Paediatric Anaesthesia

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Regarding the pre-operative psychological preparation of a five year old, the following statements are true:
- Five-year-olds readily accept surrogates instead of parents.
- It is the age when ‘stormy’ inductions are most likely.
- They tend to take the things that are said to them literally.
- They generally respond best to a full explanation of what is to happen.
- They are the age group most likely to suffer separation anxiety.
- With respect to ex-premature babies scheduled for surgery, are the following statements true or false?
- They should all receive daycase surgery where possible to minimise disruption to their routine.
- They are at risk of central apnoea following surgery
- It is important to confirm gestational age at birth in all neonates presenting for surgery
- They are at risk of perioperative bradycardia
- Daycase surgery is contra-indicated until after the first year of life
- Considering fasting prior to surgery, the following statements are true:
- Cows milk generally empties from the stomach faster than human milk.
- Clear fluids should be allowed up to 30 minutes prior to surgery.
- Starvation of over 12 hours reduces the incidence of post-operative nausea and vomiting.
- Prolonged starvation has been shown to increase the volume of gastric contents.
- Child behaviour can be improved by minimising starvation times.
- A 2yr old child presents for an emergency laparotomy for an incarcerated hernia. Capillary refill is 6s, cool peripheries, normal blood pressure, sinus tachycardia and tachypnoea. The following statements are true:
- Blood pressure is a sensitive marker for shock.
- Surgery should be delayed for fluid resuscitation.
- Hypovolaemia should be corrected over 24 hours.
- They are shocked.
- Blood sugar should be measured.
- Concerning parental presence at induction, the following statements are true.
- Most parents find attending their child’s induction stressful
- After attending their child’s induction, most parents would choose to do it again.
- It is of particular benefit for the induction of neonates.
- Parental presence at induction should always be determined by the parent’s wishes.
- There may be advantages of parental presence during child resuscitation.
- Considering premedicating a child, the following are true:
- Local anaesthetic cream is helpful if an intravenous induction is planned.
- Oral analgesics should be avoided because the child is nil-by-mouth.
- The dose of oral midazolam for a 20kg child is 10mg.
- Anxiolytic premedication has become more frequently used in recent years.
- Anxiolytics should never be used in children with obstructive sleep apnoea.
INTRODUCTION
Good preoperative assessment and preparation of children for surgery is important. This article reviews the preparation of children for elective and emergency surgery, including psychological preparation.
1: WHY DO CHILDREN REQUIRE A DIFFERENT APPROACH?
There are fundamental differences between children and adults that necessitate a tailored approach to preoperative preparation.
a) Physiological
The majority of children presenting for elective surgery are systemically well and require little in the way of complex physiological assessment and investigation. However, some children can present with complex congenital disease or unusual syndromes that can require specific preoperative investigation and preparation. Previously fit children presenting for emergency surgery may become very unwell, very quickly – this group of children must be recognised so that their condition is optimised prior to surgery.
b) Psychological
In comparison to adults, children are more likely to demonstrate behavioural problems at induction of anaesthesia. Psychological development is related to the age of the child (table 1).
Behavioural differences can result in a stormy anaesthetic induction and post-operative psychological difficulties such as nightmares, phobias, fears and negativism. Post-operative psychological problems are more likely to occur in:
- children aged between 2 and 3
- children displaying a withdrawn affect pre-operatively
- a difficult, stressful induction
- a child with a history of multiple procedures.
It is important that the anaesthetist is aware of these factors and can manage them effectively, both to improve the perioperative experience for the child, also to shape long term attitudes of the child to healthcare.
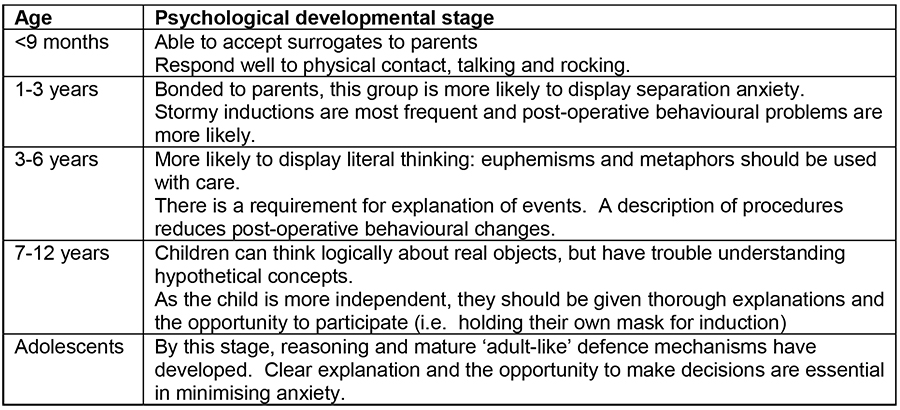
Table 1: Psychological developmental milestones
2: ELECTIVE SURGERY
Children are frequently admitted on the day of surgery, leaving little time for preparation or for the child to adjust to their surroundings. Preadmission programmes are now used in around 80% of UK children’s hospitals as an aid to preparation of the child for surgery. Many such programmes have been described and centre on a pre-assessment visit during which psychological preparation can also be addressed. Programmes may include a tour of the children’s unit, videos, printed material and the use of play, including role rehearsal. The disadvantages of such programmes are that they are labour intensive, expensive and time consuming. There is also little evidence that programmes reduce problems at anaesthetic induction itself or have any longer term advantage.
Day case surgery provides the least disruption to the child’s routine and has been shown to reduce post-operative behavioural problems; it should be encouraged where possible. Over 60% of paediatric surgery in the USA is now completed as day case procedures.
Prior to the day of surgery
There are several approaches to preassessment. Telephone screening is popular in the US and can be particularly useful if the child lives far from the hospital. Nurse-led preassessment clinics are also popular in the UK. Many institutions have produced a proforma as part of the pre-operative pathway, allowing for a thorough history to be taken by the nurse. All available notes, including clinic letters should be retrieved for review. This allows screening for suitability for day surgery, requirements for further investigation, special precautions for anaesthesia and, ultimately, can reduce day-of-surgery cancellations. Clear guidelines are used to determine whether referral to an anaesthetist for further assessment is required prior to surgery. Preadmission information may be given to the parents, supplemented by written information. A selection of common issues encountered in pre-operative screening and their implications are indicated in table 2.

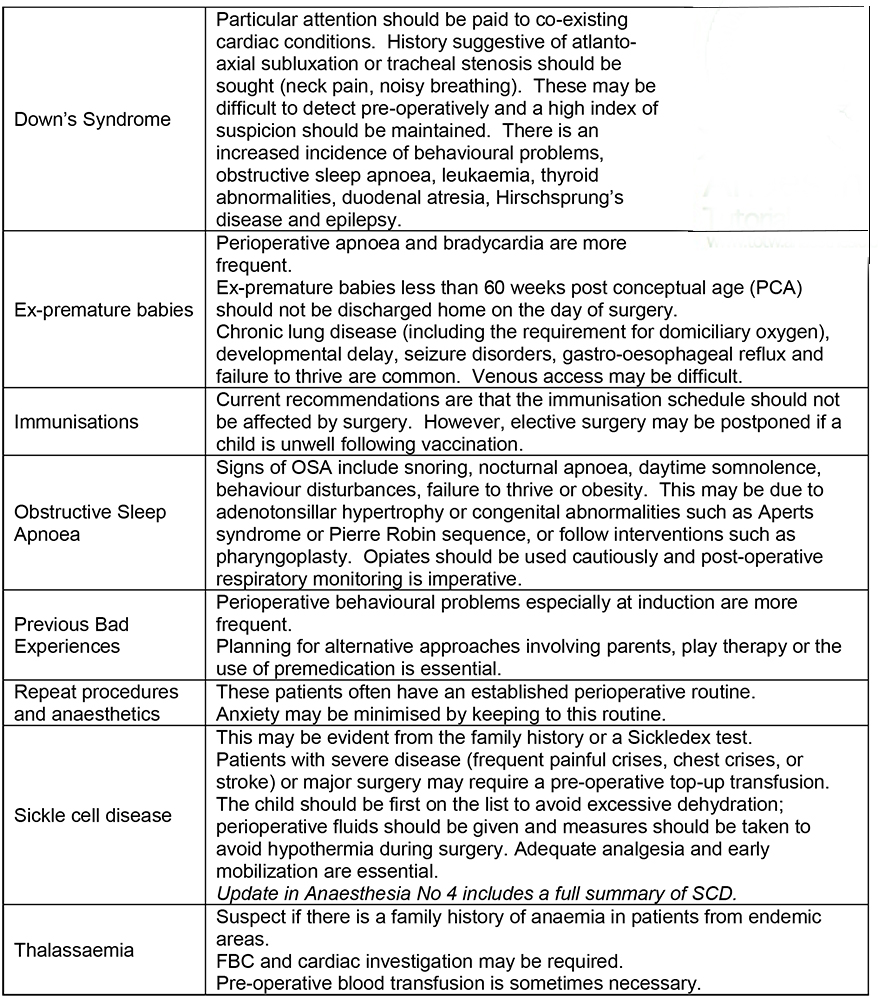
Table 2: Common issues encountered in pre-operative screening
An assessment of the social situation is also important when assessing suitability for day surgery. Complex family dynamics including the identity of legal guardians should be confirmed. The family should have access to suitable transport from the hospital with one carer free, (i.e. not driving), should live less than one hour from the hospital, and should have access to a telephone. An adult should be present at home for 24 hours after surgery and it is advisable for the family to purchase suitable analgesics in advance.
Preassessment visit
a) Explanation of procedures
Pre-assessment should allow for a thorough explanation of the perioperative sequence of events to the parent and child. Preparation of the parent is crucial in reducing parental anxiety. Parents should be encouraged to ask questions about any concerns they may have. It has been shown that children with anxious parents are more likely to display signs of perioperative anxiety themselves.
Explanation may be given through the use of videos, booklets and written instructions as well as face-to-face. If the use of interpreters is necessary, information given should be supplemented by written explanation and instructions in the patients own language.
b) Instructions
Written instructions should be used where possible to reduce confusion and increase compliance. Particular emphasis should be given to perioperative fasting and instructions regarding regular medication. There is much controversy as to suitable fasting limits for breast and formula milk, resulting in a lack of uniformity between institutions. In fact, even the concept of solids and liquids is difficult to fully appreciate, for example gelatine is ingested as a solid, but turns to liquid in the stomach whereas cows milk is ingested as a liquid, but turns to solid (curds) in the stomach! Although several studies have not been able to demonstrate much difference in gastric emptying rates, there is some evidence that human milk and whey-based formula empties from the stomach faster than cows-milk (casein) based formula. It is postulated that this is due to the higher protein content of casein formulas. There is great variability in gastric emptying with both milk and formula, however most authors agree that more than 2 hours is required to ensure adequate gastric emptying after human milk and probably longer for formula. Although guidelines vary between institutions, table 3 shows some standard fasting guidelines for elective surgery.
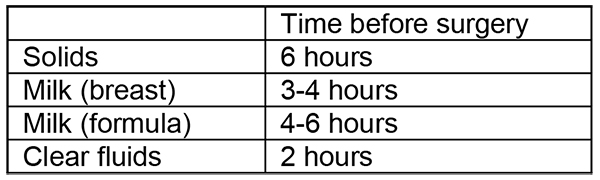
Table 3: Standard fasting guidelines for elective surgery
In recent years, there has been a greater emphasis on preventing unnecessary pre-operative fasting in children. There are many reasons why clear fluids should be encouraged up to 2 hours before surgery. Infants and small children are less able to tolerate dehydration, especially in hot environments. Nausea and vomiting is more frequent in children starved for a long period of time, hypoglycaemia can be avoided and, paradoxically, there may be an increase in gastric contents through increased secretion if starvation is prolonged. In addition, pre- and postoperative behaviour is improved by minimising fasting times.
Some units require the parent to sign a form at preassessment to ensure that they have understood pre-operative instructions.
c) Consent
The preoperative visit is the ideal opportunity to gain surgical consent for the procedure. Consent should be obtained from the parent and child if they are old enough to understand. In the UK, the child’s consent can be accepted provided they can fully understand the procedure. The process becomes complicated in the infrequent event of the child consenting whilst the parent refuses. In England, a child under the age of 16 may not refuse consent. The legal implications of this are complex, depending on the country and it may be necessary to seek legal advice.
d) Play specialists
Most UK children’s hospitals employ play specialists. As well as establishing a rapport through normal play, the specialists can explore the child’s interpretation of their operation and prepare them for their perioperative experience. For example, preparation may include the use of a doll to simulate anaesthetic induction or the use of a patient controlled analgesia. The play specialist may also identify children that fail to engage or those with particular anxiety issues that can then be dealt with effectively prior to surgery.
e) Investigations
Most children do not require routine pre-operative screening investigations unless there is a specific clinical indication such as anaemia or sickle cell disease.
Day of Surgery
Conduct on the day of surgery will be dictated, to some degree, by whether a pre- operative visit has been made. The main issues are:
a) Fasting
The fasting status should be established.
b) Preparation of child and parent
Before surgery, the anaesthetist should see the child and parent and review the pre- operative assessment. By establishing a rapport with the child, the anaesthetist can allay anxiety and reduce post-operative behavioural problems. The child should be spoken to directly in the presence of the parents to ensure a full understanding of proceedings.
The pre-assessment record should be reviewed and any new findings such as a recent URTI, gastroenteritis or change in medications should be noted.
The child should be identified with a name-band, the consent form should be reviewed and, if appropriate, the operation site marked.
The anaesthetist should examine all children preoperatively, in the presence of the parents, with particular attention to the cardiorespiratory system. This examination also helps with establishing rapport with the child and can help determine whether the child will let you near them!
The presence of a heart murmur is especially important in very young children and babies, as congenital heart disease may have gone previously un-diagnosed. Innocent murmurs tend to be quiet, early in systole, with no abnormal signs or symptoms. Pathological murmurs are diastolic, pansystolic, late systolic, loud or continuous. They are often associated with signs or symptoms suggestive of cardiac disease such as failure to thrive, recurrent chest infections, cyanosis, hypertension, radio-femoral delay, syncope cyanotic episodes.
Upper respiratory tract infection is associated with a 2-10 fold increase in peri-operative respiratory complications. Elective surgery should be postponed if there is coexisting fever, general malaise, chest signs or a productive cough. A low threshold for cancellation is also appropriate if the child is under 1 year old, has asthma or is having major surgery.
c) Investigations
Few investigations are required on the day of surgery save for the weight, blood sugar level (for diabetic children) and a peak expiratory flow rate (for brittle asthmatic children or those with an exacerbation of asthma).
d) Prescription of premedication if required (see below)
Other Issues
a) Preparation of Environment
Most children’s hospitals have a ‘child friendly’ theatre set up with brightly coloured pictures on the walls and toys (infection control should be considered when using soft toys in theatre). Even non-paediatric centres often have an area or theatre set up for children. Many departments in the UK are now using a variety of multimedia such as MP3 players, computer games, music and videos for children in the theatre complex itself.
b) Premedication
The use of premedication extends beyond that of anxiolysis. Other premedications to be considered include analgesics, antiemetics, antisialogogues, antacids and topical anaesthesia for cannula placement (such as EMLA or Ametop).
Pre-operative analgesic use has increased in recent years and is particularly useful for paracetamol administration (since the bioavailability of rectal paracetamol is comparatively poor). A small amount of water with tablets or a minimal volume of analgesic elixir is generally considered safe prior to surgery and does not significantly increase the risk of pulmonary aspiration. NSAIDs such as ibuprofen or diclofenac may also be given.
There has been a move away from routine anxiolytic premedication over the last few years. Appropriate pre-op preparation of the child combined with parental presence at induction is sufficient in the majority of cases.
There are still particular situations where anxiolytics are considered appropriate. Children presenting for multiple procedures, those with learning difficulties and extreme anxiety or uncooperative children may still benefit from premedication.
A number of anxiolytic agents have been used successfully including barbituates, opiates, benzodiazepines, chloral hydrate, ketamine and droperidol. The oral, nasal, rectal and buccal routes have all been used. Midazolam is the most frequently used pre-op anxiolytic in the UK with minimal effects on wake-up times. It may be given orally at a dose of 0.5mg/kg up to 15mg and usually results in a co-operative child after 10-15 minutes. The bitter taste may be disguised by combining with a small amount of paracetamol elixir, fruit squash or even coco-cola. Anxiolytics should be used with caution if there is a history of obstructive sleep apnoea due to the increased risk of post-operative apnoea.
c) Induction
Parental presence at induction requires preparation of the parent including a description of what to expect, including their role. The presence of parents at induction has become more common in the UK and appears to benefit both the parent and the child. Surveys of parents following inductions indicate, on the whole, that the majority would choose to do it again, despite finding it a stressful experience. In many cases, perioperative anxiety in both the parent and child are reduced.
There are certain situations when it may not be appropriate to allow parental presence. There is little benefit to children under 6 months in having a parent present and many anaesthetists chose not to have parents present for the induction of neonates and babies. Many parents may prefer not to be there for the acute management of a critically ill child (although there is evidence of the beneficial effect of parental presence for resuscitation). Finally, the anaesthetist may find that operating under the scrutiny of the parent impacts on their ability to treat the child in stressful situations.
3: EMERGENCY SURGERY
There are many additional psychological and physiological issues to take into account when preparing children for emergency surgery.
Psychological issues
By their nature, these admissions are unplanned. Pain, fear and physiological state can often result in a quiet, withdrawn child, expressing little interest in interacting with their environment. However, any child presenting in this manner should alert the anaesthetist and it should never be assumed that the child is just frightened. An immediate physiological assessment and examination should be carried out to exclude septic or hypovolaemic shock.
It is important to consider the parent: parental anxiety can present in a spectrum of behaviour from silence and crying to open aggression. This can often be attenuated, to some extent, by a full explanation of the perioperative plan.
Physiological Issues
All of the conditions outlined in table 2 can also be present in the acutely ill child and the principles of management are the same. Often patient notes are not immediately available and the need for further investigation of pre-existing disease should be weighed up against the urgency for surgery.
Children presenting for emergency surgery may be critically ill and will require thorough assessment and, if necessary, resuscitation prior to induction. Key aspects of the assessment of the critically ill child are outlined in table 4.
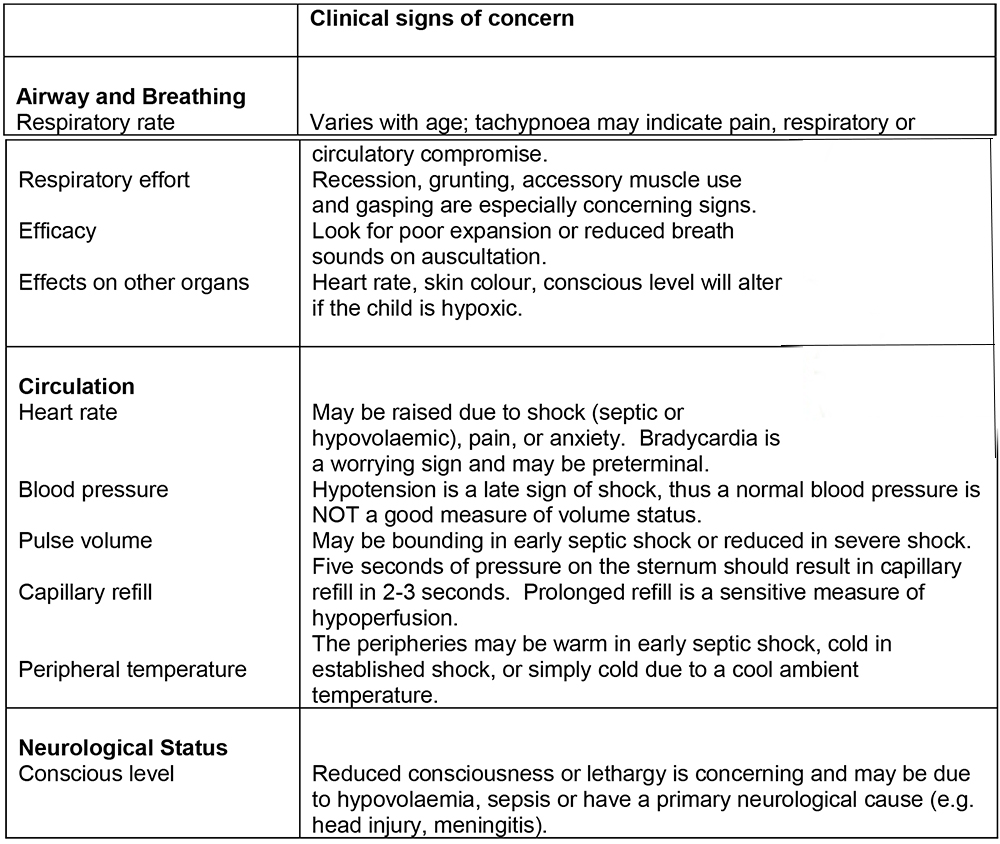
Table 4: Important signs in the assessment of the critically ill child
Failure to adequately resuscitate a critically ill child prior to induction can result in severe perioperative haemodynamic instability. Pre-operative shock may be due to hypovolaemia (e.g. trauma, dehydration, acute abdomen) or sepsis (e.g. abscess, appendicitis). The principles of management of the shocked child are as follows:
- Apply 100% oxygen, ensure adequate airway and breathing.
- Establish intravenous (or intraosseous) access.
- Give fluid bolus (isotonic crystalloid or colloid) 10-20ml/kg.
- In severe blood loss, transfusion will be required.
- Repeat fluid bolus, depending on response.
- Maintain child’s temperature.
- Surgery without adequate resuscitation should only be attempted if it is considered a necessary part of resuscitation (e.g. for haemostasis on a background of trauma).
- Anaesthetic induction and maintenance is difficult and should be managed extremely cautiously. A rapid sequence induction using judicious drug doses is usually most appropriate.
A more thorough review of the management and assessment of the critically ill child, including cardiopulmonary resuscitation can be found in the current APLS manual.
a) Fasting
Patients awaiting emergency surgery should be nil by mouth for 6 hours pre-op. However, this limit may be breached depending on surgical urgency (e.g. testicular torsion or trauma). If the child is unable to take oral fluids, it may be necessary to initiate pre-operative intravenous fluids.
b) Consent
Although it should be obtained where possible, consent is not considered absolutely necessary if emergency life-saving surgery is required and there is no parent or guardian available.
c) Investigations
Depending on the pathology, pre-operative haematological investigations are much more significant for emergency surgery. Significant electrolyte imbalance (e.g. pyloric stenosis, bowel obstruction) or anaemia (trauma) may be present and blood group typing or cross match may also be necessary. Blood sugar concentration should always be measured in a shocked child.
4: CONCLUSION
The correct preparation of children for surgery is essential to ensure a safe perioperative course and pleasant experience for the child. For elective surgery, a pre-operative visit with appropriate age- and culture-specific pre-assessment can assist in the preparation of the child and facilitates a rapport that can be continued through to the day of surgery. Although effective, pre-assessment programmes are
resource-intensive and not always feasible. By understanding the rationale behind them, simple steps can be introduced to improve the peri-operative experience for both the child and their family. Children presenting for emergency surgery may be critically ill and require a thorough physiological assessment to ensure that resuscitation measures are taken prior to induction.
ANSWERS TO QUESTIONS
- FFTTF
- FTTTF
- FFFTT
- FTFTT
- TTFFT
- TFTFF
REFERENCES and FURTHER READING
- Advanced Life Support Group. Advanced paediatric life support. The practical approach. BMJ Books/Blackwells, 2005
- Association of Paediatric Anaesthetists of Great Britain and Ireland. APA Consensus guideline on perioperative fluid management in children. v1.1 September 2007. www.apagbi.org.uk/docs/Perioperative_Fluid_Management_2007.pdf
- Armstrong TSH, Aitken HL. The developing role of play preparation in paediatric anaesthesia. Pediatric Anaesthesia 2000; 10: pp 1-4
- Brennan LJ. Modern day-case anaesthesia for children. British Journal of Anaesthesia 1999; 83(1): pp 91-103
- Brennan LJ, Prabhu AJ. Paediatric day-case anaesthesia. British journal of Anaesthesia CEPD Review 2003; 8(5): pp 134-8
- Courtman S. Children with learning disabilities. Pediatric Anesthesia 2008; 18: pp 198-207
- Ferrari LR, Rooney FM, Rockoff MA. Preoperative fasting practices in pediatrics. Anesthesiology 1999; 90: pp 978-980
- Hare A, Elliman D, Smith J. Thames PAG guidelines for immunisation and anaesthesia. http://www.ich.ucl.ac.uk/gosh/clinicalservices/thames_pag/CustomMenu_03
- Kain ZN, Caramico LA, Mayes LC, Genevro JL, Bornstein MH, Hofstadter MB. Preoperative programmes in children: a comparative examination. Anesthesia and Analgesia 1998; 87: pp 1249-55
- McGraw T. Preparing children for the operating room: psychological issues. Canadian Journal of Anaesthesia 1994; 41(11): pp 1094-1103
- Plymouth Hospitals NHS Trust: Paediatric day case integrated care pathway, 2008
- Short JA, Van der Walt, Zoanetti DC. Immunization and anesthesia- an international survey. Pediatric Anesthesia 2006; 16: pp 514-22
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/