Regional Anaesthesia

KEY POINTS
- Ultrasound-guided infraclavicular brachial plexus block can provide excellent analgesia and anaesthesia for surgery below the mid-humerus, elbow, forearm, wrist, and hand.
- The infraclavicular brachial plexus has easily recognisable sonoanatomy, a high success rate, and low risk of phrenic nerve palsy. Identification of the axillary artery is the key landmark in performing this block.
- The classic approach may be challenging because of the very narrow area between the probe and clavicle and may require a steep needle angle at the insertion point.
- The infraclavicular block is very well suited for both a single shot and a catheter technique.
- The infraclavicular position allows for a well-anchored placement of a catheter for continuous local anaesthesia infusion when compared with supraclavicular and axillary brachial plexus block.
INTRODUCTION
Infraclavicular brachial plexus block (IC-BPB) is used to provide anaesthesia and analgesia for distal upper arm, elbow, forearm, and hand surgery. Traditionally, a combination of anatomical landmarks and nerve stimulator techniques have been favoured.1–4 The use of ultrasound (US) adds valuable information such as visualisation of the needle tip and real-time observation of the injectate surrounding the nerves.5 US use also reduces the risk of adverse events such as inadvertent intravascular injection and trauma to surrounding structures.6 As there is now widespread availability of high-quality US machines, their use has become standard practice when performing an IC-BPB.7,8 Performance of the IC-BPB can be challenging and requires specific skills and training to allow optimal and safe block performance.
Anatomy and Sonoanatomy for the IC-BPB
The anterior rami of the C5-T1 spinal nerves is the origin of the innervation to the upper limb. The roots of these nerves form into 3 trunks, branch into 6 divisions, then rejoin into 3 cords, which ultimately form the terminal branches of the brachial plexus. These terminal branches are the musculocutaneous, axillary, median, ulnar, and radial nerves (Figure 1). The divisions of the brachial plexus travel laterally from the posterior triangle of the neck toward the axilla. In the axilla, the divisions merge to form 3 distinct cords: the medial, the lateral, and the posterior cords. The cords of the brachial plexus are located beneath the clavicle and are named according to their relation to the axillary artery (Figure 1). A wide variation is observed with the position of the cords and their relation to the axillary artery, which may make their identification challenging (Figure 2).
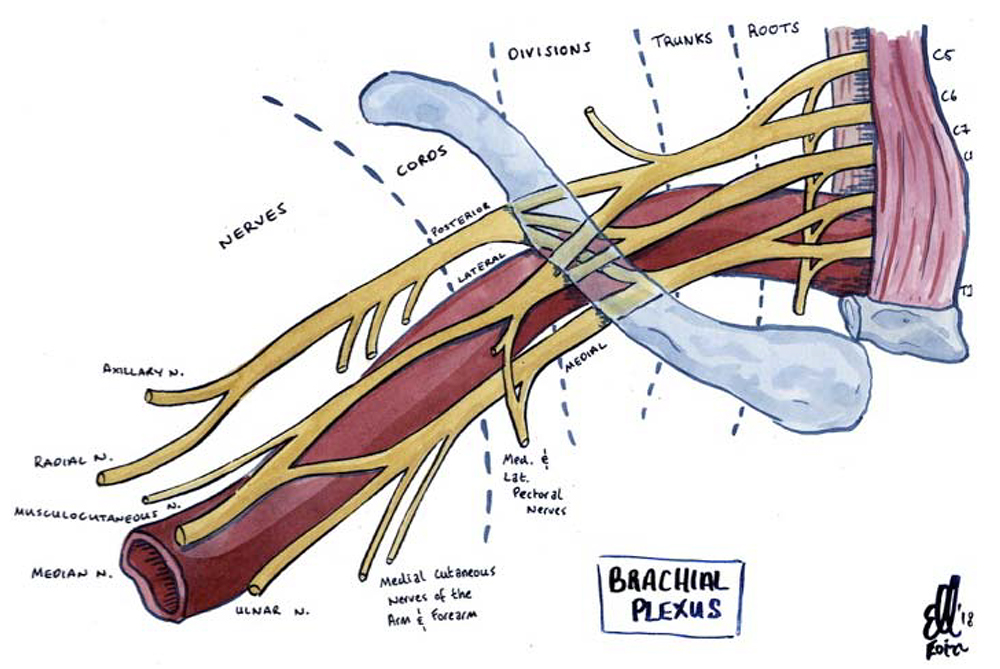
Figure 1. Illustration of the right brachial plexus. Illustration supplied by Dr. Eoin Kelleher, Specialist Registrar in Anaesthesia, Mater Misericordiae University Hospital, Dublin, Ireland.
The anatomical relations of the brachial plexus in this location are the pectoralis major and minor muscles anteriorly, the subscapularis muscle posteriorly, the clavicle and coracoid process superiorly, the ribs and intercostal muscles medially, and the humerus laterally. The location of the cords of the brachial plexus is deeper from the skin (≥4 cm) compared with the brachial plexus at other locations.
Blockade of the brachial plexus just below the clavicle at the cord level is known as an IC-BPB. The cords are located around the axillary artery (Figure 3), which is a key structure to identify when performing this block.
INDICATIONS, CONTRAINDICATIONS, AND COMPLICATIONS
Indications
The IC-BPB provides anaesthesia and analgesia of the midhumerus, elbow, forearm, and hand. The IC-BPB is an alternative approach to anaesthetising the brachial plexus and is advantageous in patients with limited mobility of the upper limb, such as seen in acute trauma, limb deformity, or advanced shoulder arthropathy.
The performance of the IC-BPB is safe and effective and can offer several advantages over other approaches to the brachial plexus (eg, interscalene, supraclavicular, and axillary brachial plexus block)1:
- The IC-BPB can provide a more reliable block of the ulnar nerve than more proximal approaches, with fewer episodes of phrenic nerve palsy, pneumothorax, and Horner’s syndrome.1
- The IC-BPB can be considered in patients unable to abduct the ipsilateral arm in order to perform an axillary brachial plexus block.2
- The musculocutaneous, axillary, and medial nerve of the forearm leave the brachial plexus proximally, which may require several needle redirections to block these nerves when performing an axillary brachial plexus block. This is avoided when an
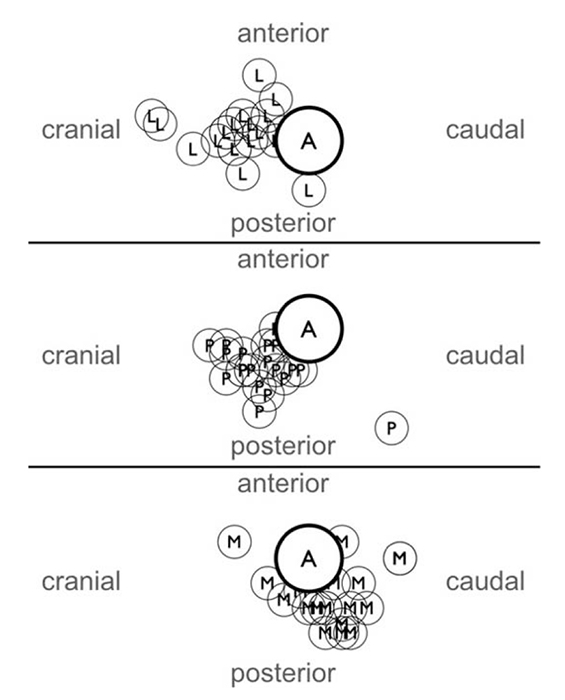
Figure 2. Illustration of the anatomical variation of the cords around the axillary artery at the level of the clavicle. A indicates axillary artery; L, lateral cord; P, posterior cord; M, medial cord. From Sauter AR, Smith HJ, Stubhaug A, Dodgson MS, Klaastad O. Use of magnetic resonance imaging to define the anatomical location closest to all three cords of the infraclavicular brachial plexus. Anesth Analg. 2006;103(6):1574-1576. Reproduced with permission.

Figure 3. Ultrasound view of the left infraclavicular brachial plexus. Location of the cords in relation to the axillary artery at the infraclavicular level. AA indicates axillary artery; AV, axillary vein; MC, medial cord; PC, posterior cord; LC, lateral cord. Image supplied by Dr. Georgi Valchev, Consultant Anaesthetist, Mater Misericordiae University Hospital, Dublin, Ireland.

Table 1. Absolute and Relative Contraindications. RAPTIR ¼ retroclavicular approach to the infraclavicular region
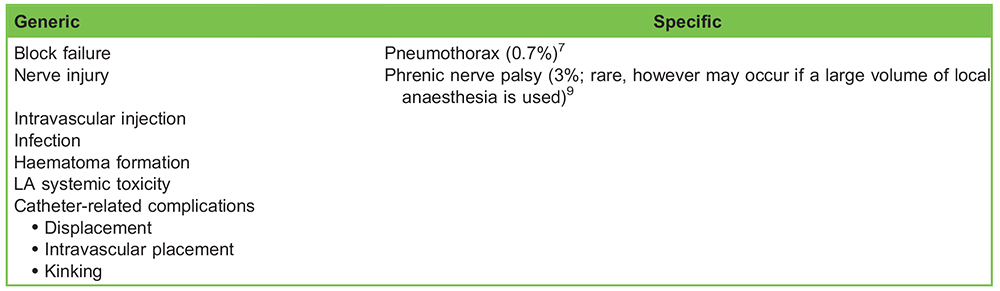
Table 2. Generic and Specific Complications
IC-BPB is performed, because it can be done with a single needle pass.3 Each needle pass or redirection adds time and risk of nerve contact to the procedure.4
- The use of US to visualise local anaesthetic (LA) distribution during an IC-BPB is common and is reported to result in quicker block performance and a higher success rate.5–8
Anatomically advantageous criteria for performing an IC-BPB are a thin pectoral region and nondeformed clavicle.
Contraindications
See Table 1 for the absolute and relative contraindications.
Complications
See Table 2 for generic and specific complications
Techniques of US-Guided IC-BPB
Several approaches to performing the IC-BPB have been described.1–4 These include the ‘‘classic’’ infraclavicular approach (Figure 4) and the retroclavicular approach to the infraclavicular region (RAPTIR; Figure 5).
PERFORMING AN IC-BPB
Equipment Required
- US machine with linear transducer (8-14 MHz)
- A nerve block set with sterile probe cover, gel, sterile gloves, and face mask
- Transparent sterile drape (optional)
- 8- or 10-cm, 21- or 22-gauge insulated, stimulating nerve block needle
- Peripheral nerve stimulator (optional)
- Injection pressure-monitoring system (optional)
- 20-40 mL of LA*
- 5 ml of lidocaine 2% for skin anaesthesia
*The authors advise following local hospital guidelines on LA volumes. Please adhere to the maximum LA dose calculated for each patient. Operators should be familiar with the recognition and management of LA systemic toxicity.
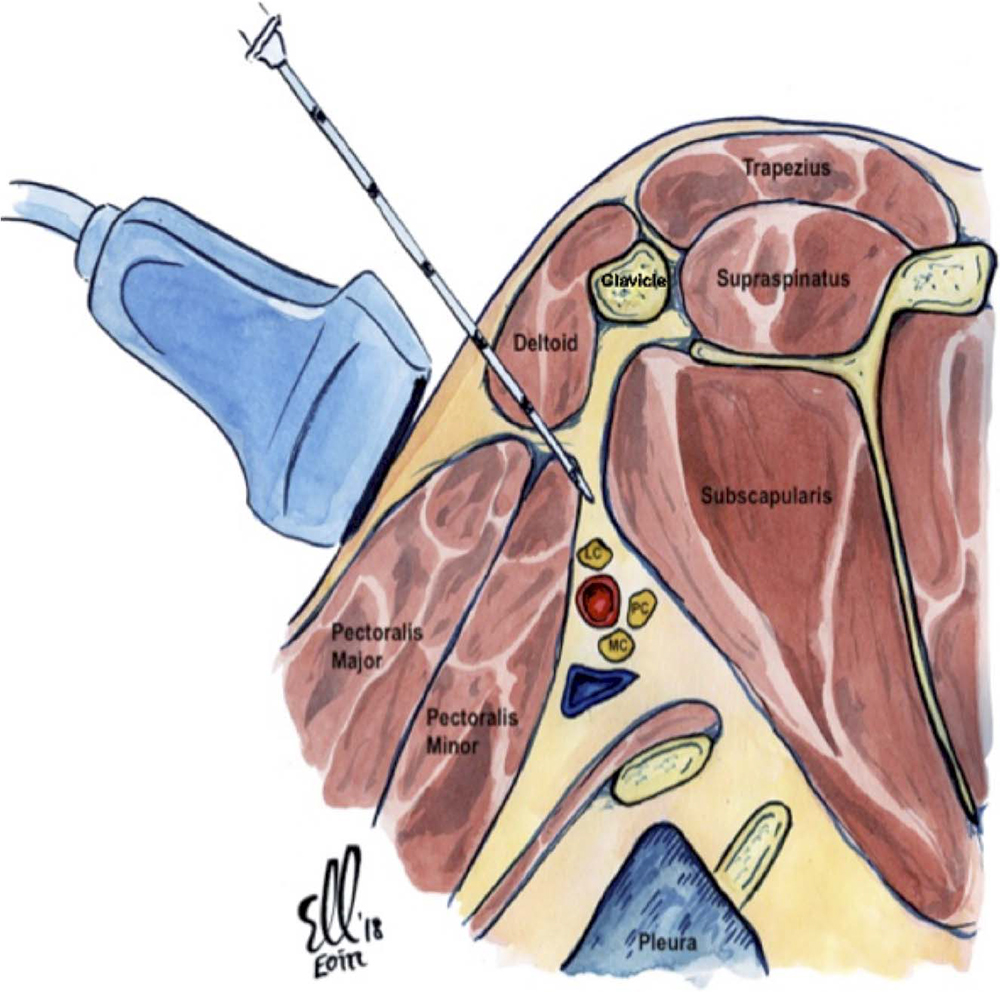
Figure 4. Illustration of the saggital plane of the right infraclavicular brachial plexus with the needle inserted in plane with the ultrasound transducer on the anterior chest wall inferior to the clavicle. This is the classic infraclavicular approach. Illustration supplied by Dr. Eoin Kelleher, Specialist Registrar in Anaesthesia, Mater Misericordiae University Hospital, Dublin, Ireland.
The volume administered for the IC-BPB in the authors’ institution is 30 mL of 0.375% levobupivacaine.
Note: Using a pressure-monitoring system while injecting LA may aid in the detection of intraneural needle tip position.10 The literature suggests that an opening injection pressure greater than 15 pounds per square inch during nerve block may indicate needle-nerve contact and cause neural damage.10 The authors of this tutorial use triple monitoring techniques for IC-BPB composed of US, nerve stimulation, and opening injection pressure.
Patient Positioning
The patient should be placed supine with the head turned toward the contralateral shoulder. Ensure a functioning intravenous cannula is placed, and apply all standards of monitoring as outlined by the Association of Anaesthetists of Great Britain and Ireland.11 A preliminary scan of the area will allow identification of anatomical variation and time to plan the IC-BPB for patients.
There are 2 main setup approaches for performing the block, which can be classified according to the position of the US machine:
- ‘‘Opposite the operator’’: In this configuration, the US machine is placed on the contralateral side to be blocked, opposite to the operator (Figure 6).
- ‘‘Alongside the operator’’: In this configuration, the US machine is on the same side as the operator to allow use of the dominant hand for needling.
In our institution, we prefer the ‘‘opposite the operator’’ configuration for performing the block. The operator should consider the ergonomics of performing the block, which in this position does not require the operator to turn his or her head to get an adequate view of the screen. Ensure that the bed height and patient position are optimised (Figure 6).
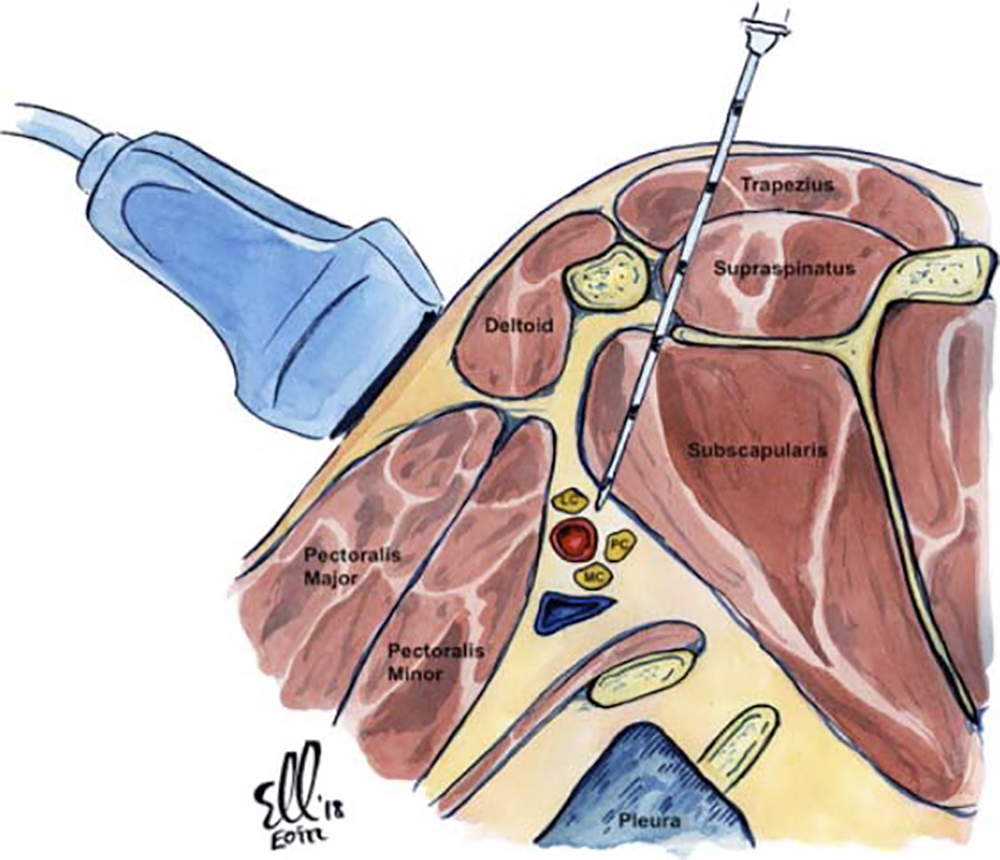
Figure 5. Illustration of the right infraclavicular brachial plexus with the needle inserted in plane with the ultrasound transducer. This is the retroclavicular approach to performing an infraclavicular brachial plexus block. Illustration supplied by Dr. Eoin Kelleher, Specialist Registrar in Anaesthesia, Mater Misericordiae University Hospital, Dublin, Ireland.
Preparation
- Prior to any instrumentation of the patient, perform a World Health Organization surgical safety check and a ‘‘stop before you block’’ checklist to reduce the risk of wrong-site block.11,12
- Ensure that consent is obtained, along with documentation of a detailed discussion of all risks and benefits pertaining to the IC-BPB for each patient. Identify any contraindications to performing an IC-BPB.
Performing the Block
The key anatomical structure to visualise when performing a US-guided IC-BPB is the axillary artery (Figure 3). It lies posterior to the pectoralis major and minor muscles. The lateral cord generally lies superior to the axillary artery, and the posterior and medial cords lie posteriorly and inferiorly to the axillary artery, respectively (Figure 5).
Orientating oneself in relation to the sonoanatomy and probe placement is important. The authors use the following orientation of the probe to the US image: on the US screen, with a left-sided IC-BPB, the top of the screen is superficial/anterior and the bottom of the screen is posterior; the right side of the screen is cephalad, and the left side of the screen is caudad (Figures 6 and 7).
The IC-BPB is a perivascular block; therefore, the aim is to deliver LA around 2 target areas. These targets areas are near the lateral cord and the medial and posterior cords, respectively (Figure 8).
- Clean and sterilise the infraclavicular area as per local departmental protocol.
- Place the transducer below the clavicle, medial to the coracoid process with the probe positioned in a parasagittal fashion (Figure 6).
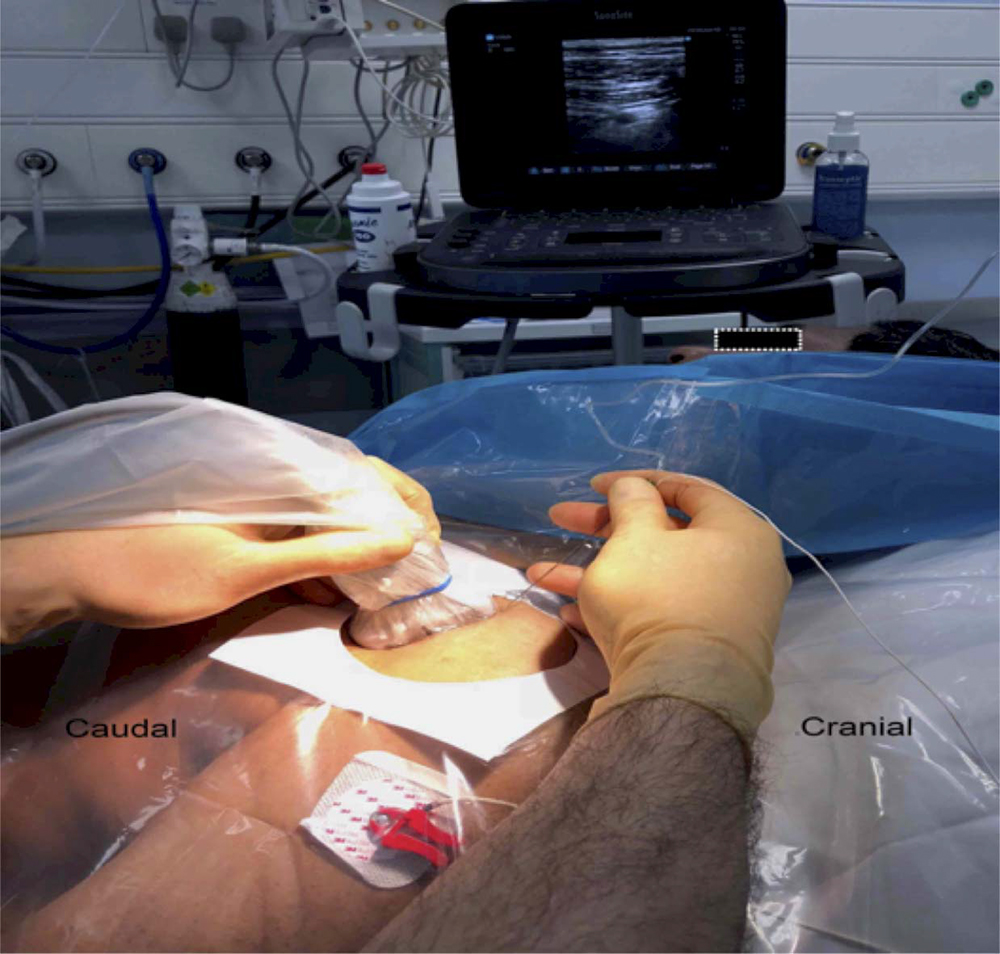
Figure 6. Suggested ‘‘opposite the operator’’ configuration for performing an IC-BPB. Note the supine position of the patient with patient comfort optimised. Note the optimisation of the ultrasound machine position and bed height to enhance the ergonomics of block performance. Image supplied by Dr. Georgi Valchev, Consultant Anaesthetist, Mater Misericordiae University Hospital, Dublin, Ireland.
- Identify the axillary artery, which lies posterior to the pectoralis major and minor muscles. The axillary artery is typically located at a depth of 3 to 4.5 cm. It is seen as a dark, round, pulsating structure with a hyperechoic wall (Figure 3). The axillary vein usually lies beside the artery (medially and inferiorly), and it very easily collapses with compression. Hence, additional attention should be paid to the vein to prevent inadvertent puncture of the vessel.
- A combination of 2-dimensional and colour Doppler will allow identification of arterial and venous anatomy and confirm their position.
- Be mindful that the brachial plexus in the infraclavicular region is deeper compared with other sites (≥4 cm), and the location of the cords around the axillary artery can vary significantly (Figure 2).
- The axillary artery is surrounded by 3 hyperechoic circular cords of the brachial plexus: the lateral, posterior, and medial cords. These have a honeycomb appearance.
- The lateral cord generally lies superior (cranial) to the axillary artery, and the posterior and medial cords lie posteriorly and inferiorly (cephalad) to the axillary artery, respectively (Figures 3 and 4).
- Place 2 mL of 1% to 2% lidocaine subcutaneously prior to placement of the block needle.
- Reconfirm the sonoanatomy with US and anchor the probe by placing your hand on the patient’s torso.
- Using an in-plane needle technique, from cephalad to caudad, visualise the needle throughout the performance of the block.
- Place the needle inferior to the clavicle and direct the needle inferiorly toward the posterior aspect of the axillary artery. The skin, subcutaneous tissue, pectoralis major, and pectoralis minor are penetrated en route toward the infraclavicular plexus (Figure 7).
- The angle of approach is very acute, which requires the direction of the needle to be quite steep. This will make concurrent visualisation of the needle and the surrounding anatomy challenging. A ‘‘heel-in’’ manoeuvre (as described below) may help to improve the view and allow more space on the skin below the clavicle to insert the needle (Figure 9).
- As the needle is advanced under US guidance, with a nerve stimulator connected with a stimulation current of 0.5 mA to 1 mA at 0.1 seconds, the lateral cord motor response will be manifested as elbow or finger flexion. Reducing the stimulating current to 0.2 mA with no motor manifestations of lateral cord response would deem it safe to begin deposition of LA in this location.
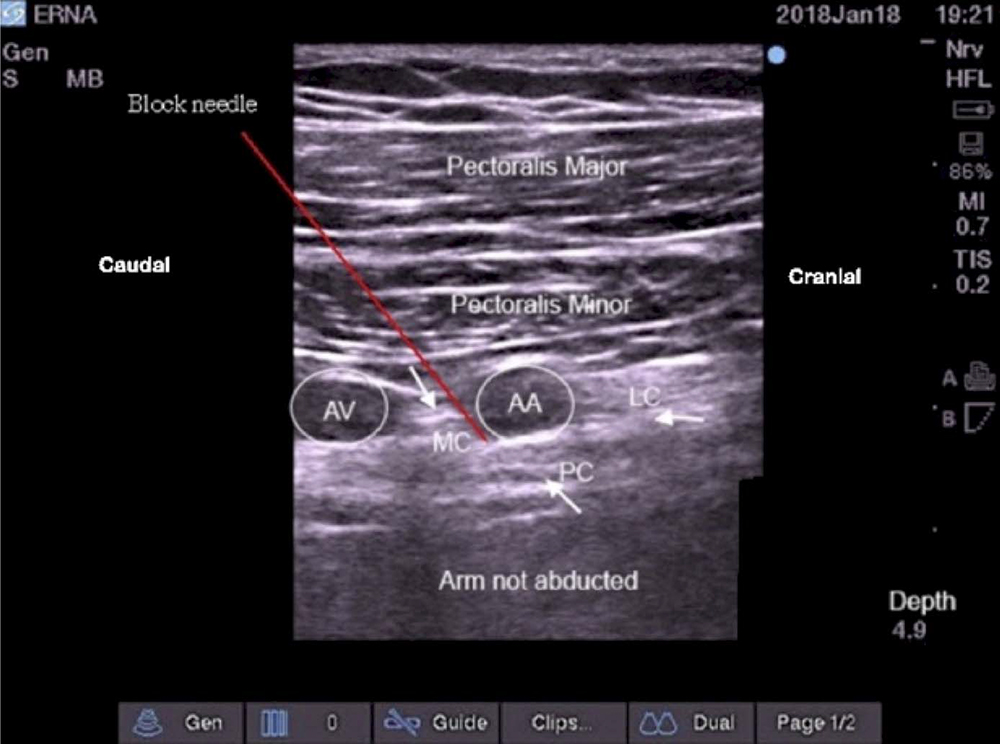
Figure 7. Ultrasound view of the left infraclavicular brachial plexus with the left arm not abducted. Orientation: right side of the screen is cephalad, left side opf the screen caudad. AA indicates axillary artery; AV, axillary vein; MC, medial cord; PC, posterior cord; LC, lateral cord. Image supplied by Dr. Georgi Valchev, Consultant Anaesthetist, Mater Misericordiae University Hospital, Dublin, Ireland.

Figure 8. U-shaped spread of local anaesthetic around the left axillary artery. The spread of local anaesthetic is targeted at the lateral, medial, and posterior cords. AA indicates axillary artery; AV, axillary vein; MC, medial cord; PC, posterior cord; LC, lateral cord; LA, local anaesthetic. Image supplied by Dr. Georgi Valchev, Consultant Anaesthetist, Mater Misericordiae University Hospital, Dublin, Ireland.

Figure 9. ‘‘Heel-in’’ positioning of the ultrasound probe to aid needle placement and advancement when performing an infraclavicular brachial plexus block. Image supplied by Dr. Georgi Valchev, Consultant Anaesthetist, Mater Misericordiae University Hospital, Dublin, Ireland.
- Further advancement of the needle posteriorly will elicit a motor response of the posterior cord, manifested as finger and wrist extension. Reducing the stimulating current to 0.2 mA with no motor manifestations of the posterior cord response would deem it safe to begin deposition of LA in this location.
- A suggested approach would be to inject LA (two-thirds of the volume) posterior to the axillary artery around the posterior and medial cords (the deeper cords) and redirect the needle toward the lateral cord (more superficial) during retraction of the needle and inject the remaining LA (one-third of the volume). The aim is to achieve the desired ‘‘U-shaped’’ crescentic distribution of LA around the artery (Figure 8).
- Deposit LA in 5-mL aliquots followed by aspiration to decrease the risk of intravascular injection.
Note
The ‘‘heel-in’’ manoeuvre consists of the following: on the US probe, the caudal end of the transducer is labelled as the ‘‘heel,’’ and the cranial end is labelled as the ‘‘toe.’’ Pressing only the heel end of the transducer deeply into the patient and not the toe end is helpful in changing the US image of the needle and improves needle visualisation. It also helps by providing more skin area for needle entry for the block (Figure 9). Be mindful that a steeper angle may increase the risk of pleural puncture and pneumothorax, as the visibility of the needle tip is reduced the deeper it goes.
TIPS FOR PERFORMING IC-BPB
- Beaware of the acoustic enhancement of the axillary artery posteriorly. This may result in misinterpretation of the position of the posterior cord.
- Improvedvisualisation of the cord may be achieved when the patient’s arm is abducted at 90°. This will allow superior movement of the acromioclavicular joint and reduce the depth of plexus from the skin (this will bring the plexus more superficial and aid with needle trajectory; Figures 7 and 8).
- Considerationshould be given to using a curved array probe if the location of the plexus is deeper than 5 cm.
- Theuse of a nerve stimulator with US may help with block performance.
- Usingan echogenic needle will aid needle-tip visualisation.
Alternative Techniques for US IC-BPB
The RAPTIR uses a US probe position that is similar to that of the classical technique. The point of needle insertion, however, is over the trapezius muscle posteriorly. This approach allows the needle to pass between the scapula and the clavicle toward the axillary artery13,14 (Figures 5 and 10).
With the patient in the supine position, the probe is placed in a parasagittal position below the clavicle as described above. Locate the axillary artery as it exits from under the clavicle. The block needle is placed 2 cm posterior to the clavicle and in a parallel angle with the probe. A ‘‘blind zone’’ is located below the clavicle. The needle is not visualised in this zone for 2 to 3 cm (Figure 10).
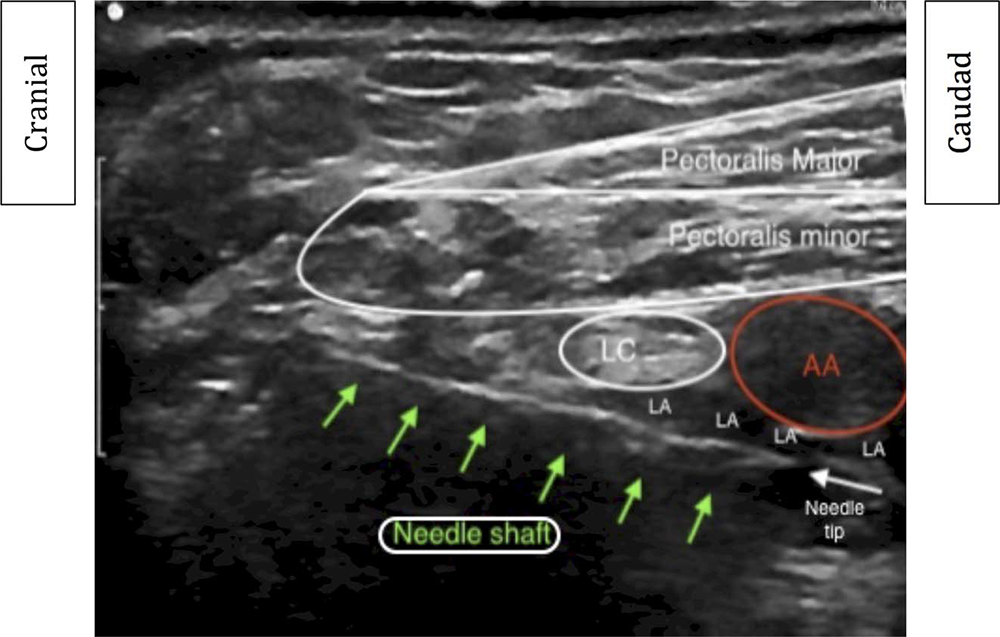
Figure 10. Ultrasound view of the right infraclavicular brachial plexus (retroclavicular approach). The green arrows indicate the location of the ultrasound needle in relation to the lateral cord and the axillary artery. AA indicates axillary artery; LC, lateral cord; LA, local anaesthetic. Image supplied by Dr. Steve Copens, Consultant Anaesthetist, UZ Leuven, Belgium.
The benefit of the RAPTIR over the classical IC-BPB is improved needle visualisation closer to the cords. There is a risk of injury to the suprascapular neurovascular bundle and the posterior cord and a risk of causing a pneumothorax, which is postulated to be lower than with the traditional parasagittal approach.13,14 Contraindications to the RAPTIR include short neck, any clavicular deformity, and prominent pectoral muscles. Of note, blockade of the musculocutaneous nerve may be very difficult to achieve with the RAPTIR. The RAPTIR does not require the patient to abduct his or her arm. If it is technically difficult to perform the IC-BPB in the infraclavicular groove, performing the RAPTIR should be considered.
CONTINUOUS IC-BPB
The infraclavicular fossa is an ideal location for placement of a catheter for continuous postoperative analgesia to the elbow, forearm, wrist, and hand. The musculature of the chest wall secures the catheter. The depth of the IC-BPB (≥4 cm) generally averts its dislodgment.
Performing a continuous IC-BPB involves 3 steps: (1) needle positioning, (2) catheter placement, and (3) securing the catheter. The catheter is placed under direct US guidance. Similar to the single-shot technique as described in this tutorial, the needle tip should be placed posterior to the axillary artery and therefore the catheter ideally located beneath the axillary artery. Hydrodissection with LA or normal saline (0.9% NaCl) prior to catheter advancement may help with threading the catheter. At our institution, we confirm the catheter tip position by observing the posterior spread of LA or 0.9% NaCl around the axillary artery. This may also be performed by nerve stimulation of the posterior cord.
It is important to ensure stability of the needle during catheter advancement. Resting the needling hand against the patient’s chest will provide additional stability and may help avoid inadvertent needle tip migration. The ideal location of the catheter tip is 2 to 3 cm from the needle tip. This will allow the catheter to be in close vicinity to the posterior and medial cord and facilitate spread of LA around the cords. A typical LA infusion regimen used in the authors’ institution is 5 mL of 0.125% levobupivacaine per hour. A patient-controlled bolus of 5 mL can be performed with a lockout time of 60 minutes. The catheter should be taped to the skin with an appropriate adhesive material or tunnelled under the subcutaneous tissue. The catheter is secured using a clear adhesive dressing on the anterior chest wall to avoid dislodgement.
REFERENCES
- Chin KJ, Alakkad H, Adhikary SD, et al. Infraclavicular brachial plexus block for regional anaesthesia of the lower arm. Cochrane Database Syst Rev. 2013;28(8):CD005487.
- Kilka HG, Geiger P, Mehrkens HH. Infraclavicular vertical brachial plexus blockade. A new method of anesthesia of the upper extremity. An anatomical and clinical study. Anaesthesist. 1995;44(5):339-344
- Raj PP, Montogmery SJ, Nettles D, et al. Infraclavicular brachial plexus block—a new approach. Anesth Analg. 1973;52(6):897-903.
- Koscielniak-Nielsen ZJ, Rasmussen H, Hesselbjerg L, et al. Clinical evaluation of the lateral sagittal infraclavicular block developed by MRI studies. Reg Anesth Pain Med. 2005;30(4):329-334.
- Borgeat A, Ekatodramis G, Dumont C. An evaluation of the infraclavicular block via a modified approach of the Raj technique. Anesth Analg. 2001;93(2):436-441.
- Dingemans E, Williams SR, Arcand G, et al. Neurostimulation in ultrasound-guided infraclavicular block: a prospective randomized trial. Anesth Analg. 2007;104(5):1275-1280.
- Sandhi NS, Capan LM. Ultrasound-guided infraclavicular brachial plexus block. Br J Anaesth. 2002;89(2):254-259.
- Mariano ER, Loland VJ, Bellars RH, et al. Ultrasound guidance versus electrical stimulation for infraclavicular brachial plexus perineural catheter insertion. J Ultrasound Med. 2009;28(9):1211-1218.
- Petrar SD, Seltenrich ME, Head SJ, Schwarz SK. Hemidiaphragmatic paralysis following ultrasound-guided supraclavicular versus infraclavicular brachial plexus blockade: a randomized clinical trial. Reg Anesth Pain Med. 2015;40:133-138.
- Gadsden JC, Choi JJ, Lin E, et al. Opening injection pressure consistently detects needle-nerve contact during ultrasound-guided interscalene brachial plexus block. Anesthesiology. 2014;120(5):1246-1253.
- Association of Anaesthetists of Great Britain and Ireland. Recommendations for standards of monitoring during anaesthesia and recovery. December 2015. Report No. 1. 9 November 2018. https://www.aagbi.org/sites/default/files/ Standards_of_monitoring_2015_0.pdf.
- Royal College of Anaesthetists. Wrong site block. https://www.rcoa.ac.uk/standards-of-clinical-practice/wrong-site-block. Accessed November 8, 2018.
- Beh ZY, Hasan MS, Lai HY, et al. Posterior parasagittal in-plane ultrasound-guided infraclavicular brachial plexus block— a case series. BMC Anesthesiol. 2015;15:105.
- Luftig J, Mantuani D, Herring AA, Nagdev A. Ultrasound-guided retroclavicular approach infraclavicular brachial plexus block for upper extremity emergency procedures. Am J Emerg Med. 2017;35(5):773-777.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/