Modified Bromage Score15
SUMMARY
Compared to traditional labour epidural analgesia, ambulatory epidurals (with consideration of using a PIEB regime rather than a CEI regime) have shown several benefits, such as less motor block, lower instrumental delivery rates, reduced need for urinary catheterisation, less impact on blood pressure, improved maternal satisfaction, and reduced workload for bedside staff. Ambulatory epidurals can be initiated with a CSE or epidural technique with fractionated low-dose epidural boluses replacing a traditional test dose. To improve patient safety, careful selection should be employed as well as close monitoring using tools such as the modified Bromage score. To achieve successful implementation, hospitals should develop site-specific policies and aim to keep members of the interdisciplinary team up-to-date with current literature, data and outcomes.
REFERENCES
- Preston R. Walking epidurals for labour analgesia: do they benefit anyone? Can J Anaesth. 2010;57:103-106.
- Effect of low-dose mobile versus traditional epidural techniques on mode of delivery: a randomised controlled trial. Lancet. 2001;358:19-23.
- Wilson MJ, Macarthur C, Shennan A. Urinary catheterization in labour with high-dose vs mobile epidural analgesia: a randomized controlled trial. Br J Anaesth. 2009;102:97-103.
- Weiniger CF, Yaghmour H, Nadjari M, et al. Walking reduces the post-void residual volume in parturients with epidural analgesia for labor: a randomized-controlled study. Acta Anaesthesiol Scand. 2009;53:665-672.
- Capogna G, Camorcia M, Stirparo S, et al. Programmed intermittent epidural bolus versus continuous epidural infusion for labor analgesia: the effects on maternal motor function and labor outcome. A randomized double-blind study in nulliparous women. Anesth Analg. 2011;113:826-831.
- Lawrence A, Lewis L, Hofmeyr GJ, et al. Maternal positions and mobility during first stage labour. Cochrane Database Syst Rev. 2009: Cd003934.
- Kemp E, Kingswood CJ, Kibuka M, et al. Position in the second stage of labour for women with epidural anaesthesia. Cochrane Database Syst Rev. 2013:Cd008070.
- Camorcia M. Testing the epidural catheter. Curr Opin Anaesthesiol. 2009;22:336-340.
- Shennan A, Cooke V, Lloyd-Jones F, et al. Blood pressure changes during labour and whilst ambulating with combined spinal epidural analgesia. Br J Obstet Gynaecol. 1995;102:192-197.
- Pickering AE, Parry MG, Ousta B, et al. Effect of combined spinal-epidural ambulatory labor analgesia on balance. Anesthesiology. 1999;91:436-441.
- Davies J, Fernando R, McLeod A, et al. Postural stability following ambulatory regional analgesia for labor. Anesthesiology. 2002;97:1576-1581.
- Engel N. Labour analgesia effects on foetal heart rate. A mini-review. Open J Obstet Gynecol. 2011;1:113-120.
- Kaynar AM, Shankar KB. Epidural infusion: continuous or bolus? Anesth Analg. 1999;89:534.
- George RB, Allen TK, Habib AS. Intermittent epidural bolus compared with continuous epidural infusions for labor analgesia: a systematic review and meta-analysis. Anesth Analg. 2013;116:133-144.
- Breen TW, Shapiro T, Glass B, et al. Epidural anesthesia for labor in an ambulatory patient. Anesth Analg. 1993;77:919- 924.
- Carvalho B, George RB, Cobb B, et al. Implementation of programmed intermittent epidural bolus for the maintenance of labor analgesia. Anesth Analg. 2016;123:965-971.
- Chau A, Tsen LC. Update on modalities and techniques for labor epidural analgesia and anesthesia. Adv Anesth 2018;36:139-162.
- The American Society of Anesthesiologists Committee on Standards and Practice Parameters and the Task Force on Obstetric Anesthesia and the Society for Obstetric Anesthesia and Perinatology. Practice guidelines for obstetric anesthesia: an updated report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia and the Society for Obstetric Anesthesia and Perinatology. Anesthesiology. 2016;124:270-300.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/