Regional Anaesthesia

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation. Please answer True or False:
- Regarding the anatomy of the adductor canal (sub-sartorial canal):
a. It is roughly triangular in cross section and is bounded by four muscles.
b. The canal contains the femoral artery, femoral vein, posterior branch of the obturator nerve and branches of the femoral nerve.
c. It extends from the upper, anterior thigh where sartorius crosses adductor longus to the lower lateral thigh.
d. 12-14 cm distal to the knee is the adductor hiatus, a distal opening in the adductor magnus muscle.
e. It is an inter-muscular tunnel in the middle third of the thigh. - The saphenous nerve:
a. Is a branch of the femoral nerve.
b. Is both motor and sensory.
c. Innervates the lateral side of the lower leg and foot; albeit with significant inter-patient variability.
d. Follows the saphenous vein subcutaneously along the medial side of the knee to the lower leg.
e. Provides sensory innervation to the knee joint. - The adductor canal block:
a. Involves injection of local anaesthetic into the adductor canal deep to sartorius.
b. Is useful after lower limb, foot and ankle surgery (usually in combination with a popliteal block).
c. Is not useful for post-operative analgesia after knee arthroscopy or anterior cruciate ligament reconstruction.
d. Generally small volumes of local anaesthetic are used and spread distally down the adductor canal.
e. Is performed with the patients leg extended and internally rotated.
INTRODUCTION
As a purely sensory nerve the saphenous nerve innervates the medial side of the lower leg and foot; albeit with significant inter-patient variability. The adductor canal block involves injection of local anaesthetic into the adductor canal deep to the sartorius muscle and is a technically easy and reliable method for blocking the saphenous nerve1. This may be useful for post-operative analgesia after knee, foot or ankle surgery (usually in combination with a popliteal block). It will also result in block of the infra-patellar nerve2 which may be useful for post-operative analgesia after knee arthroscopy3 or anterior cruciate ligament repair.
Finally, larger volumes of local anaesthetic may spread proximally up the adductor canal resulting in sensory block of the whole of the front of the knee without appreciable motor block4,5. This may be useful in major knee surgery (such as total knee arthroplasty) and recent evidence for this, although limited is encouraging6.
ANATOMY
The Adductor Canal
The position of the saphenous nerve in the adductor canal has been well described, originally by Mansour7 and later revisited by Hornet al.8 Gray et al who published an earlier description of ultrasound guided sub-sartorial saphenous block9. The adductor canal, also known as Hunter’s canal or the sub-sartorial canal, is an aponeurotic intermuscular tunnel in the middle third of the thigh (figure1).
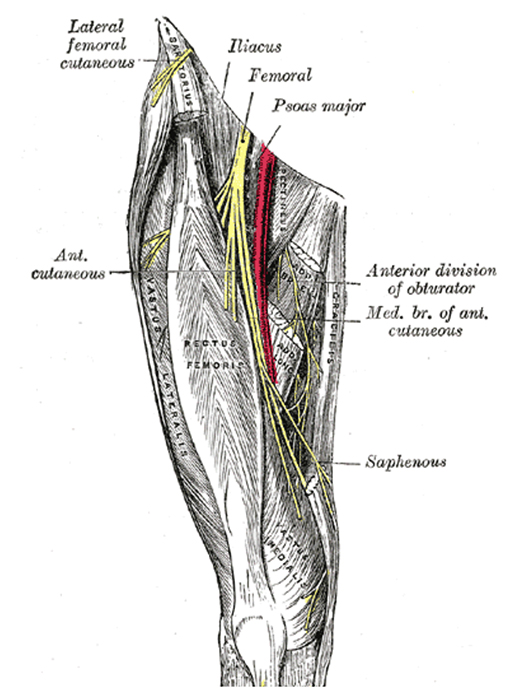
Figure 1: Course of Femoral nerve and its branches.
The canal is roughly triangular in cross section and is bounded by three muscles: quadriceps anterolaterally (specifically vastusmedialis), sartorius medially and adductor magnus posteriorly. This muscular tunnel extends from the upper, anterior thigh at the point at which sartorius crosses adductor longus to the lower, medial thigh. Approximately 12-14 cm proximal to the knee is the adductor hiatus, a distal opening in the adductor magnus muscle. Within this canal is the femoral artery, femoral vein, the posterior branch of the obturator nerve, and branches of the femoral nerve; specifically the saphenous nerve and nerve to vastus medialis (Figure 2).
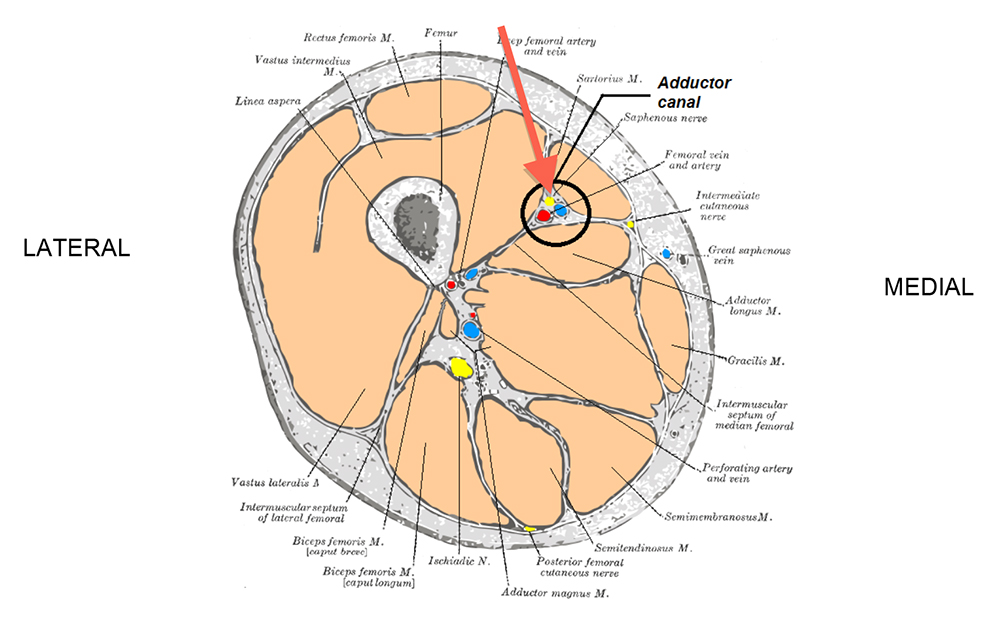
Figure 2: Sagittal section through mid-thigh showing the adductor canal
At the adductor hiatus, the femoral vessels pass deeply before leaving the canal. The femoral artery changes course to this deeper plane to become the popliteal artery and the saphenous nerve travels with the smaller descending genicular artery to emerge from the adductor canal to eventually diverge from the artery and become subcutaneous.
It is this sudden change in depth that is a useful indicator of the canals distal limit, and therefore the optimal level to form the adductor canal (sub-sartorial) block. Once the saphenous nerve becomes subcutaneous it follows the saphenous vein along the medial side of the knee to the lower leg.
The posterior division of the femoral nerve sends branches to the quadriceps muscle (particularly vastus lateralis and vastus intermedius). Together with the saphenous nerve, each one of these branches gives rise to articular nerves that provide sensory innervation to the knee joint. It is for this reason the saphenous nerve block does not provide as good analgesia after knee surgery as the conventional femoral block at the inguinal level. The clinical relevance of these proximally arising femoral sensorynerves in terms of mediating pain after knee surgery (compared to the saphenous nerve) is at present unknown.
INDICATIONS
This is not intended to be an exhaustive list, but the following operations may benefit from adductor canal block:
Low volume block (5-10mls)
- Knee arthroscopy.
- Anterior Cruciate Ligament reconstruction (ACLr).
- Lower leg, foot and ankle surgery involving areas of skin supplied by the saphenous nerve.
High volume block (20-30mls)
- Total and uni-compartmental knee replacement.
CONTRAINDICATIONS
Absolute
- Patient refusal.
- Inflammation or infection over injection site.
- Allergy to local anaesthetics.
Relative
- Anticoagulation or bleeding disorders.
- Pre-existing peripheral neuropathies.
COMPLICATIONS
These are the same as for any regional anaesthetic technique:
- Block failure.
- Bleeding/Bruising.
- Infection.
- Local anaesthetic toxicity.
- Nerve injury.
GENERAL PREPARATION
Before starting ensure there are appropriate indications for a sub-sartorial block and no contraindications. Consent the patient and advise them on the likely duration of block.
Ensure the site/side is clearly marked, the patient is monitored, IV access obtained and that appropriate, assistance, equipment and resuscitation drugs are available. For complete details on preparation for peripheral nerve blocks please see ATOTW tutorial no.134 “Peripheral nerve blocks – Getting started”.
Specific equipment required
- 22-gauge 100mm length, short-bevelled regional block needle.
- Skin antiseptic solution.
- Sterile gloves.
- 1-2 ml of 1% lignocaine for skin infiltration in awake patients.
- Low volume block: 5-10mls of long-acting local anaesthetic, e.g. 0.25-0.5% Bupivacaine, Levobupivacaine or 0.2-0.75% Ropivacaine.
- High volume block: 20-30mls of long-acting local anaesthetic.
- Portable ultrasound machine.
PROCEDURE
- Confirm operative site and side with patient; Check limb is marked and corresponds with information on consent form.
- Apply full monitoring as per AAGBI guidelines.
- Secure IV access.
- If required, proceed with sedation/induction of general anaesthesia/spinal anaesthesia as per anaesthetic plan.
- Position patient supine with knee slightly flexed and leg externally rotated (frog leg position).

Figure 3: Patient positioning
- Clean the area with 0.5% Chlorhexidine spray.
- Stand to the side of the patient to be blocked with the ultrasound machine on the opposite side and the screen facing you.
- Place a high frequency ultrasound probe on the anterior aspect of the patient’s thigh, approximately mid-point between the inguinal crease and medial condyle.
- Identify the femur (usually at a depth of 3-5cm although variable) and move probe medially until the trapezoid/boat shaped Sartorius muscle is visualised (Figure 4).
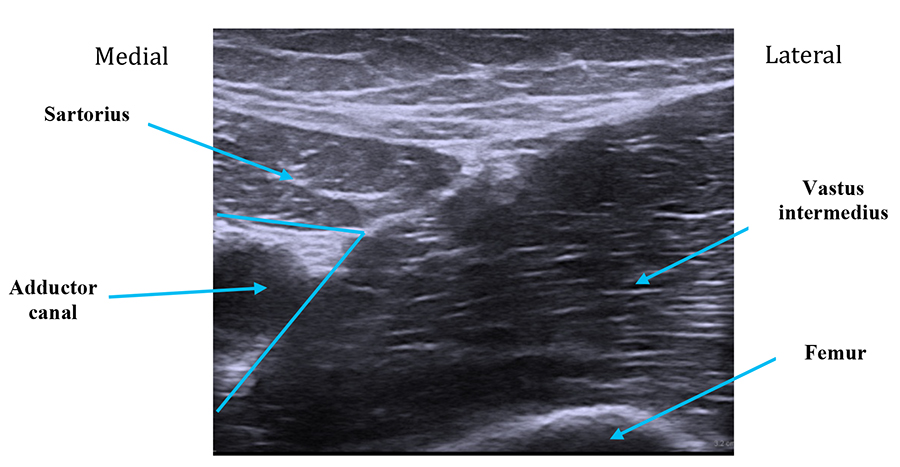
Figure 4: Notice the femur (bottom right) with the vastus intermedius muscle upon it. The adductor canal lies medially just beneath sartorius.
- The femoral artery lies just under this muscle within the adductor canal. Please note the saphenous nerve is almost always too small to be reliably imaged and the aim of the technique is therefore to deposit local anaesthetic under Sartorius and around the femoral artery (i.e. within the adductor canal).(Figure 5)
- Optimise image, adjusting depth, gain and frequency settings as required.
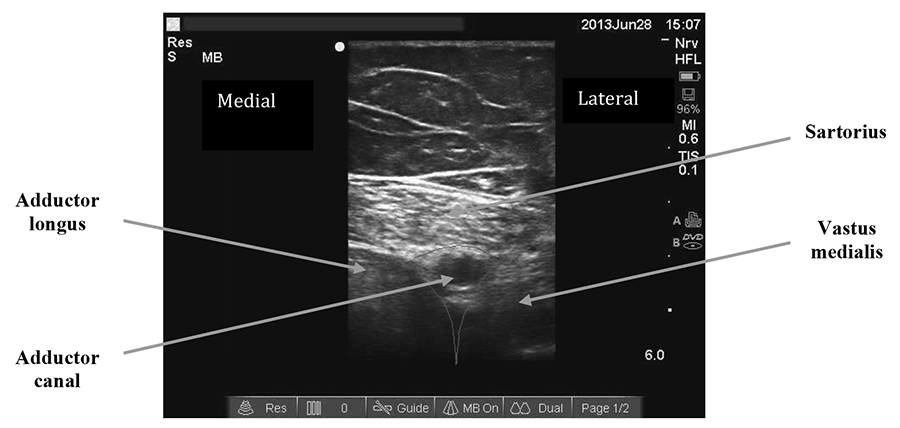
Figure 5: The adductor canal beneath sartorius
- The appropriate probe position is just proximal to where the femoral artery “dives” posteriorly and the probe should be positioned perpendicular to artery. At this point the femoral artery should start to pass deeper to form the popliteal artery. The vastus medialis muscle lies anterolateral, the adductor magnus muscle posteromedial and the sartorius muscle medial. Use an in-plane approach from lateral to medial ensuring that your needle tip can be seen at all times.
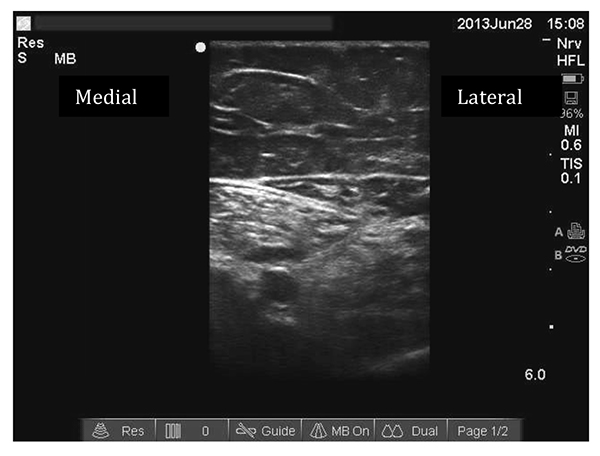
Figure 6: Needle traversing sartorius and tip within adductor canal ( in-plane needle approach)
- Advance your needle into the adductor canal. This can be achieved by traversing sartorius or vastus medialis. Aspirate and inject a test dose of 1ml of the local anaesthetic solution.
- Observe the spread of the local anaesthetic to ensure your needle tip is definitely within the adductor canal. If you cannot clearly see the spread of local anaesthetic consider intravascular placement of needle and reposition.

Figure 7: Local anaesthetic spreading under sartorius within adductor canal
- Continue with the remainder of the injection, aspirating every 5mls.
POST-PROCEDURE CARE
- Continue monitoring the patient carefully, looking particularly for signs of local anaesthetic toxicity.
- Document the block clearly including whether done awake or after GA or spinal, the side and site of injection, needle used, volume and name of local anaesthetic, and any associated problems (for example vascular puncture).
- All patients should be seen or contacted postoperatively to ensure that the block has worn off completely.
Clinical tips
- During injection further needle adjustments may be required to ensure local anaesthetic spreads around both sides of the femoral artery. (The saphenous nerve begins lateral to the femoral vessels but crosses to medial during its course through the adductor canal).
- An out of plane approach is an acceptable alternative to an in plane approach as long as you can ensure that your needle tip is visualised at all times.
- If you have difficulty identifying the femoral artery first check that the depth of your survey is adequate. Then move the probe circumferentially around the thigh until the vessel is identified.
- Use of a colour flow Doppler mode may also help to identify the artery.
- If difficulty persists, follow the femoral artery distally from the inguinal crease until sartorius is seen superficial to it thus forming the adductor canal.
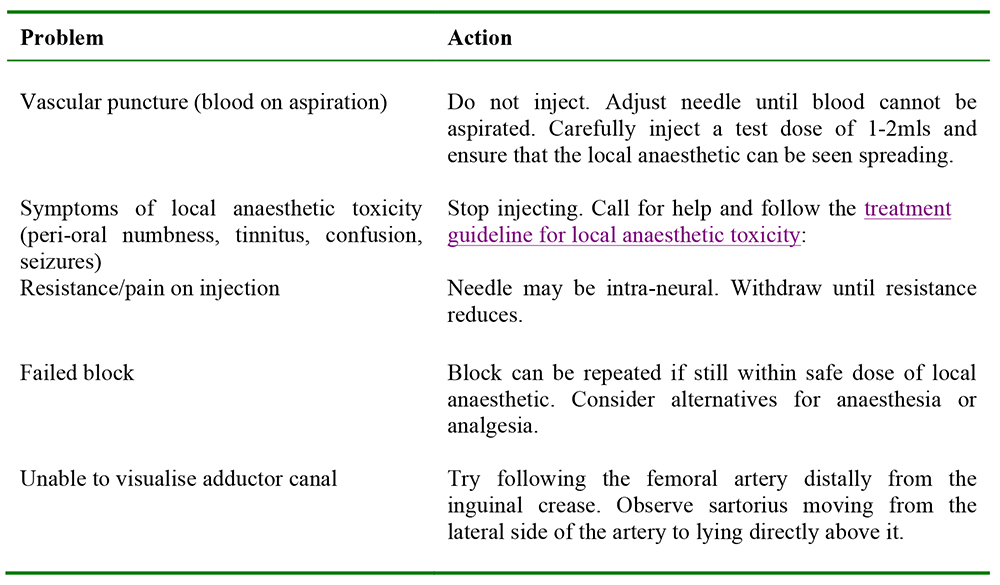
TROUBLESHOOTING
COMPLICATIONS
Common to all blocks
- Block failure.
- Intravascular injection.
- Local anaesthetic toxicity:
- Central nervous system effects cause tinnitus, peri-oral numbness, metallic tastes,confusion and seizures.
- Cardiac effects cause tachycardia, hypertension, arrhythmias and potentiallycardiac arrest.
- For details on the management of local anaesthetic toxicity please seetroubleshooting, above.
- Nerve damage- temporary or permanent.
- Infection.
- Allergy to local anaesthetic.
- Methaemoglobinaemia when using Prilocaine.
Specific to adductor canal block
- Vascular puncture.
- Haematoma.
SUMMARY
Key safety points
- Always perform the block in an appropriate setting using suitable equipment with a trained assistant and resuscitation facilities to hand.
- Always prepare your patient correctly ensuring informed consent, appropriate monitoring and intravenous access.
- Always ensure you are within the safe dose of local anaesthetic.
- Never try to inject the local anaesthetic dose if blood has been aspirated, the patient complains of pain or there is resistance to injection.
- If symptoms of local anaesthetic toxicity develop, stop injecting, call for help and follow the AAGBI guidelines on the management of severe local anaesthetic toxicity.
- As with any peripheral nerve block be prepared for block failure and have a backup plan.
- The ultrasound-guided adductor canal block provides a reliable method for blocking the saphenous nerve. It is therefore a useful technique for post-operative analgesia following foot and ankle surgery.
- The block also results in blockade of the infra-patellar nerve. It is therefore a useful technique for post-operative analgesia following knee arthroscopy.
- Higher volumes of local anaesthetic spread proximally up the adductor canal and result in motor sparing sensory change over the front of the knee.
- Current evidence for use for Total Knee Replacement is limited but encouraging.
ANSWERS TO QUESTIONS
- Please answer True or False: Regarding the anatomy of the adductor canal (sub-sartorial canal)
a. False. It is bounded by 3 muscles: sartorius, vastus medialis and adductor longus.
b. True.
c. False. It is extends to the lower medial thigh.
d. False. The adductor hiatus is proximal to the knee.
e. True. - Please answer True or False: The saphenous nerve:
a. True.
b. False. It is a purely sensory nerve.
c. False. It innervates the medial side of the leg.
d. True.
e. True. - Please answer True or False: The sub-sartorial block:
a. True.
b. True.
c. False. It may be useful after ACL repair.
d. False. Larger volumes of local anaesthetic may spread proximally up the adductor canal.
e. False. The leg should be slightly flexed at the knee and externally rotated (frog leg position).
WEBLINKS
REFERENCES and FURTHER READING
- Manickam B et al.Feasibility and efficacy of ultrasound-guided block of the saphenous nerve in the adductor canal. RegAnesth Pain Med. 2009;34: 578-580
- M. Lundblad M et al.Ultrasound-guided infrapatellar nerve block in human volunteers: description of a novel technique. BJA. 2006;97(5): 710–14
- Akkaya T et al. Saphenous nerve block is an effective regional technique for post-menisectomy pain. Knee Surg Sports TraumatolArthrosc. 2008;16(9): 855-8
- Jenstrup MT et al. Effects of adductor-canal-blockade on pain and ambulation after total knee arthroplasty: a randomized study. ActaAnaesthesiol Scand. 2012;56(3):357-64
- Kwofie MK et al. The effects of Ultrasound-Guided Adductor Canal Block Versus Femoral Nerve Block on Quadriceps Strength and Fall Risk. A blinded, Randomized Trial of Volunteers. RegAnesth Pain Med 2013; 38 (2): 321-325
- Andersen HL et al. Continuous Saphenous Nerve Block as Supplement to Single-Dose Local Infiltration Analgesia for postoperative Pain Management After Total Knee Arthroplasty. RegAnesth Pain Med 2013; 38 (2): 106-111
- MansourNY..Sub-sartorial saphenous nerve block with the aid of nerve stimulator. Regional Anesthesia. 18(4):266-8, 1993 Jul-Aug.
- Horn ,Pitsch T, Salinas F et al. Anatomic basis to the ultrasound-guided approach for saphenous nerve blockade. RegAnesth Pain Med 2009; 34: 486–489.
- Gray AT, Collins AB. Ultrasound-guided saphenous nerve block. RegAnesth Pain Med 2003;28: 148.
Sources of Images:
Fig 1: Gray’s Anatomy of the Human Body. www.wikipedia.org/wiki/File:Adductor_canal.png
Fig 2: Gray’s Anatomy of the Human Body. www.wikipedia.org/wiki/File:Gray827.png
Figs 3-7: A McEwen’s personal archive
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/