Regional Anaesthesia

KEY POINTS
- Pain following shoulder surgery remains challenging in the perioperative period.
- The shoulder block consists of a combined suprascapular and axillary nerve block.
- The shoulder block offers an alternative analgesic option for shoulder surgery, particularly in patients who refuse or in whom interscalene blocks are contraindicated.
- There is a lower risk of complications compared with the interscalene block, with several advantages and high patient satisfaction.
ANATOMY
The skin over the shoulder receives innervation from branches of the cervical and brachial plexuses. The shoulder joint is innervated by several peripheral branches of the brachial plexus (Table 1).
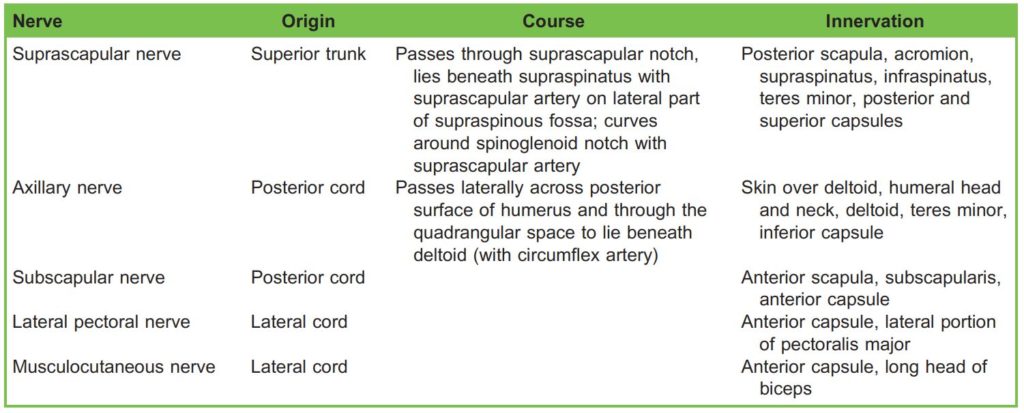
Table 1. The Innervation of the Shoulder Joint. The Suprascapular and Axillary Nerves are Responsible for the Majority of the Supply to the Shoulder Joint Whilst the Other Nerves Have Relatively Minor Contributions
INDICATIONS
Arthroscopic Procedures
There is increasing evidence supporting the use of the CSANB for arthroscopic surgical procedures.3
Open Procedures
There is sparse evidence at present comparing ISBs and CSANBs in open shoulder procedures. However, there are patients that refuse an ISB or may be unsuitable for an ISB (patients with respiratory compromise, eg chronic obstructive pulmonary disease) who may benefit from the opioid-sparing effect of regional anaesthesia.1,4 The analgesia options should be made available and the decision should be made tailored to individual needs.
Chronic Shoulder Pain
Suprascapular nerve blocks are commonly used in chronic pain5 and the CSANB may be used to improve chronic shoulder pain management.
BLOCK TECHNIQUE
Prior to performing any block, it is vital to ensure the following practices are followed:
- Obtain informed consent from the patient.
- Establish intravenous access and attach appropriate monitoring (electrocardiogram, noninvasive blood pressure monitoring, and pulse oximeter).
- Confirm the correct side of block (stop before you block).6
- Ensure appropriate aseptic precautions (eg 0.5% chlorhexidine gluconate and 70% denatured ethanol, sterile gloves, and sterile probe cover).
Consent involves describing the block (including sedation if required), positioning, the intended benefits, risks (see below) and alternatives. Specific to this block, patients are also informed that there may be some pain in the recovery room initially (due to swelling of the anterior capsule) which will subside with time (absorption of fluid into the joint) and requires systemic multimodal analgesia.
Suprascapular Nerve Block
Equipment
- Ultrasound machine with a high-frequency linear or curvilinear probe (and probe cover)
- 15-20 mL of local anaesthetic (LA) of choice (bupivacaine, ropivacaine) for the injection ensuring a safe, nontoxic dose (< 2mg/kg)
- 50- to 100-mm needle
- Sterile tray with gloves and skin prep
- Lidocaine for skin infiltration
Position
- Ideally, the operator is positioned behind the patient with the ultrasound positioned in front of the patient (Figure 1).
- The suprascapular nerve block can be easier to perform with the patient sitting.
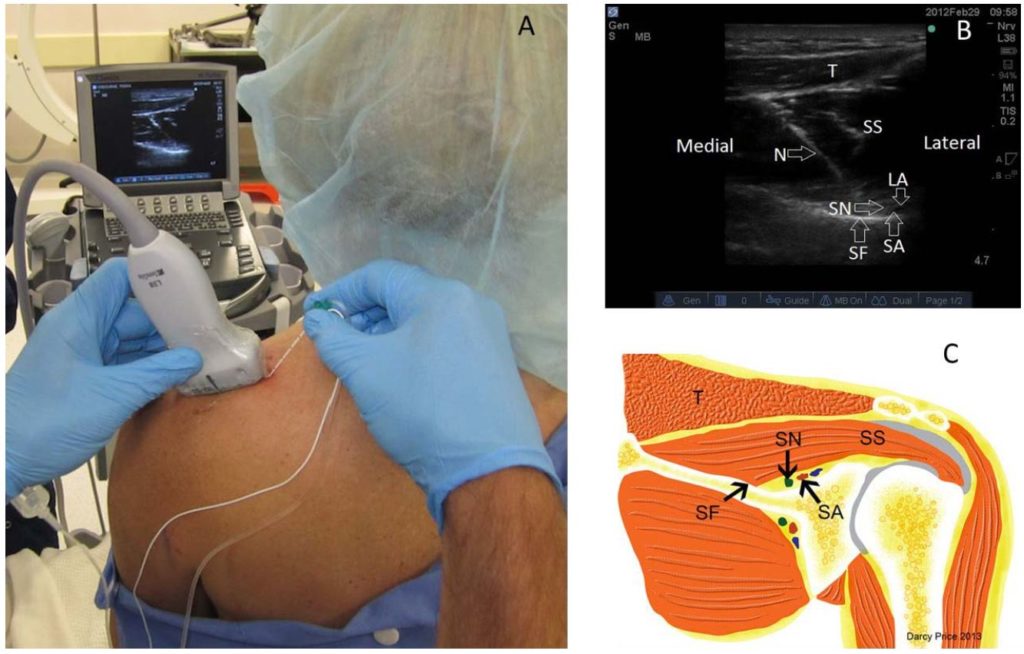
Figure 1. Performing the suprascapular nerve block.3,7 (A) Positioning of the patient and probe for visualising the supraspinous fossa. (B) Sonography of supraspinous fossa, showing the needle passing through trapezius and supraspinatus and injecting local anaesthetic into the floor, adjacent to the suprascapular artery and suprascapular nerve. (C) Relevant anatomy. SF indicates supraspinous fossa; SS, supraspinatus; T, trapezius; SN, suprascapular nerve; SA, suprascapular artery; N, needle; LA. Image supplied by D.P.
Performing the Block
With the patient sitting, the ultrasound probe is applied in the long axis parallel to the spine of the scapula, the supraspinous fossa can be visualised with its characteristic ‘hockey stick’ appearance, containing the supraspinatus overlying the neurovascular bundle of the suprascapular artery and suprascapular nerve (Figure 1).
Injection of LA fills the potential space and appears to lift supraspinatus up. In some cases, if the neurovascular bundle is not visible the needle can still be directed towards the floor of the fossa and withdrawn slightly once bony contact is made. Once negative aspiration for blood is confirmed, injection of LA will fill the space and cause supraspinatus to lift up.
Other approaches have also been described where the suprascapular nerve can be blocked in the supraclavicular region as the nerve passes below the omohyoid muscle.8
Axillary Nerve Block
Equipment
- Ultrasound machine with a high frequency linear/curvilinear probe (and probe cover)
- 5–7 mL7,9 of LA of choice (bupivacaine, ropivacaine) for the injection ensuring a safe, nontoxic dose (< 2 mg/kg)
- 50- to 100-mm needle
- Sterile tray with gloves and skin prep
- Lidocaine for skin infiltration
Position
- Ideally the operator is positioned behind the patient with the ultrasound positioned in front of the patient (Figure 2).
- The axillary nerve (AN) block can be easier to perform with the patient sitting or lateral. (D.P. recommends lateral positioning as a personal preference.)
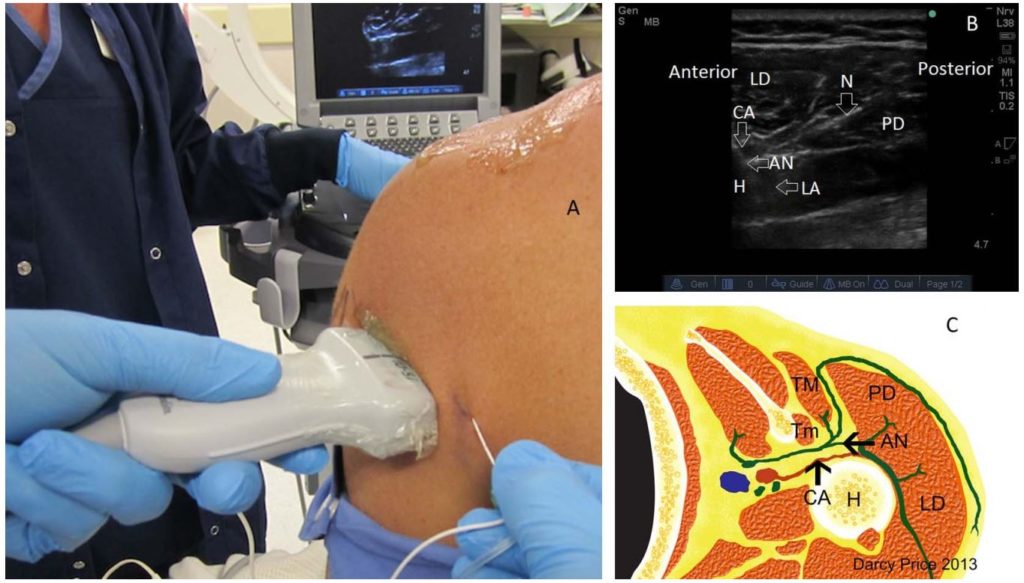
Figure 2. Performing the axillary nerve block.3,7 (A) Positioning of the patient and probe for visualising the posterior surface of the humerus. (B) Short-axis sonography view of axillary nerve block, showing the needle passing between lateral deltoid and posterior deltoid towards the humerus and deposition of local anaesthetic around the axillary nerve and circumflex artery. (C) Relevant cross-sectional anatomy including teres major and teres minor. AN indicates axillary nerve; N, needle; LD, lateral deltoid; PD, posterior deltoid; H, humerus; LA, local anaesthetic; CA, circumflex artery; TM, teres major; Tm, teres minor. Image supplied by D.P.
The probe is placed on the posterior surface of the humerus, proximal to the axillary crease (where the latissimus dorsi and deltoid meet) to visualise the neurovascular bundle (consisting of the AN and circumflex artery. The bundle may be visualised in the short- and long-axis planes (Figures 2 and 3).
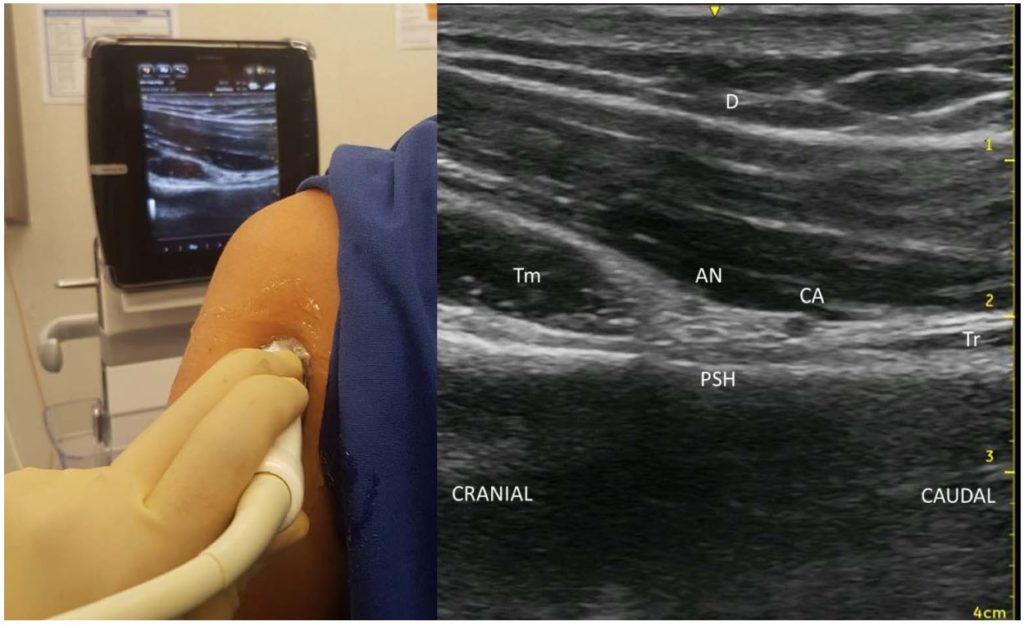
Figure 3. The axillary nerve. Long-axis view showing the position of the probe and the image generated. The axillary nerve and circumflex artery lie between the deltoid, triceps, and teres minor along the posterior surface of the humerus. AN indicates axillary nerve; CA, circumflex artery; D, deltoid; Tr, triceps; Tm, teres minor; PSH, posterior surface of the humerus. Image supplied by B.S.
When scanning the posterior humerus in the short axis, the lateral and posterior deltoid muscles create a ‘donut sign’ where the circumflex artery is easily identified beneath the posterior deltoid (Figure 2). The needle is passed in-plane through the posterior deltoid, directed anteriorly, and aiming for the posterior surface (rather than lateral) to allow a better spread of LA medially towards the posterior cord to cover more branches.
Performing the Block
Five to seven milliters of LA is normally injected and should fill the potential space beneath the posterior deltoid (large volumes associated with more proximal spread resulting in radial nerve block (Figure 4).7,9
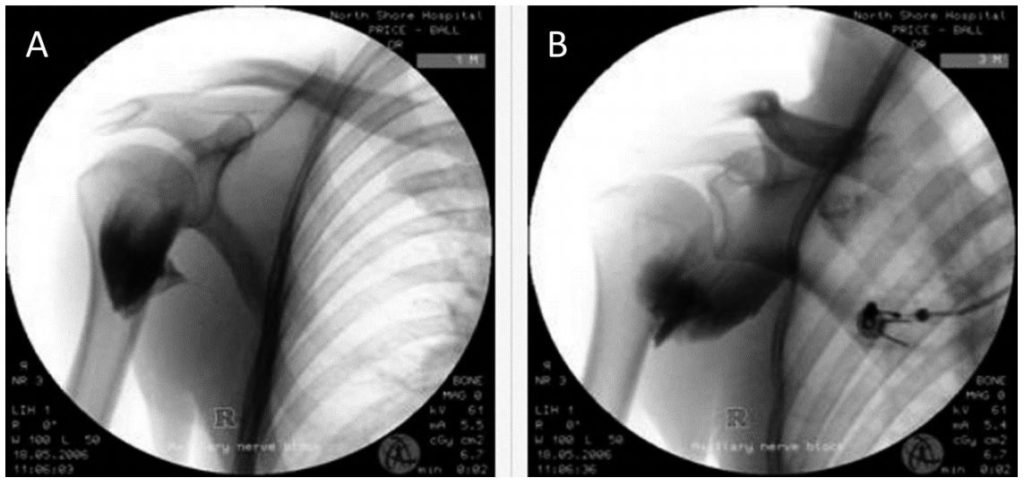
Figure 4. Fluoroscopy showing spread of 15 mL local anaesthetic after axillary nerve injection. (A) Immediate injection fills the potential space beneath posterior deltoid. (B) Spread of injectate seconds later showing proximal spread through quadrangular space. Image supplied by D.P.
Whilst an ISB may be used with sedation for surgical procedures, the CSANB provides analgesia and not anaesthesia and is therefore recommended to be used only in conjunction with general anaesthesia.
Catheter techniques may benefit some groups of patients and can be placed for the suprascapular nerve but may lie within the surgical field for the AN.
COMPLICATIONS
- The usual risks of any block apply including LA toxicity or allergy, nerve injury, bleeding, infection, and intravascular injection.
- Cases of radial nerve palsy were reported during the first few AN injections when 15 mL of LA was injected, leading to more proximal spread and involvement of the radial nerve.3
- Specific to the block, there are very few complications reported so far.7
- Ultrasound-guided blocks are likely to be more accurate than landmark techniques.10
COMPARISON TO ISB
Compared to ISB, the CSANB offers the following:
- Peripheral nerve blockade (rather than central) reducing the risk of damage to nerves11) and deeper structures
- Sparing of phrenic nerve blockade (phrenic nerve almost certainly blocked with ISB with almost 50% describing the hemidiaphragmatic paralysis as uncomfortable7; less arm paraesthesia and is generally well tolerated (almost 50% of patients report dissatisfaction with ISB due to the sensation of a numb arm and motor discomfort)12,13
- Noninferior analgesia at rest and on movement with reduced opioid consumption from 6-24 hours7
- Reduced rebound pain13
- Reduced postoperative nausea and vomiting 14
- Satisfaction score similar to ISB14
- Lower pain scores with CSANB with fewer fluctuations than ISB at 6-8 hours16
There are some limitations to the CSANB (compared to ISB):
- Increased pain in the immediate postoperative phase up to 6 hours (which can possibly increase opioid consumption as the lateral pectoral, subscapular, and musculocutaneous nerves are not blocked)15
- There is no evidence to support use of CSANB over ISB in open and major arthroscopic procedures (however, a CSANB can act as an alternative in patients where an ISB is contraindicated or refused). Furthermore, anterior shoulder pain is not effectively blocked by the CSANB and further research is required to develop this aspect for this block.
At present, there is increasing evidence supporting the use of CSANBs in arthroscopic surgery with overall equivalent analgesia and without some of the undesired effects of the ISB. The CSANB is an analgesic block used in conjunction with general anaesthesia (and systemic analgesia in early stages of recovery); however, the analgesic benefits become obvious after 6 hours and have fewer undesirable effects (compared to ISB). There are some further areas of development, including the following:
- CSANB should be compared with ISB for open shoulder surgery.
- Rotator cuff surgery involving the subscapularis may require subscapularis nerve blockade.
SUMMARY
- The CSANB is a simple, low-risk block combination that can be performed in the awake patient.
- The CSANB can be used for arthroscopic procedures, rescue techniques, chronic shoulder pain management, and open techniques when an ISB is contraindicated or refused.
- Good intraoperative pain management is required and the benefits of the CSANB are seen in the postoperative period.
ACKNOWLEDGEMENTS
This article is dedicated to Dr Darcy Price (1966-2018), a highly respected and much-admired anaesthetist, dedicated teacher, and regional anaesthesia enthusiast. He was instrumental in developing, researching, and educating our specialty as to the benefits of the combined suprascapular and axillary nerve block as an alternative to the interscalene block for shoulder anaesthesia. A pioneer, but also humble, he simply named this technique the ‘Shoulder Block’; in Auckland, New Zealand, it is known more appropriately as the ‘Darcy Block’.
He was an inspiration to many and each of us has a special memory of him. He was an esteemed colleague and loyal friend; a kind, humble, and considerate gentleman with an engaging sense of humour who will be greatly missed.
REFERENCES
- Bowens C, Sripada R. Regional blockade of the shoulder: approaches and outcomes. Anesthesiol Res Pract. 2012;2012(4):1-12.
- Borgeat A, Ekatodramis G, Kalbere F, Benz C. Acute and nonacute complications associated with interscalene block and shoulder surgery: a prospective study. Anesthesiology. 2001; Vol 95, 875-880.
- Price DJ. The shoulder block: a new alternative to interscalene brachial plexus blockade for the control of postoperative shoulder pain. Anaesth Intensive Care. 2007 Aug;35(4):575-581.
- Verelst P, van Zundert A. Respiratory impact of analgesic strategies for shoulder surgery. Reg Anesth Pain Med. 2013;38:50-53.
- Shanahan EM, Ahern M, Smith M, et al, Suprascapular nerve block (using bupivacaine and methylprednisolone acetate) in chronic shoulder pain. Ann Rheum Dis. 2003;62:400-406.
- Regional Anaesthesia UK. Stop before you block Accessed September, 2020. https://www.ra-uk.org/index.php/stopbefore-you-block.
- Price D, Abeysekera A, Chaddock M. A randomised comparison of combined suprascapular and axillary (circumflex) nerve block with interscalene block for postoperative analgesia following arthroscopic shoulder surgery. Anaesth Intensive Care. 2012;40(1):183-184.
- Siegenthaler A, Moriggl B, Mlekusch S. Ultrasound-guided suprascapular nerve block, description of a novel supraclavicular approach. Reg Anesth Pain Med. 2012;37:325-328.
- Checcucci G, Allegra A, Bigazzi P, et al. A new technique for regional anesthesia for arthroscopic shoulder surgery based on a suprascapular nerve block and an axillary nerve block: an evaluation of the first results. Arthroscopy. 2008;24:689-696.
- Lancaster S, Clark D, Redpath Y, et al. Blockade of the suprascapular nerve: a radiological and cadaveric study comparing landmark and ultrasound-guided blocking techniques. 2013. Shoulder Elbow. 5(3):173-177.
- Quinn H. Hogan; Phrenic nerve function after interscalene block revisited: now, the long view. Anesthesiology. 2013;119(2):250-252. doi:10.1097/ALN.0b013e31829c2f3a
- Pitombo PF, Barros RM, Matos MA, Mo´ dolo NSueliP. Selective suprascapular and axillary nerve block provides adequate analgesia and minimal motor block: comparison with interscalene block. Revista Brasileira Anestesiol. 2013;63(1):52-58.
- Lee JJ, Yoo YS, Hwang JT, et al. Efficacy of direct arthroscopy-guided suprascapular nerve block after arthroscopic rotator cuff repair: a prospective randomized study. Knee Surg Sports Traumatol Arthrosc. 2015;23(2):562-566.
- Dhir S, Sondekoppam RV, Sharma R et al. A comparison of combined suprascapular and axillary nerve blocks to interscalene nerve block for analgesia in arthroscopic shoulder surgery: an equivalence study. Reg Anesth Pain Med. 2016;41(5):564-571.
- Hussain N, Goldar G, Ragina N, et al. Suprascapular and interscalene nerve block for shoulder surgery: a systematic review and meta-analysis. Anesthesiology. 2017;127(6):998-1013.
- Abdallah FW, Halpern SH, Aoyama K, et al. Will the real benefits of single-shot interscalene block please stand up? A systematic review and meta-analysis. Anesth Analg. 2015;120(5):1114-1129.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/