General Topics

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Which of the following statements are correct?
- Female patients should consider stopping oestrogen containing contraceptives 4 weeks before elective surgery.
- Regional anaesthesia (compared to general anaesthesia) reduces the risk of a thrombus by 35%.
- The half-life of protamine is 60-90 minutes.
- Anti-platelet medications are adequate prophylaxis in low-risk surgical patients.
- Which clotting factors does warfarin interfere with?
- Which of the following are risk factors for bleeding or complications due to bleeding in surgical patients?
- Central neuraxial blockade expected within the next 12 hours.
- Acute liver failure.
- Central neuraxial blockade within the previous 4 hours.
- Uncontrolled systolic hypertension >200mmHg.
INTRODUCTION
Thromboprophylaxis: Part One, discussed clot development,‘at risk’ groups, diagnosis, investigation and treatment of surgical patients with a suspected venous thromboembolism. In this follow on tutorial the options for prophylaxis against venous thromboembolism (VTE) in the surgical population will be reviewed and evidence based VTE prophylaxis guidelines will be examined. Thromboprophylaxis in special groups, such as pregnant women and patients with renal failure will also be considered.
THROMBOPROPHYLAXIS: THE OPTIONS
Following careful assessment of a patient’s VTE risk as described in tutorial one, the most suitable method of thromboprophylaxis should be selected. Options include:
- Simple precautionary advice and education
- Mechanical thromboprophylaxis
- Pharmacological thromboprophylaxis
- Vena cava filters
Simple precautionary advice and education
Not all patients require prophylactic therapy, whether it be pharmacological or mechanical, however all will benefit from education on ways they can limit their risk.
The contraceptive pill
Preoperatively female patients should consider stopping oestrogen containing oral contraceptives four weeks before elective surgery however, this must be accompanied by appropriate advice on alternative methods of contraception. It is unlikely that a patient would wish to stop hormone replacement therapy prior to elective surgery, but in the high risk population this should be discussed as an option1.
Antiplatelet drugs.
If a patient is already on antiplatelet medication serious consideration of the risks associated with stopping the drugs compared to the risk of surgical bleeding must be undertaken. This may involve other specialists, including a cardiologist, as well as the surgeon conducting the procedure.
Hydration
Patients should not be allowed to become dehydrated, especially during a prolonged “Nil by Mouth” period perioperatively. Oral fluids should be encouraged or intravenous fluids should be prescribed.
Regional anaesthesia
The anaesthetist should consider the possibility of a regional technique for high risk patients as this can reduce the risk of a thrombus by about 50% as compared to general anesthesia2. Consideration of the timing of pharmacotherapy pre and post operatively must be included in the anaesthetic plan to avoid increasing the risk of an epidural or spinal haematoma.
Early mobilisation
Mobilisation should be as prompt as possible post-operatively with appropriate aids and advice from a physiotherapist. Simple movements in bed can also be undertaken by those that are unable to walk or sit1.
Mechanical thromboprophylaxis
Mechanical compression methods reduced the risk of venous thrombosis by about two-thirds when used as monotherapy, and by about half when added to a pharmacological method2. Methods of reducing the incidence of VTE include: anti-embolism stockings, intermittent pneumatic compression devices and foot impulse devices. Each of these therapies are equally efficacious at reducing VTE.
Anti-embolism stockings
These stockings provide a graduated compression to produce a calf pressure of 15mmHg to prevent venous pooling. Correct sizing of stockings is important as a poor fit can increase thromboembolic risk. Stockings must remain on, day and night, until normal mobilisation is resumed. Daily review of skin integrity and pressure areas must be undertaken.
Anti-embolism stockings should not be worn in the following circumstances: peripheral arterial disease or bypass grafting, peripheral neuropathy, dermatitis, gangrene, recent skin graft, severe leg oedema secondary to congestive heart failure, major limb deformity preventing a correct fit. Venous leg ulcers present a relative contra-indication.
Intermittent pneumatic compression and foot impulse devices
These devices mimic the normal venous calf pump, reducing venous stasis. The patient should be encouraged to keep them on whenever they are in bed or sitting in a chair. Contra-indications are fewer than with the use of stockings but each patient must be assessed for their suitability, and the integrity of the skin beneath the pump should be regularly reviewed.
Vena Cava filters
In patients at high risk of VTE, especially those with cancer, in whom mechanical or pharmacological thromboprophylaxis is not possible, the insertion of a temporary or permanent vena caval filter preoperatively, should be considered.
PHARMACOLOGICAL THROMBOPROPHYLAXIS
Historically, pharmacotherapy for the surgical inpatient has been almost exclusively with unfractionated or low molecular weight heparins. In the last few years a plethora of alternative pharmacological strategies for thromboprophylaxis have become available. The following section summarises these new treatments accompanied by advice from the American College of Chest Physicians3 regarding the agents of choice, given the current evidence base.
Indirect thrombin and factor X inhibitors
Indirect thrombin inhibitors act on antithrombin or coagulation factor X to inhibit the effect of factor IIa, thrombin. Thrombin is responsible for the conversion of fibrinogen to fibrin and the consequential formation of a fibrin plug, and the activation of platelets via protein C. Positive feedback via coagulation factors V and VIII further increases thrombin production.
Unfractionated Heparin
Heparin was first discovered by a medical student from Johns Hopkins University. The name heparin comes from the Greek “hepar”, meaning liver as the molecule was originally derived from canine liver cells. These acidic glycosaminoglycans are found in human liver, lung, mast cells and basophils. The polymers are negatively charged and have molecular weights varying from 3 to 30 kDa. Only around one third of the heterogenous chains contribute to the majority of the anticoagulant activity due to the presence of a specific pentasaccaride sequence.
Unfractionated heparin (UFH) binds to antithrombin (AT), converting it from a slow inhibitor of thrombin to a fast inhibitor. Antithrombin covalently binds to the active centre of thrombin but also interacts with other coagulation factors (Xa, IXa, XIa and XIIa) to produce its anticoagulant effects. Factor Xa produces its anticoagulant effect by cleaving prothrombin to form thrombin. Although factor Xa is also inhibited by AT, the inhibition of thrombin is 10 times greater. The resultant effect of UFH is prevention of fibrin production, activation of platelets and formation of a clot.
Heparin dosage is measured in units; one unit is the quantity of heparin required to keep 1ml of cats’ blood fluid for 24 hours at zero degrees Celsius. UFH is not absorbed orally and must be administered as an intravenous infusion or subcutaneous bolus. Once in plasma, heparin binds to plasma proteins, endothelial cells and macrophages. Clearance is non-linear, depending on a rapid, saturatable mechanism and slower renal clearance. Due to the variable binding and clearance of UFH, monitoring is required. Initial dosage is dependent on patient weight and thereafter adjusted depending on the activated partial thromboplastin time (APTT). An APTT ratio of 1.5-2.5 is often used as a target therapeutic window for patients receiving UFH for VTE prophylaxis although this target was in response to a retrospective study carried out in the 1970s. Various reagents and coagulometers are used to derive the APTT and each has its own nomogram for dose adjustment to maintain the target range. Assays of the ability of heparin to inhibit coagulation factor Xa (anti-Xa) are also available for monitoring UFH as well as other anticoagulants. A proportion of patients appear to be relatively resistant to UFH and require significantly higher dosing strategies. AT deficiency, increased clearance and elevated levels of factor VIII have all been put forward as possible explanations for this phenomenon.
One of the unique advantages of UFH is the availability of an agent to reliably reverse it’s effects; protamine sulphate. This basic protein has a half-life of 7 minutes, compared to that of UFH which is 60-90 minutes. It is for this reason that when calculating the dose of protamine sulphate, the total dose of heparin given in the preceding hour, must be taken in to account. 1mg of protamine sulphate will reverse 100u of UFH. Adverse reactions to protamine sulphate, including hypotension and bradycardia, can be reduced by slow administration. Due to its derivation from fish sperm, anaphylaxis is possible in patients who have a sensitivity to fish, or have had a previous vasectomy.
Complications associated with UFH include haemorrhage, osteoporosis, alopecia, hypersensitivity, elevation of serum transaminases and heparin induced thrombocytopenia (HIT). HIT appears to be caused by heparin-dependent antibodies that bind to platelet factor IV and the surface of the platelet itself. The consequence of platelet activation and removal from the circulation results in a reduced platelet count, but counter-intuitively, the activated platelets provide a substrate for factor II activation and clot formation, producing microthrombi and arterial or venous thrombosis. Platelets should be monitored intermittently until day 14 of administration6 (see ATOTW 243 & 245 for more about HIT).
Low Molecular Weight Heparins
Only polymers of sufficient length can inhibit thrombin via AT, however, smaller chains can still act on AT to cause inhibition of factor Xa. Low molecular weight heparins (LMWH) are derived from UFH by chemical or enzymatic depolymerisation to produce chains with molecular weights ranging from 2-9kDa. The shorter chains have reduced binding to plasma proteins, producing predictable doseresponse relationships and less endothelial cell binding thus extending the plasma half-life. Binding to platelet factor IV is also reduced, although not completely, so HIT is less frequent but still possible.
LMWH is given via the subcutaneous route and dosage is calculated from the patient’s weight. Routine monitoring is not necessary. In Europe a once daily dosing strategy is used for VTE prophylaxis (for example 40mg enoxaparin daily) however, in North America a twice daily regime is used (for example 30mg enoxaparin twelve hourly). This differing dosing strategy does alter the protection against VTE and bleeding risk. When comparing LMWH to newer anticoagulants it is important to know which dosing strategy the trials used as the comparator.
Clearance of LMWH is via the kidneys and the effects are prolonged in patients with renal failure. It may be wise to carry out monitoring with anti-Xa assays in obese patients, pregnant women and patients with renal failure.
Although there is no reliable method of reversing LMWH, protamine sulphate does have some effect, although it can not completely halt the anticoagulant process. Current recommendations suggests that if LMWH was given within 8 hours then protamine sulphate should be administered at a dose of 1mg for every 100U of anti-Xa activity (1mg enoxaparin = 100U anti-Xa activity). If bleeding continues then half the original dose should be given again. If the time since administration is greater than 8 hours then a reduced dose should be administered. If available, recombinant coagulation factor VIIa may also be effective in patients treated with LMWH.
Fondaparinux Sodium
This is the synthetic analogue of the pentasaccaride fragment of heparin responsible for binding AT. By modifying the structure, the affinity of fondaparinux sodium for AT is increased, thus increasing the half-life and specific activity. Fondaparinux sodium has a molecular weight of 1.7kDa and is more specific for inhibition of factor Xa than the LMWH, with no effect on thrombin inhibition.
Absorption is via the subcutaneous route and half-life is around 17 hours. A fixed dosing regime for VTE prophylaxis of 2.5mg once daily is not adjusted for body weight. No monitoring is advised although fondaparinux sodium can be monitored with an anti-Xa assay. It is contraindicated in patients with a creatinine clearance of less than 30ml/min as it is excreted unchanged in the urine. No reports of HIT have been made at present.
Fondaparinux can not be reversed with protamine sulphate, but as with LMWH, recombinant factor VIIa may be effective.
Danaparoid
A mixture of glycosaminoglycans, danaparoid is chemically distinct from heparin. It is an inhibitor of factor Xa via activation of AT. With a half-life of 25 hours it is longer acting than the LMWHs. Due to its dissimilarity to heparin, its use is largely limited to management of patients with HIT.
Direct thrombin inhibitors
Hirudins (lepirudin and desrudin)
Originally isolated from the salivary gland of the leech, hirudin is now available in recombinant forms. The terminal ends of the polypeptide produce irreversible complexes with thrombin, inhibiting its activity. Administration is via the subcutaneous route and dosage is independent of weight. Given in a twice daily regime the hirudins are excreted renally and contraindicated in patients with renal failure. Lepirudin is licensed for the treatment of thrombosis in HIT in North America and desrudin is approved in Europe for VTE prophylaxis after hip replacement.
Argatroban
This competitive thrombin inhibitor forms a reversible complex with thrombin. Administered via the intravenous route and excreted hepaticaly, it has a place in the treatment of patients with renal failure or HIT. Argatroban is monitored using the APTT ratio.
Dabigatran etexilate
This is a competitive, reversible, non-peptide antagonist of factor IIa. It is a prodrug that can be administered orally. Dosing is independent of weight and fixed according to indication. Bioavailability is only 6.5% but the dabigatran etexilate is rapidly metabolised to dabigatran, the active metabolite. Duration of action is 24-36 hours and although proton pump inhibitors may reduce absorption, there are minimal drug interactions. Excretion is renal and it is therefore contraindicated in patients with renal failure. No data on safety in pregnancy means that it is contraindicated in this population. Reversal of direct thrombin inhibitors is not possible but recombinant factor VIIa may be of use and special dialysis membranes can remove hirudin.
Direct factor Xa inhibitors
Rivaroxaban
A new inhibitor of coagulation factor Xa, rivaroxaban is an oxazolidone derivative that can be taken orally. It’s a highly selective, competitive, reversible antagonist of factor Xa with a bioavailability of 80%. VTE prophylaxis with rivaroxaban compares favourably with both the North American and European LMWH dosing strategies.4 With a duration of action of 24 hours, a once daily dosing strategy is used and there is no need for monitoring of effect. Metabolism is via the hepatic P450 system and potent inhibitors (ketonazole, clarithromycin) may augment the anticoagulant effect. Unfortunately no reversal agent is available for rivaroxaban and it is contraindicated in patients with renal failure and pregnancy.
Apixaban
Another oral factor Xa inhibitor, apixaban has been evaluated against enoxaparin in the ADVANCE trials. In ADVANCE 25 apixaban compared well against the European enoxaparin dosing regime in patients undergoing elective knee replacement. In ADVANCE 1 however, apixaban failed to show a benefit over the North American enoxaparin regime in terms of reducing VTE, although bleeding risk was reduced.
Vitamin K antagonists (warfarin, acenocoumarol, phenprocoumon)
Vitamin K antagonists have been the cornerstone of oral anticoagulation for many years and their effectiveness has been established in many different population groups. Use in the preoperative period is largely limited to long term anticoagulation due to their onset of action; 36-72 hours. For this reason they will not be discussed at length in this tutorial.
The vitamin K antagonists (VKA) produce their effect by interfering with the interconversion of vitamin K and vitamin K epoxide in the liver. The carboxylation of coagulation factors II, VII, IX and X is prevented and in this way, coagulation is impaired. Other proteins are also dependent on vitamin K carboxylation, especially those involved in bone growth, leading to foetal bone abnormalities if women receive VKA during pregnancy.
The most common VKA, warfarin, has a high oral bioavailability and circulates bound to plasma proteins. Hepaticaly metabolised by the P450 system, there is considerable interaction with many drugs. The pharmacokinetics of warfarin are highly variable and it is for this reason that patients who receive VKAs must be regularly monitored. Monitoring is via the prothrombin time and international normalised ratio (INR). Although a target INR of 1.5-2 has been shown to reduce the recurrence of VTE as compared to placebo, a higher INR 2-3 appears to be more effective, but carries a higher risk of bleeding. Reversal of VKAs can be with vitamin K orally or intravenously, fresh frozen plasma, prothrombin complex concentrates or recombinant factor VIIa depending on the urgency and availability of agents.
Antiplatelet agents
At present, antiplatelet medications should not be considered sufficient anticoagulation for VTE prophylaxis. However, there are new antiplatelet agents in trial which may, in the future, be considered adequate.
Dextrans
Dextran is a polysaccharide that binds to red blood cells and platelets, reducing their cohesion. They need to be administered in large volumes and although they do reduce the incidence of DVT, they are less effective than other pharmacological treatments. Consequently they are no longer recommended6.
WHO SHOULD RECEIVE THROMBOPROPHYLAXIS?
On admission to hospital, every patient should have their risk of VTE assessed. The risk factors for VTE have been discussed previously in Thromboprophylaxis Part 1, and are summarised in figure 1. Risk factors for bleeding are summarized in figure 2.
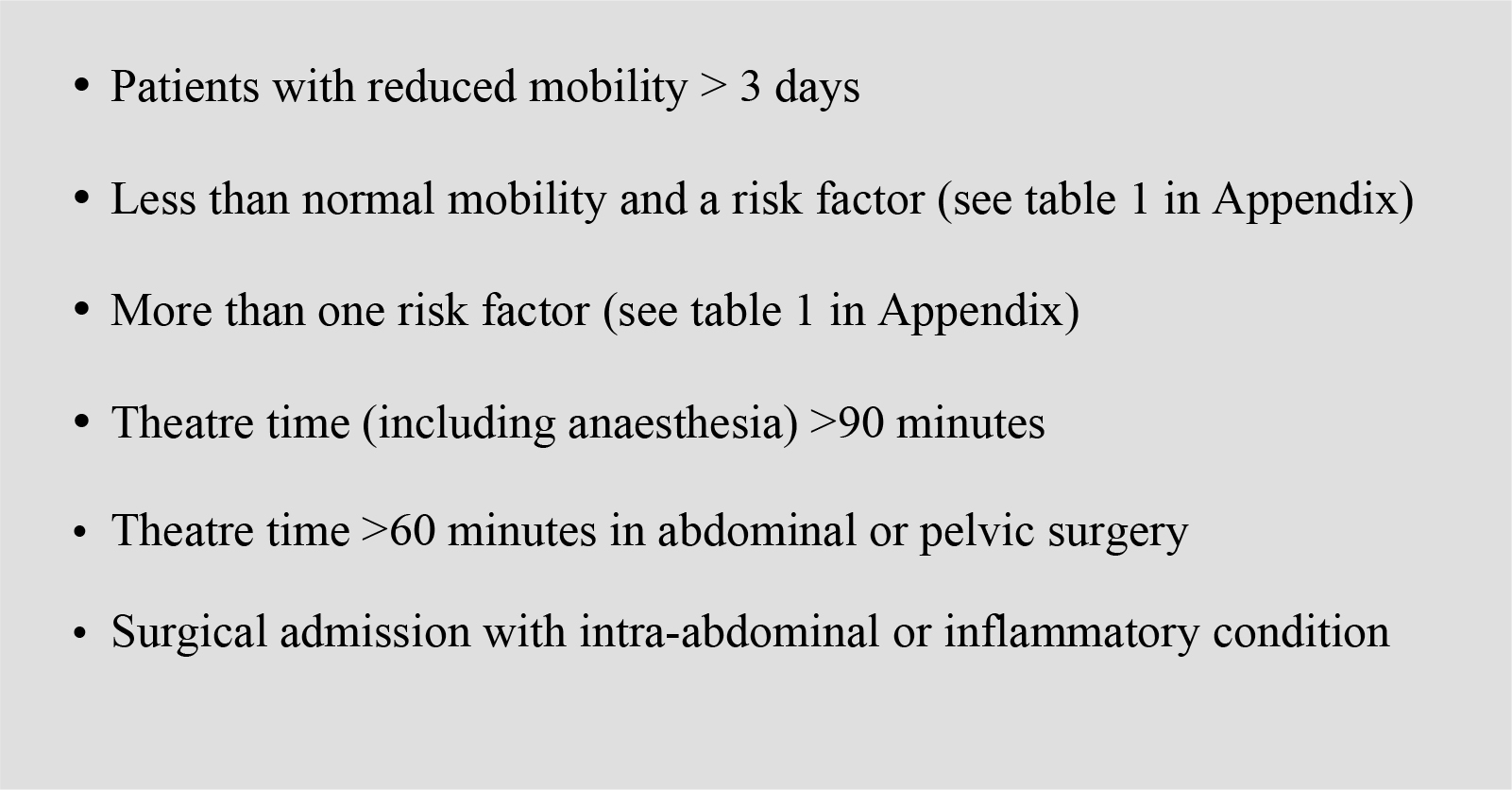
Figure 1: Surgical patients at increased risk of VTE
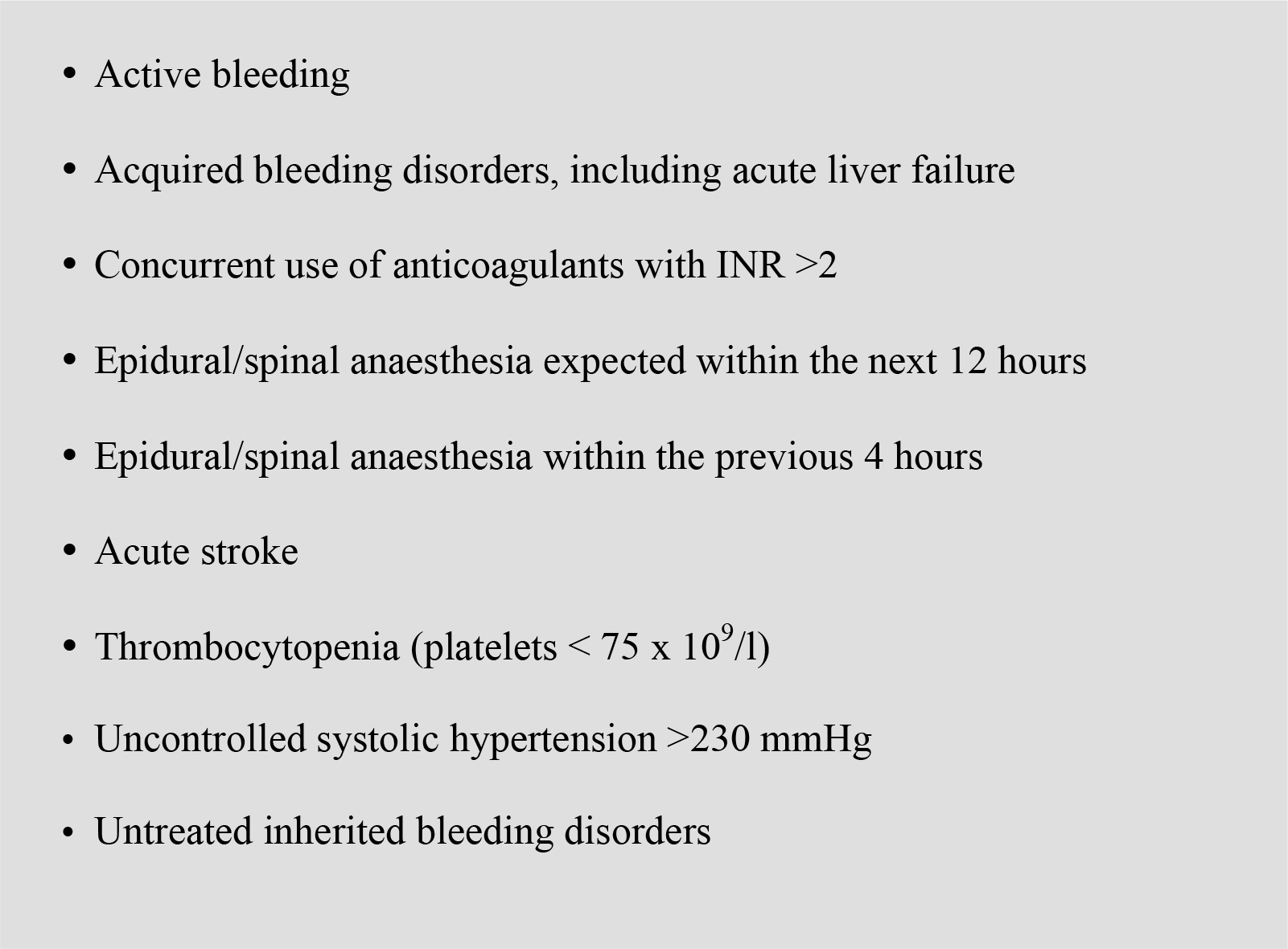
Figure 2: Surgical patients at increased risk of bleeding or complications due to bleeding
THROMBOPROPHYLAXIS GUIDELINES
The UK based National Institute for Clinical Excellence (NICE)1 has recently released guidelines on thromboprophylaxis and it is from these that the next section is derived.
General guidance
Any surgical patient that has been assessed as at increased risk of VTE should have mechanical VTE prophylaxis prescribed on admission, as long as there are no contraindications. If the risk of bleeding is low then pharmacological prophylaxis with LMWH or UFH in patients with renal failure, should be commenced 6-12 hours post operatively. These measures should be continued until there is no significant reduction in mobility. Elaborations and exceptions to this rule are now discussed.
Obese patients
For thromboprophylaxis in obese patients undergoing surgery, the minimal evidence suggests that weight based prophylactic dosing is preferable to fixed dosing. Factor Xa activity is inhibited appropriately when the drug is administered to obese patients in doses based on total body weight up to 144kg (enoxaparin), 165kg (tinzaparin) and 190Kg (dalteparin).
Fondaparinux may be used instead of LMWH or UFH post-operatively and there may be some benefit in extending the post-surgical treatment to up to 3 weeks.
Cancer patients
Pharmacotherapy should be extended to 28 days post-operatively in any patient who has had major cancer surgery in the abdomen or pelvis.
Neurosurgical and spinal surgery patients
Pharmacotherapy should not be offered to patients with ruptured cranial or spinal vascular malformations or acute traumatic or non-traumatic haemorrhage until the lesion has been secured or the patient is stable.
All patients having spinal surgery should have mechanical VTE prophylaxis post-operatively. The decision to use pharmacotherapy needs to be made on an individual patient basis depending on the balance of risk. Regular assessment of VTE and bleeding risks should be made and reviewed.
Orthopaedic patients
Elective hip and knee surgery
Patients undergoing elective hip or knee replacement surgery should have mechanical VTE prophylaxis on admission. If there are no contraindications then VTE prophylaxis should be commenced post operatively. Table 1 illustrates the agents recommended by NICE and the time they should be commenced after surgery. Pharmacotherapy should be continued for 28-35 days post surgery, depending on the agent chosen
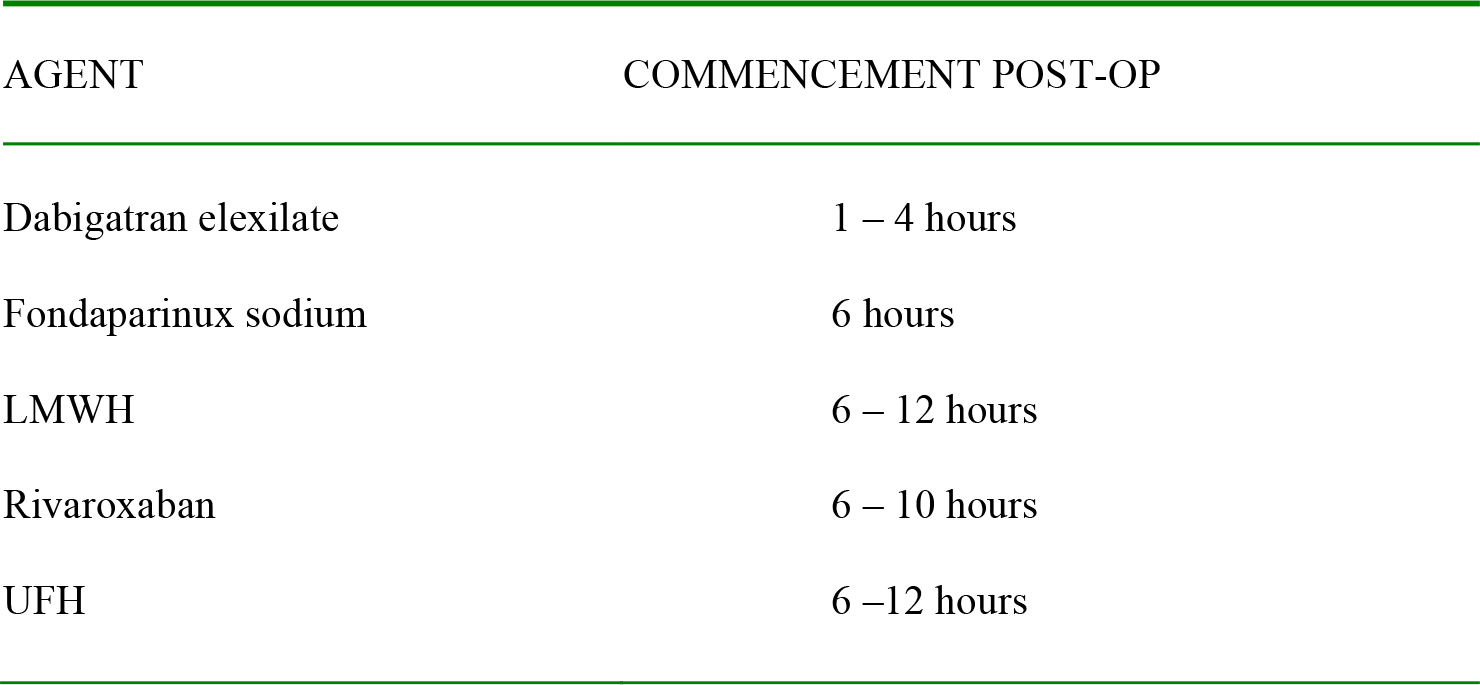
Table 1: Agents used in VTE prophylaxis after hip or knee surgery
Hip fracture
Patients undergoing surgery for hip fractures should have mechanical and pharmacological prophylaxis commenced on admission if there are no contraindications. Pharmacotherapy should be stopped 24 hours before surgery and recommenced after 6 – 12 hours post-operatively. Choice of agents include LMWH, fondaparinux sodium and UFH for patients with renal failure.
Upper limb surgery
VTE prophylaxis is not recommended routinely for patients undergoing upper limb surgery unless they are at increased risk.
Trauma patients
Assessment of risk of VTE versus risk of bleeding should be reviewed daily.
Critical care patients
This cohort of patients are at high risk of VTE, but a daily assessment of risk of VTE versus risk of bleeding should be undertaken.
Patients on anti-platelet medications
Anti-platelet medications should not be considered as adequate prophylaxis against VTE. Mechanical and pharmacological methods should be considered in relation to the risk of bleeding.
Renal Failure
Reduction in the factor Xa inhibitory effect of LMWH is highly correlated with creatinine clearance with the exception of tinzaparin. A decrease in LMWH clearance has been associated with an increased risk of bleeding in patients receiving treatment doses of LMWH for VTE but not in those receiving only prophylactic doses of LMWH.
Tinzaparin has a higher average molecular weight than the other LMWHs and this may result in partial hepatic clearance, accounting for the reduced correlation between creatinine clearance and anticoagulant effect.
Pregnancy
Pregnant women undergoing elective caesarian section who have one additional risk factor (not including pregnancy or caesarian section) should receive pharmacological thromboprophylaxis with LMWH or UFH, or mechanical prophylaxis post-operatively in hospital.
Pregnant women with more than one additional risk factor should receive both pharmacological and mechanical prophylaxis. Certain high risk patients with multiple risk factors should receive prophylaxis for 4 to 6 weeks after delivery. Informed consent should be granted by the mother before any pharmacological prophylaxis is started.
SUMMARY
In summary, if we are to reduce the incidence of VTE in the perioperative population, it is imperative that every patient is assessed for their risk at admission and this decision is regularly reviewed in light of any changes in their condition. After assessment, an individualised prophylactic regime incorporating the correct method or methods of prophylaxis, in the correct dosage, for the correct length of time, can be prescribed.
ANSWERS TO QUESTIONS
- T / F ( it’s about 50%) / F (7 minutes, heparin is 60-90 minutes) / F
- Factors II, VII, IX & X.
- A, B & C. Uncontrolled systolic hypertension >230 is a risk factor. See table for the complete set.
REFERENCES
- National Institute of Clinical Evidence. Venous thromboembolism: reducing the risk NICE guideline num 92 Jan. 2010
- Roderick P, Ferris G, Wilson K, Halls H, et al -Towards evidence-based guidelines for the prevention of venous thromboembolism: systematic reviews of mechanical methods, oral anticoagulation, dextran and regional anaesthesia as thromboprophylaxis. Health Technology Assessment, 2005 vol: 9, (49), 1-78.
- Hirsh j, Guyatt G, Albers GW, Harrington R, Schunemann HJ. Executive Summary: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) Chest 2008; 133;71S-109S
- Turpie AGG, Lassen MR, Davidson BL, Bauer KA et al – Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4) The Lancet 2009, Vol. 373, (9676) 1673 – 1680
- Lassen MR, Raskob GE, Gallus A, Pineo G et al – Apixaban versus enoxaparin for thromboprophylaxis after knee replacement (ADVANCE-2) The Lancet 2010 Vol. 375, (9717) 807-
- Barker RC, Marval P – Venous thromboembolism: risks and prevention Continuing Education in Anaesthesia, Critical Care & Pain 2011 Vol 1118-23
APPENDIX
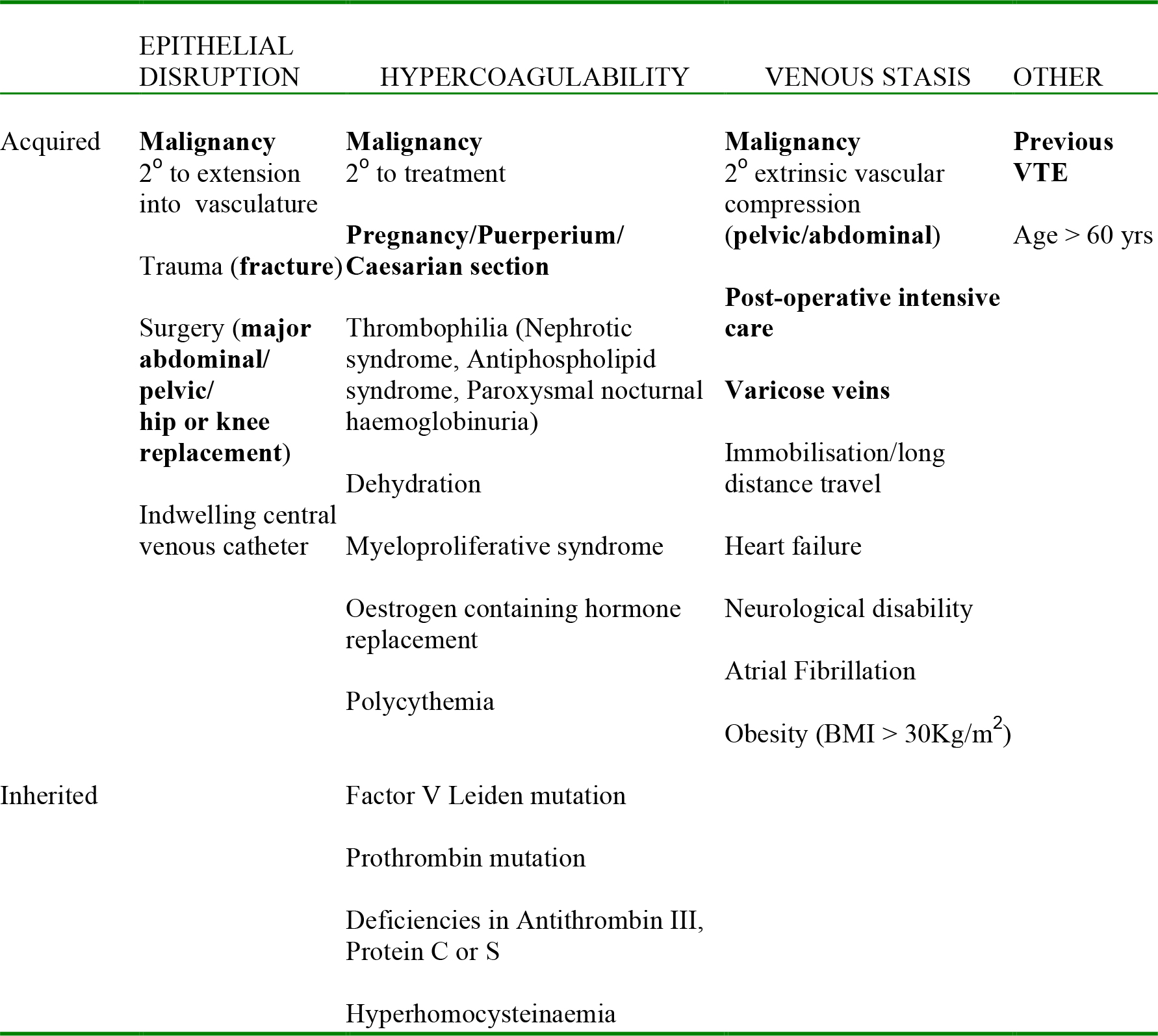
Risk factors for venous thromboembolism. British Thoracic Society1 major risk factors in bold.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/