Basic Sciences

KEY POINTS
- Tranexamic acid reduces bleeding and reduces the need for blood transfusion. It is used in the management of major trauma, haemorrhage, and as prophylaxis in surgery.
- Standard dose is 1g intravenously, over a minimum of 10 minutes.
- The main mechanism of action is anti-fibrinolytic activity. It also possesses anti-inflammatory effects and may help attenuate the systemic inflammatory response syndrome in cardiac patients.
- There has been no evidence of thrombotic events with tranexamic acid use, but theoretical concerns remain, and caution is advised in patients with recent or significant history of venous thromboembolism.
- In cardiac patients it has been shown to increase the risk of seizures, and manufacturers advise against using in any patient with a history of seizures.
INTRODUCTION
Tranexamic acid was introduced in the 1960s, it reduces bleeding by competitively inhibiting fibrinolysis. It was initially prescribed for heavy menstrual bleeding but is now recommended in a variety of elective surgical procedures to reduce blood loss, and also for the treatment of major haemorrhage. It has relatively few contraindications, is well-tolerated and cheap to use. As such, its use continues to expand into other specialties and surgeries.
The CRASH2 trial (2010) is the largest study to date on tranexamic acid demonstrating a significant (1.5%) mortality benefit when 1g of intravenous tranexamic acid, compared to placebo, was given within 3 hours of injury to trauma patients with suspected major haemorrhage1. In the WOMAN trial (2017) 1g of intravenous tranexamic acid was given for the treatment of post-partum haemorrhage resulting in reduced deaths due to bleeding (0.4%), with a greater survival benefit when tranexamic acid is given as close as possible to the onset of post-partum haemorrhage2. The ATACAS trial (2018) studied the effect of tranexamic acid in cardiac surgery and, consistent with the effect seen in other surgical specialties, blood loss was reduced. Relatively high doses (50-100mg/kg) were administered and post-operative seizure rate was increased with tranexamic acid compared to placebo3. Some evidence links higher doses with larger reductions in peri-operative blood loss but at the expense of increased seizure rate. Tranexamic acid is also commonly used in orthopaedic surgeries as a 1g prophylactic pre-incision dose in total knee and total hip arthroplasty4. Research into its benefits in spinal surgery, intra-cranial haemorrhage, liver resection and paediatrics is ongoing.
After reviewing the pharmacology, contraindications and side effects, this article will consider the use of tranexamic acid in clinical practice across various specialties.
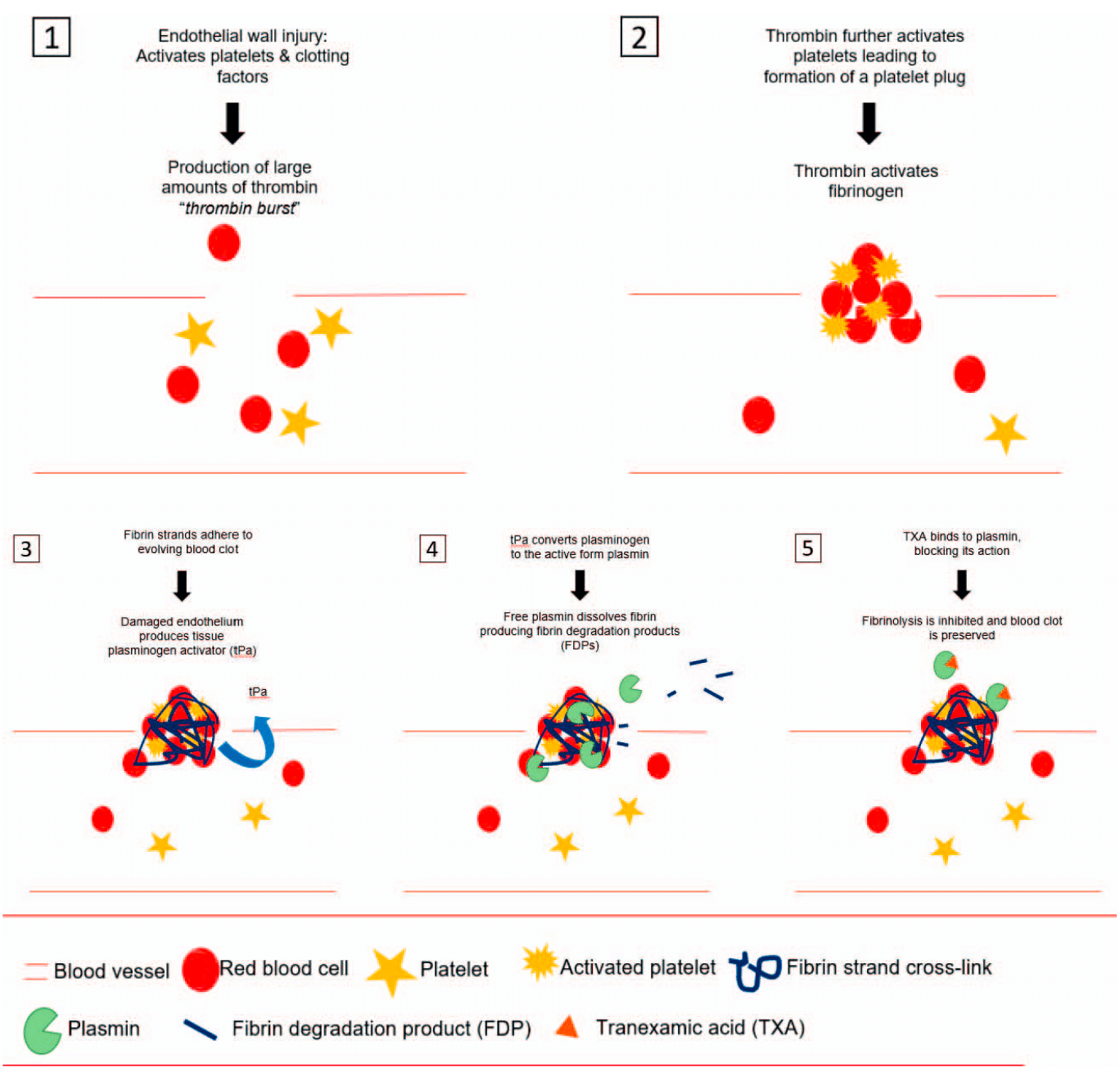
Figure. The clotting and fibrinolytic systems.
FIBRINOLYSIS AND MECHANISM OF ACTION OF TRANEXAMIC ACID
Tranexamic acid has beneficial actions on fibrinolysis, platelet function and the systemic inflammatory syndrome5.
Following trauma, surgery, or exposure to extracorporeal circulations the body’s ability to regulate local fibrinolysis is exceeded and generalised fibrinolysis can occur leading to a coagulopathy. Vascular endothelial wall stress activates the clotting cascade leading to platelet activation and plug formation, large amounts of thrombin production and later fibrin cross-links that strengthen the developing blood clot (a mass of red blood cells, white blood cells, platelets, fibrinogen, fibrin and plasminogen). To prevent uncontrolled growth of the blood clot, fibrinolysis is also initiated. Fibrinolysis is activated locally by plasminogenactivators found in endovascular endothelium as well as being produced by macrophages that convert plasminogen to plasmin and promote fibrinolysis at the site of clot formation5.
Tranexamic acid is a synthetic derivative of the amino acid lysine and inhibits fibrinolysis by reversibly binding to lysine-binding sites on plasminogen, thereby preventing the cleavage of fibrin5,6. (See Figure)
Plasmin acts on platelets to reduce platelet aggregation and adhesion and therefore tranexamic acid, by reducing the formation of plasmin, helps to preserve platelet function5. Plasmin and plasminogen also demonstrate pro-inflammatory effects including monocyte activation and cytokine production and whilst the role of tranexamic acid in reducing inflammation is not fully

Table 1. Dose Adjustment in Renal Impairment
elucidated the expression of several pro-inflammatory genes is altered in the cardiac setting following the administration of tranexamic acid and it demonstrates a reduction in the systemic-inflammatory-response-syndrome and subsequent vasopressor use 7. It has also been shown to inhibit complement 6.
There is limited evidence that some patients experience a fibrinolytic shutdown scenario whereby they increase their own plasminogen-activator inhibitor activity and thus would not benefit from tranexamic acid and may become pro-thrombotic if tranexamic acid is given to this subset of patients. This is an ongoing area of research and currently has not impacted clinical guidance on usage 7.
PHARMACOKINETICS
Absorption
Maximum plasma concentrations of tranexamic acid are attained within 3 hours of an oral dose and absorption is not slowed by a full stomach. Peak concentrations occur rapidly after intravenous injection and fall in a multi-exponential manner 6.
Distribution
Tranexamic acid has a volume of distribution of 9-12L and is 3% plasma-protein bound. It has good penetration of joint fluid and synovial membranes as well as crossing the placenta and blood-brain barrier. In both cerebrospinal fluid and aqueous humour, concentrations are 1/10 that of plasma and with minimal concentrations in breast milk (1/100), it is considered safe in breast feeding6.
Metabolism and Elimination
Tranexamic acid is excreted unchanged in the urine and 90% is excreted within the first 24 hours after an intravenous dose6. Doses should be adjusted in renal insufficiency.
Routes of Administration, Storage and Compatibility
Oral, topical and intravenous formulations exist but intra-cerebral and intrathecal use are contraindicated due to seizure activity in animals. It has a long shelf-life of 3 years and can be stored at room temperature. Intravenous tranexamic acid is compatible with electrolyte, glucose and amino acid solutions as well as with heparin6. (See Table 1)
Side Effect Profile
Seizures
Administration of topical tranexamic acid directly to the central nervous system in animals provokes seizures. Clinically, tranexamic acid has been shown to increase the risk of seizures in patients undergoing cardiac surgery, largely when moderate and high doses (more than 10mg/kg) are used. Possible causal mechanisms include inhibition of GABA-A and glycine inhibitory receptors leading to stimulation of excitatory pathways, as well as an increased susceptibility of cardiac patients to postoperative seizures due to emboli introduced during surgery 3. Increased risk of seizures has not been observed in other clinical settings. However, manufacturers advise avoidance of tranexamic acid in all patients with a history of convulsions6.
Thrombo-embolism
There is a theoretical basis for concerns that tranexamic acid could promote thrombus formation, and this is supported by in vivo animal studies showing a dose-dependent increase in thrombus and risk of thrombo-embolism7. However, multiple metaanalyses have failed to show an increased risk of myocardial infarction, stroke, pulmonary embolism or deep vein thrombosis with tranexamic acid compared to placebo5,7,8. Subsequently, it is recommended that an acute venous thromboembolism is an absolute contraindication to tranexamic acid, and a risk/benefit analysis must be undertaken if there is a personal history of VTE6. (See Table 2)
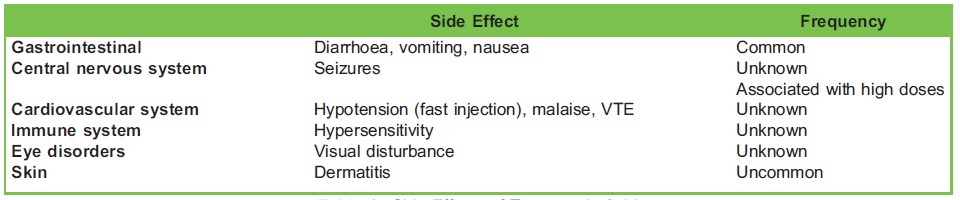
Table 2. Side Effects of Tranexamic Acid
CLINICAL USES
Tranexamic acid reduces blood loss in patients with both normal fibrinolysis and hyperfibrinolysis6. Hyperfibrinolysis can occur following surgery, trauma, tissue damage or exposure to extracorporeal circulations where the body’s natural ability to regulate local fibrinolysis is exceeded and fibrinolysis becomes systemic, leading to coagulopathy. Additionally, during clot formation fibrinogen is consumed rapidly and early tranexamic acid preserves fibrinogen stores during haemorrhage. Therefore, clinicians should aim to prevent, rather than treat, coagulopathy and administer tranexamic acid as early as possible.
It is a cost-effective intervention for preventing bleeding during major surgery across a broad spectrum of surgical procedures, reducing average peri-operative blood loss, and subsequent transfusion, by 34% and 39% respectively9. Blood transfusion is costly and scarce, especially in areas with limited resources and poses multiple risks to patients including transfusion-related reactions, immunomodulation and transfusion transmitted infection. (See Table 3)
Trauma
Trauma is a major contributor to death worldwide with haemorrhage causative in 1/3 of in-hospital trauma deaths. Early clotting abnormalities, including hyperfibrinolysis, occur frequently in trauma patients and substantially contribute to mortality. A large study found that 1g of intravenous tranexamic acid, compared to placebo, reduced risk of death from bleeding by 15% with no increased risk of any adverse events1. However, treatment benefit decreases by 10% for every 15 minute delay after the first
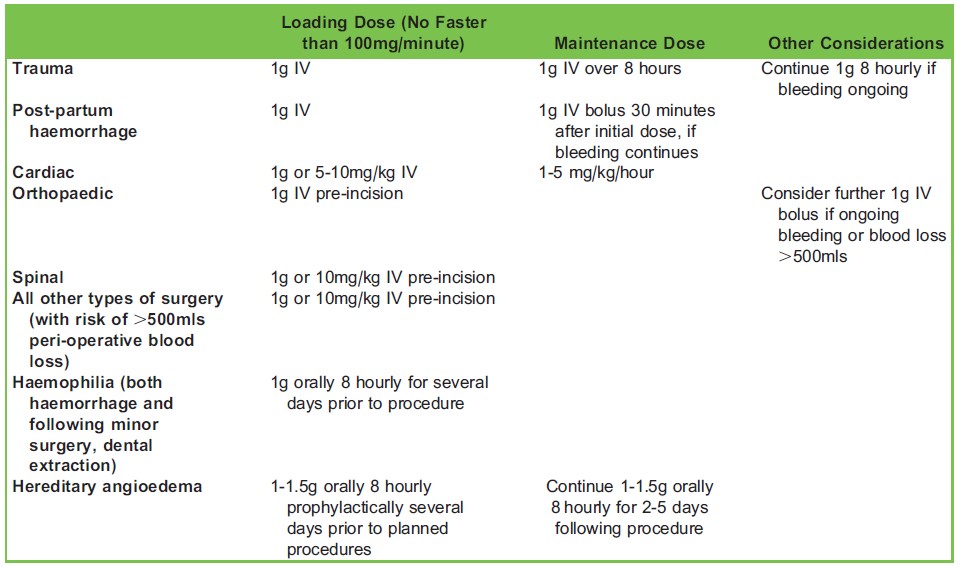
Table 3. Summary Dosing Table
hour following onset of haemorrhage and therefore should be given as soon as possible but certainly within 3 hours. After 3 hours it should be omitted unless there is clear evidence of hyperfibrinolysis on blood results10.
Obstetrics
Postpartum haemorrhage is the leading cause of maternal mortality worldwide. Within 1 hour of birth the concentration of plasminogen doubles leading to activation of fibrinolysis. Despite not showing a reduction in the volume of blood loss or transfusion rate, the WOMAN trial demonstrated that intravenous tranexamic acid, compared to placebo, reduced the risk of death from bleeding by almost 1/3 with no increase in adverse events for mother or baby2. It should therefore be given as a 1g intravenous bolus as close as possible to bleeding onset (birth) and a further 1g intravenous dose can be repeated 30 minutes later if bleeding continues. It is not to be given if more than 3 hours has elapsed since birth due to lack of treatment benefit.
Cardiac
Tranexamic acid has several beneficial actions in patients undergoing cardiac surgery. These patients are at high risk of blood loss, and subsequent transfusion, due to the highly invasive nature of cardiac surgery, high dose anticoagulation and blood lost within the extracorporeal cardiopulmonary bypass circuit. Exposure to the extracorporeal circuit activates the fibrinolytic system and causes platelet dysfunction, thus in addition to its’ antifibrinolytic activity tranexamic acid helps preserve platelet function during cardiopulmonary bypass3. Patients undergoing major cardiac surgery often suffer a profound systemic inflammatory response syndrome leading to shock and multiorgan failure and tranexamic acid has been shown to alter the expression of several inflammatory genes, dampening this inflammatory response5.
Tranexamic acid reduces the rate of blood loss, risk of reoperation due to haemorrhage (which carries increased morbidity and mortality) and the need for blood transfusion with no increased risk of death or thrombotic complications in patients undergoing on-pump or off-pump surgery3. However, it does cause an increased risk of seizures demonstrating a dose-dependent relationship. Therefore lower dose tranexamic acid (5-10mg/kg) is being increasingly used in UK cardiac centres with less postoperative seizures observed as a result. Seizures generally occur within hours of surgery and are grand-mal in nature. Those who have post-operative seizures are subsequently more at risk of stroke or death. The risk of seizures is particularly high in the elderly, those with pre-existing renal failure and those undergoing open-heart surgery3.
Orthopaedic
Prosthetic implantation and use of a tourniquet activates fibrinolysis and haemorrhage is common post arthroplasty. Patients presenting for hip and knee joint replacement are often elderly with multiple co-morbidities such as anaemia and ischaemic heart disease, that render them more susceptible to bleeding-related morbidity and mortality. Tranexamic acid significantly reduces blood loss in total hip and knee replacement. Intravenous delivery appears to provide the most benefit but both oral and combination topical/intravenous preparations are favourable to placebo4. Tranexamic acid has excellent joint penetration and its use has been fully embedded in total knee and hip arthroplasty fast track protocols in many centres. Similar usage is expected in the future in all types of major arthroplasty.
Intra-cranial Haemorrhage
In spontaneous haemorrhage tranexamic acid can reduce haematoma expansion and leads to fewer deaths at 7 days with no increased risk of seizures or other adverse events but with no significant improvement in neurological or mortality outcomes at 90 days11. Therefore it is not currently recommended in clinical practice but results are anticipated from an ongoing study (STOP-AUST) into the benefit of tranexamic acid in a subset of these patients and a meta-analysis of ongoing multiple smaller trials is planned.
Spinal Surgery
Research in spinal surgery and tranexamic acid has largely been on smaller studies showing a slight reduction in blood loss and transfusion rate following administration of tranexamic acid but differences have not yet shown to be statistically significant. As there have been no adverse outcomes alongside increasing evidence in most other surgical specialties tranexamic acid is recommended in all spinal surgery that carries a risk of major bleeding (>30% total estimated blood volume) and/or surgery involving fusion at 3 vertebral levels12.
Other Uses
Tranexamic acid has been introduced prophylactically across a wide range of other conditions and procedures including haemophiliacs undergoing any surgery, hereditary angioedema, and prostatectomy. It should be used, unless contraindicated, in any other major surgery at risk of more than 500ml blood loss or loss of 10% circulating blood volume. It is also recommended for treatment of major bleeding from haemoptysis and gastrointestinal haemorrhage7,8. Currently a large multicentre trial (HeLiX) is investigating the impact of tranexamic acid on perioperative blood transfusion in patients undergoing liver resection13.
SUMMARY
Tranexamic acid significantly reduces peri-operative blood loss in a wide variety of surgical specialties and improves survival in haemorrhage from trauma and birth. In cardiac patients it carries a risk of seizures, especially with higher doses, and theoretically may predispose to thromboembolic disease but clinically relatively few side effects are observed. It is highly cost-effective and requires minimal training to administer. As such the World Health Organisation now include it on the essential medicines list. Future research to clarify dosing regimens, especially in the cardiac and paediatric populations, as well as usage in other surgical disciplines and intracranial haemorrhage is expected.
REFERENCES AND FURTHER READING
- CRASH-2 trial collaborators. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet 2010;376:23-3
- WOMAN trial collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebocontrolled trial. Lancet 2017;389:2105-16
- Myles PS, Smith JA, Forbes A, et al. Tranexamic Acid in Patients Undergoing Coronary-Artery Surgery. N Engl J Med 2017;376:136-48
- Fillingham YA, Ramkumar DB, Jevsevar DS, et al. The Efficacy of Tranexamic Acid in Total Hip Arthroplasty: A Network Meta-Analysis. J Arthroplasty 2018;33:3083-3089.e4 https://www.arthroplastyjournal.org/article/S0883-5403(18)30593-X/ fulltext. Accessed September 8, 2018.
- Levy JH, Koster A, Quinones QJ, Milling TJ, Key NS. Anti-fibrinolytic therapy and perioperative considerations. Anesthesiology 2018;128:657-670
- Datapharm electronics Medicines Compendium (eMC). Pfizer Limited Cyklokapron Injection Summary of product characteristics. https://www.medicines.org.uk/emc/product/1077/smpc. Accessed July 2, 2018.
- Ng W, Jerath A, Wasowicz M. Tranexamic acid: a clinical review. Anaesthesiol Intensive Ther 2015;47:339-50
- Kozek-Langenecker SA, Ahmed AB, Afshari A, et al. Management of severe perioperative bleeding: guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol 2017;34:332-395
- Henry DA, Carless PA, Moxey AJ, et al. Anti-fibrinolytic use for minimising perioperative allogeneic blood transfusion. Cochrane database of systematic reviews 2011. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD00 1886.pub4/full. Accessed July 21, 2018.
- Gayet-Ageron A, Prieto-Merino D, Ker K, et al. Effect of treatment delay on effectiveness and safety of anti-fibrinolytics in acute severe haemorrhage. Lancet 2018;391:125-132
- Sprigg N, Flaherty K, Appleton JP, et al. Tranexamic acid for hyperacute primary IntraCerebral haemorrhage (TICH-2): an international randomised, placebo-controlled, phase 3 superiority trial. Lancet 2018;391:2107-15.
- Colomina MJ, Koo M, Basora M, Pizones J, Mora L and Bago J. Intraoperative tranexamic acid use in major spine surgery in adults: a multicentre, randomized, placebo-controlled trial. Br J anaesth 2017;118:380-90
- U.S. National Library of Medicine. Clinical trials.gov. https://clinicaltrials.gov/ct2/show/NCT02261415. Accessed May 22, 2019
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/