Regional Anaesthesia

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article.
- Which of the following statements is correct?
- At the elbow the median nerve can be viewed lateral to the brachial artery
- The ulnar nerve should be blocked at the elbow
- At the elbow, the radial nerve sits between the brachioradialis and brachialis muscles
- In the forearm, the ulnar nerve sits medial to the ulnar artery
- Name three muscles that the ulnar nerve supplies.
- What movement can be elicited in the wrist or hand with stimulation of the following nerves?
- Median
- Ulnar
- Radial
INTRODUCTION
Using ultrasound-guidance, the median and ulnar nerves can be easily blocked in the forearm and the radial nerve just above the elbow. These blocks are commonly used to provide analgesia following hand surgery, or to augment or expedite a more proximal brachial plexus block. The purely sensory medial, lateral and posterior cutaneous nerves of the forearm can also be blocked at the elbow using ultrasound. Nerve stimulators can be used to confirm nerve identification, though be aware that there are wide variations in nerve sensitivities when placing needle-tips in contact with nerves.
INNERVATION OF THE ARM
Figure 1 shows the cutaneous innervation of the arm. Table 1 details the motor responses elicited when stimulating the nerves of the forearm.
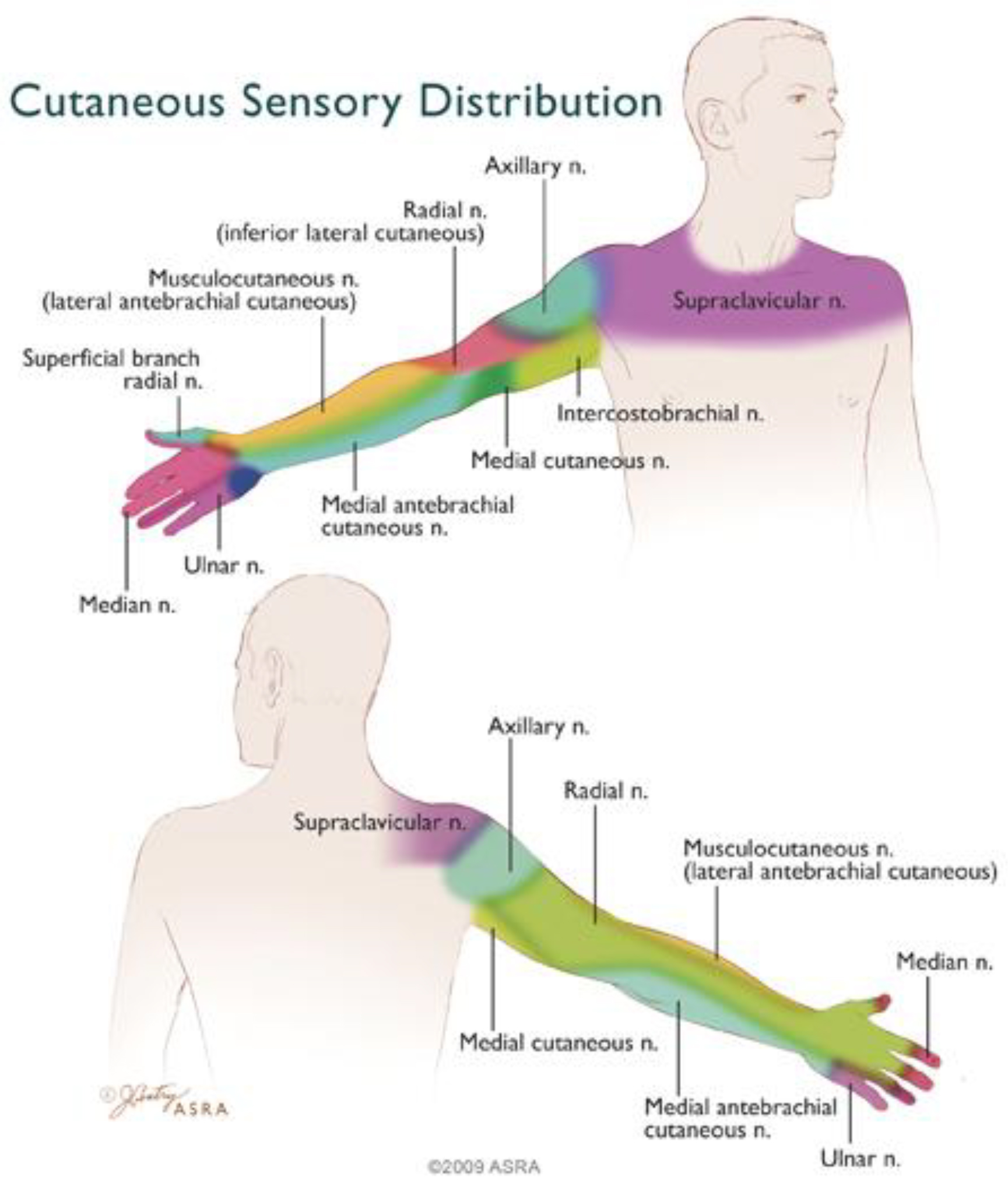
Figure 1: Cutaneous innervation of the arm (ASRA 2009)
Copyright 2009 American Society of Regional Anesthesia and Pain Medicine. Used with permission. All rights reserved. Use of this image does not constitute or imply endorsement by ASRA of the website or material on which it appears or the product or service provided
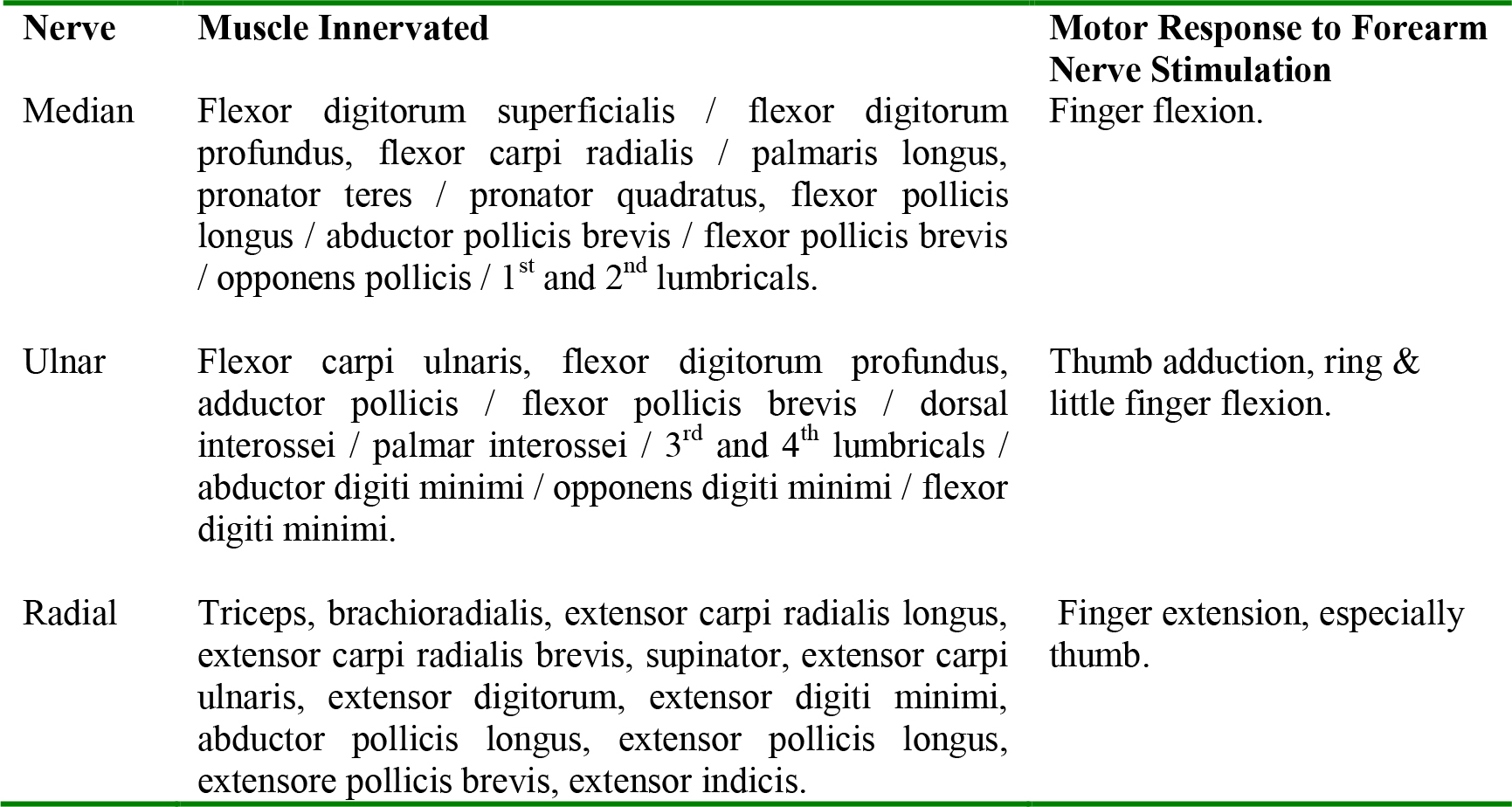
Table 1: Elicited motor response for upper limb nerves (modified from Nicholls 2008)
MEDIAN NERVE
Anatomy
The median nerve is formed from medial and lateral cords of brachial plexus.
Passes into forearm between the heads of pronator teres.
Its palmar cutaneous branch, passes beneath the flexor retinaculum before it gives branches to the thenar eminence, lateral hand, abductor pollicis brevis, flexor pollicis brevis, opponens pollicis and 1st and 2nd lumbricals
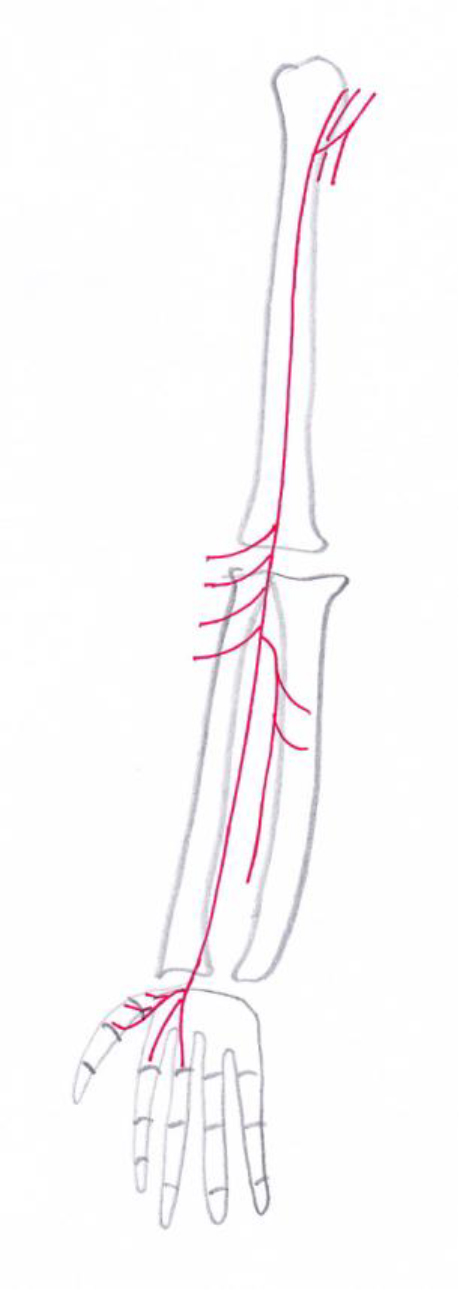
Figure 2: Course of the median nerve
Gives branches to pronator teres, flexor carpi radialis, palmaris longus and flexor digitorum superficialis
Its branch the anterior interosseous nerve supplies flexor digitorum profundus (radial half only), flexor pollicis longus and pronator quadratus
In the forearm the median nerve lies between flexor digitorum superficialis and profundus
Its palmar cutaneous branch, passes beneath the flexor retinaculum before it gives branches to the thenar eminence, lateral hand, abductor pollicis brevis, flexor pollicis brevis, opponens pollicis and 1st and 2nd lumbricals
Performing a median nerve block
Basic median nerve anatomy is shown in Figure 2. At the elbow, the median nerve can be viewed medial to the brachial artery, deep to the basilic vein but superficial to the medial epicondyle. In the forearm, the median nerve can be viewed medial to the radial artery and the radius.
Place the ultrasound probe on the anterior surface of the forearm, either at the antecubital fossa or more distally and view the median nerve in axial section. The nerve will be seen as a single elliptical hyperechoic structure with internal hypoechoic circles (Figure 3). Adjust the angle of the probe until the best image of the median nerve is obtained.
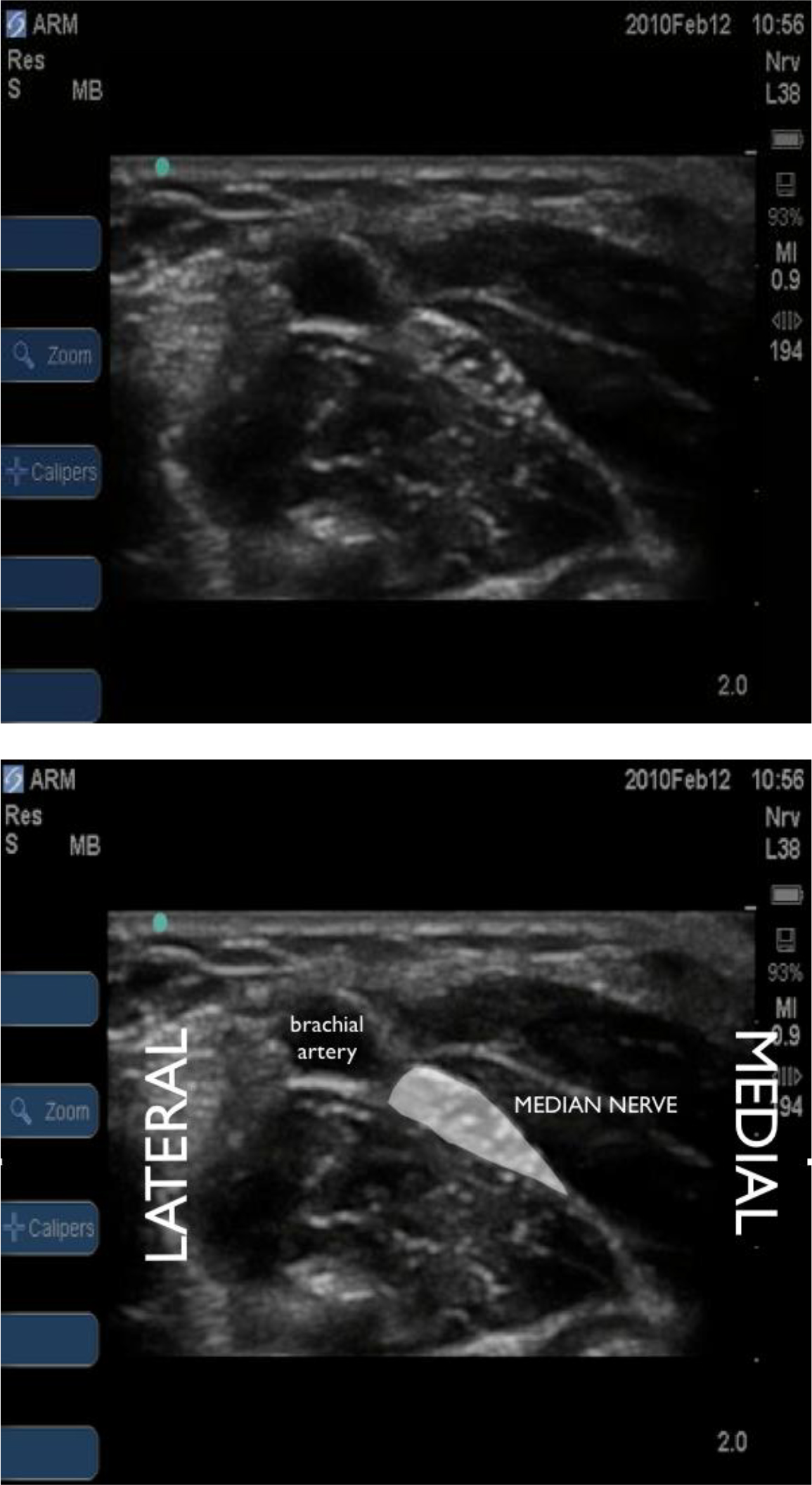
Figure 3: Ultrasound view of median nerve just distal to antecubital fossa. Nerve lies medial and deep to brachial artery.
Insert the needle in-plane from the radial side of the probe. One can use a nerve stimulator to aid positioning of needle-tip in proximity to the median nerve but beware variable nerve sensitivities and loose connections! As the needle-tip is visualised adjacent to the nerve, aspirate and inject local anaesthetic. Look for spread around the circumference of the nerve and reposition as necessary to ensure this. It is easiest to block the median nerve mid-forearm (Figure 4) where there are rarely any adjacent vascular structures.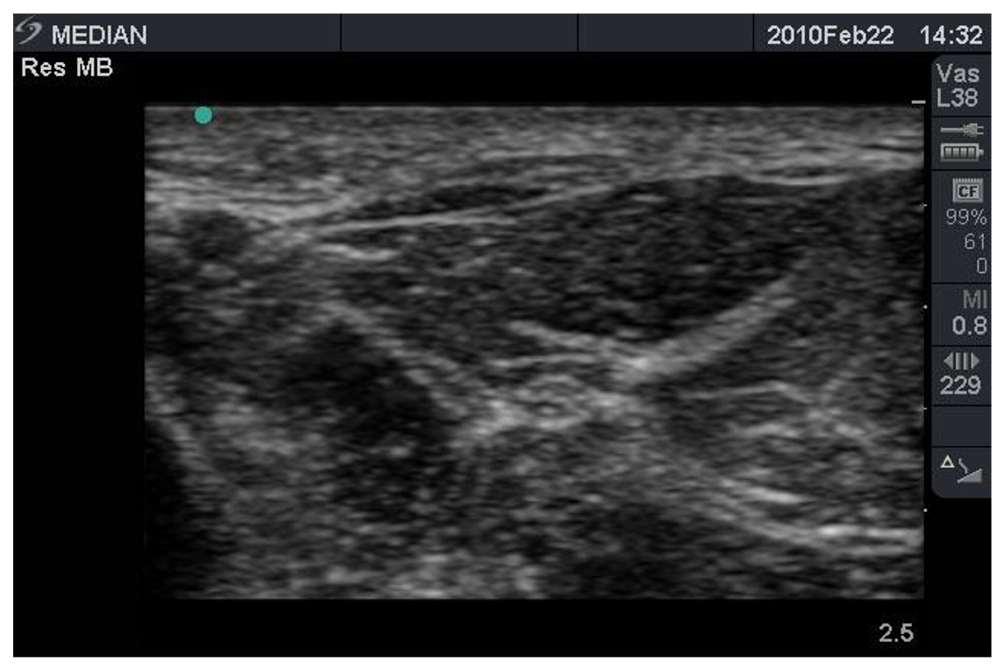

Figure 4: Ultrasound view of median nerve at mid-forearm level.
The median nerve can also be visualised at the wrist (Figure 5) and tracked proximally. If using the in-plane technique, check medially and laterally to ensure that your needle does not pass through either radial or ulnar vessels or nerves (more likely with longer, shallower needle paths). Table 2 details the local anaesthetic, needle and motor stimulation end-point for a median nerve block.

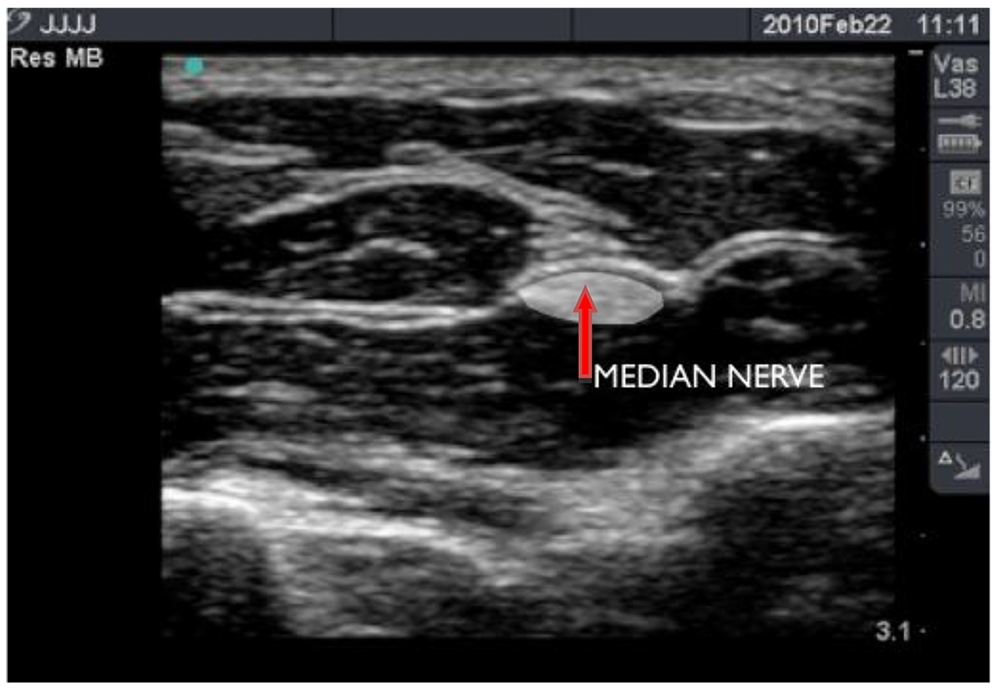
Figure 5: Ultrasound view of median nerve at wrist.

Table 2: Median nerve block
ULNAR NERVE
Anatomy
The ulnar nerve is formed from the medial cord of brachial plexus
Lies behind the medial epicondyle and passes into the forearm between the heads of flexor carpi ulnaris
Gives branches to flexor carpi ulnaris and half of flexor digitorum profundus
Its dorsal branch supplies the medial part of dorsum of the hand
Its palmar cutaneous branch supplies the skin on the medialside of the hand and the nails of the 4th and 5th fingers
Gives branches to adductor pollicis, flexor pollicis brevis, 1st dorsal interosseus, 1st palmar interosseus, 3rd and 4th fourth lumbrical, and hypothenar muscles (opponens digiti minimi, abductor digiti minimi,flexor digiti minimi brevis)
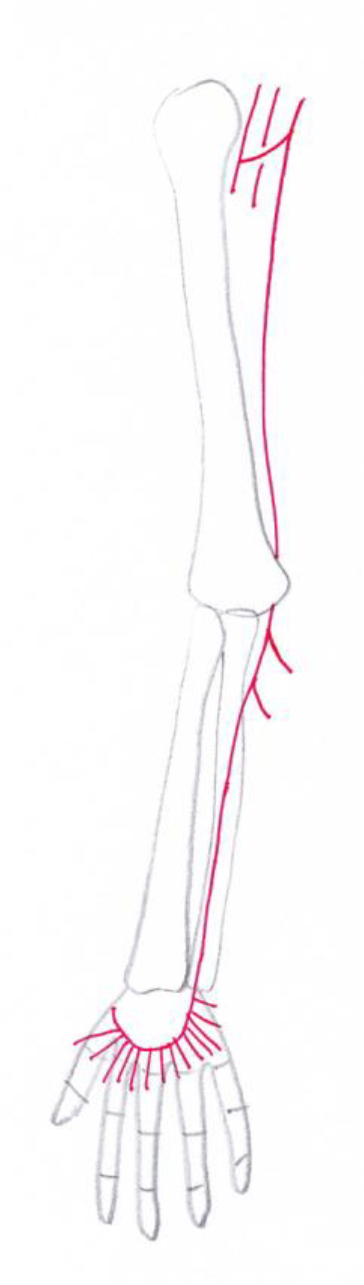
Figure 6: Course of the ulnar nerve
Performing an ulnar nerve block
Basic anatomy of the ulnar nerve is demonstrated in Figure 6. The ulnar nerve should not be blocked at the level of the elbow due to the risk of ischaemia. At this level it lies in the groove between the olecranon and medial epicondyle and the addition of local anaesthetic into this groove may result in high pressures causing nerve ischaemia. It should therefore be blocked either proximal or distal to the elbow.
Distal to the elbow, the ulnar nerve can be viewed on the medial/ulna side of the forearm (Figures 7, 8 and 9). It is easiest to find the ulnar artery first at the wrist, then identify the ulnar nerve lying medial to it. Place the probe on the anterior surface of the forearm and adjust the angle of the probe until the best image of the nerve is obtained. Trace the nerve proximally until the nerve becomes separate from the ulnar artery and perform the block here to minimise risk of vascular puncture.
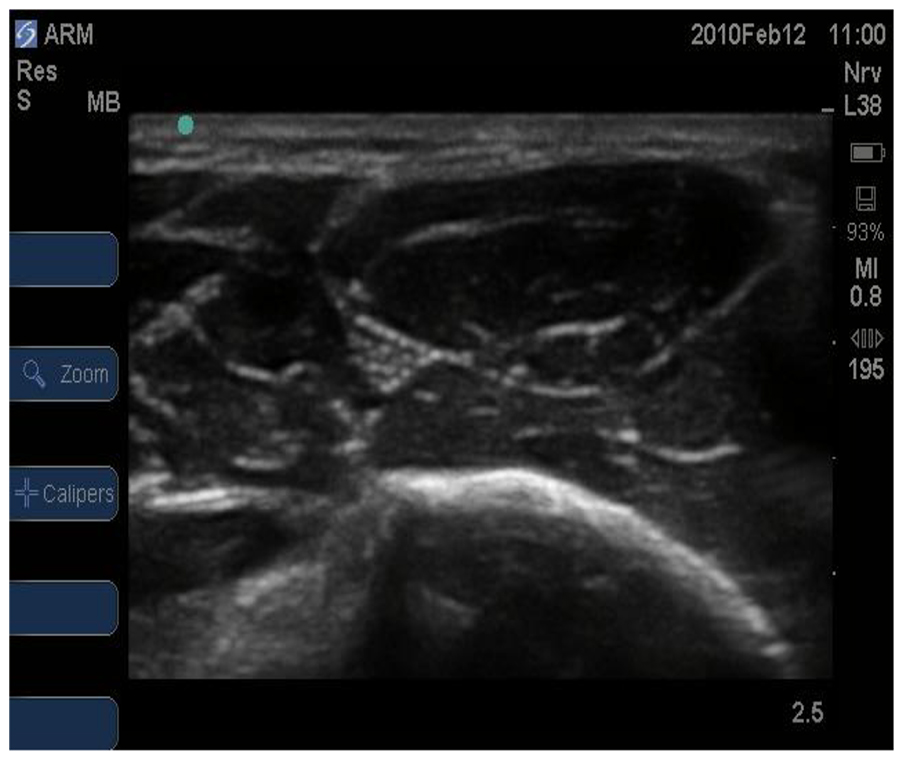

Figure 7: Ultrasound view of ulnar nerve 5cm distal to elbow
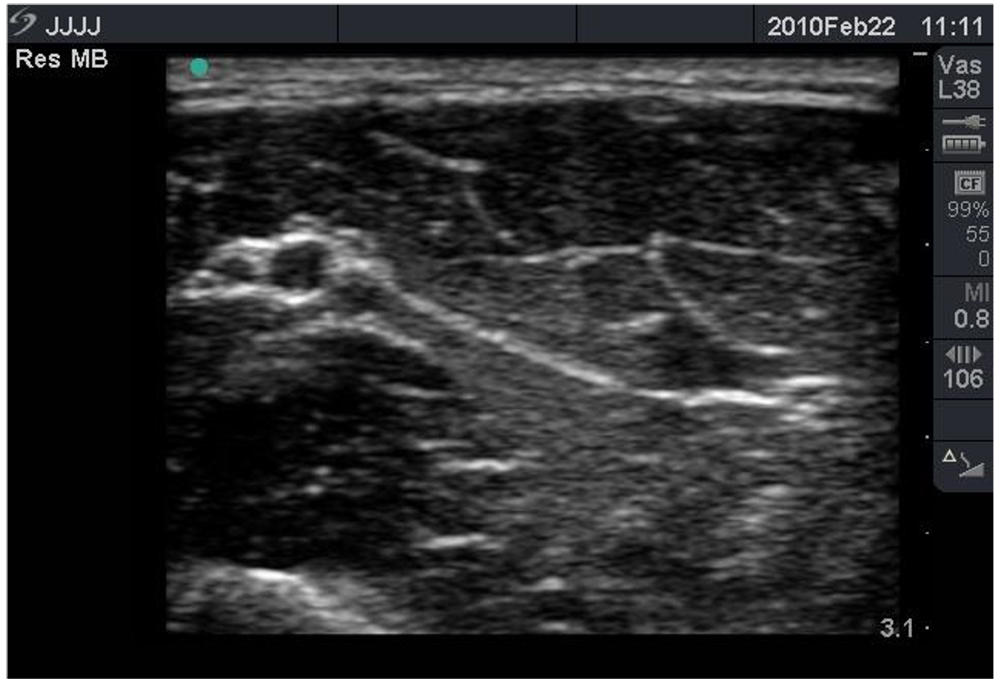

Figure 8: Ultrasound image of distal forearm showing ulnar nerve medial to ulnar artery.
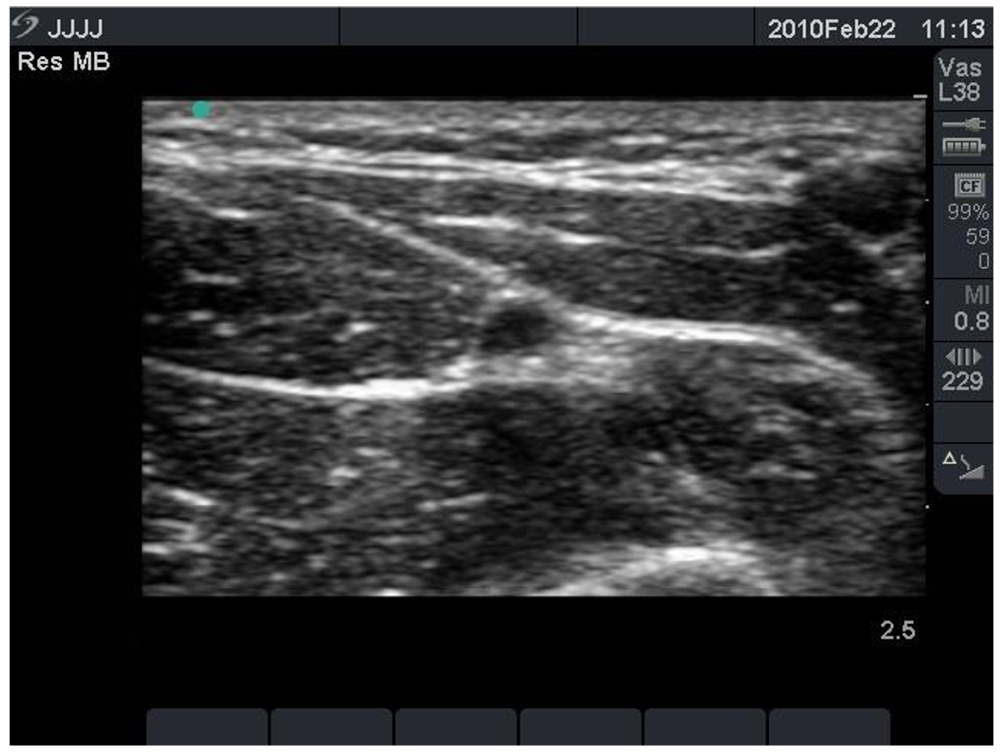
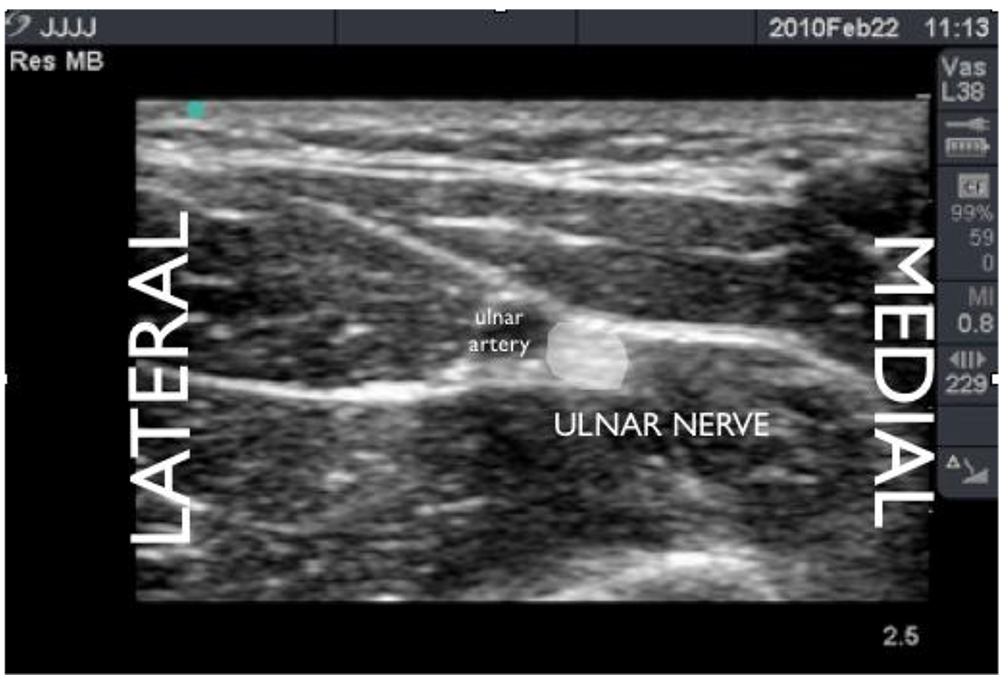
Figure 9: Ultrasound view of distal forearm showing ulnar nerve medial to ulnar artery.
An in-plane approach is advised. A nerve stimulator can also be used in with the ultrasound to confirm identity of the nerve. Position the needle-tip adjacent to nerve (Figure 10). Following negative aspiration, inject the local anaesthetic. Look for spread around the circumference of the nerve and reposition as necessary to achieve this. See Table 3 for details of LA and desired muscle twitch.

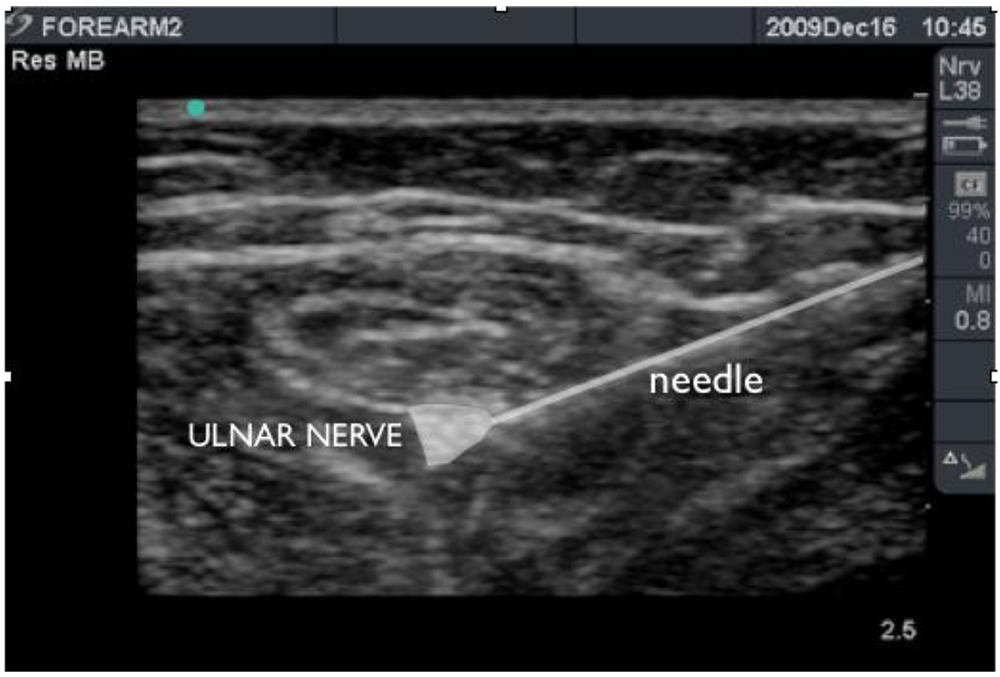
Figure 10: Needle positioned adjacent to ulnar nerve prior to injection of local anaesthetic 5cm distal to elbow.
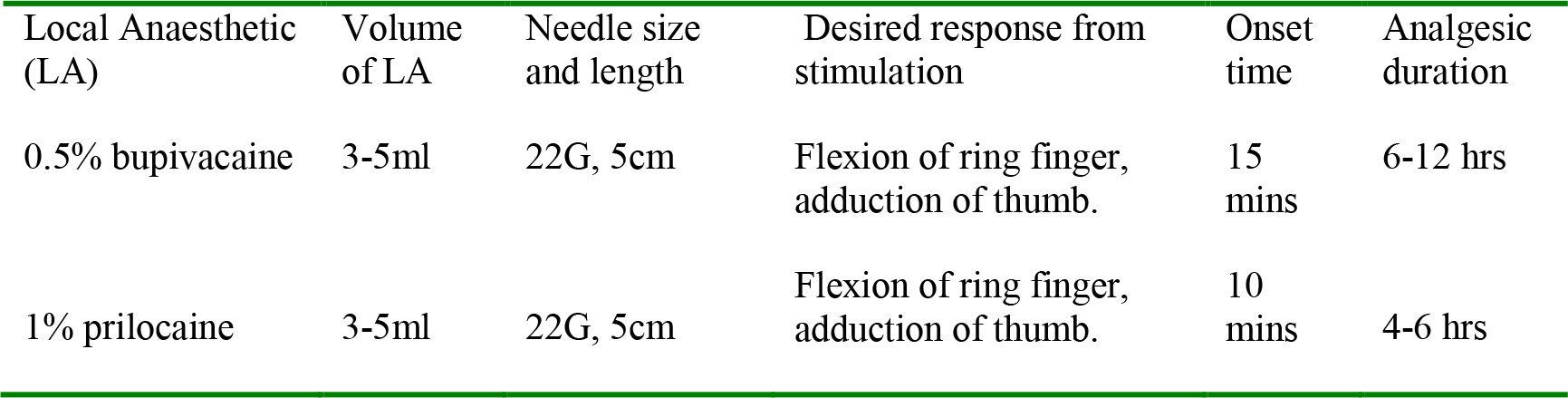
Table 3: Ulnar nerve block
RADIAL NERVE
Anatomy
The radial nerve is formed from posterior cord of the brachial plexus.
Gives branches to triceps before entering spiral groove in the arm Lies between brachioradialis and brachialis at elbow
Gives off superficial and deep terminal branches
Gives branches to brachioradialis and extensor carpi radialis
Its deep branch becomes the posterior interosseus nerve which supplies the extensor compartment
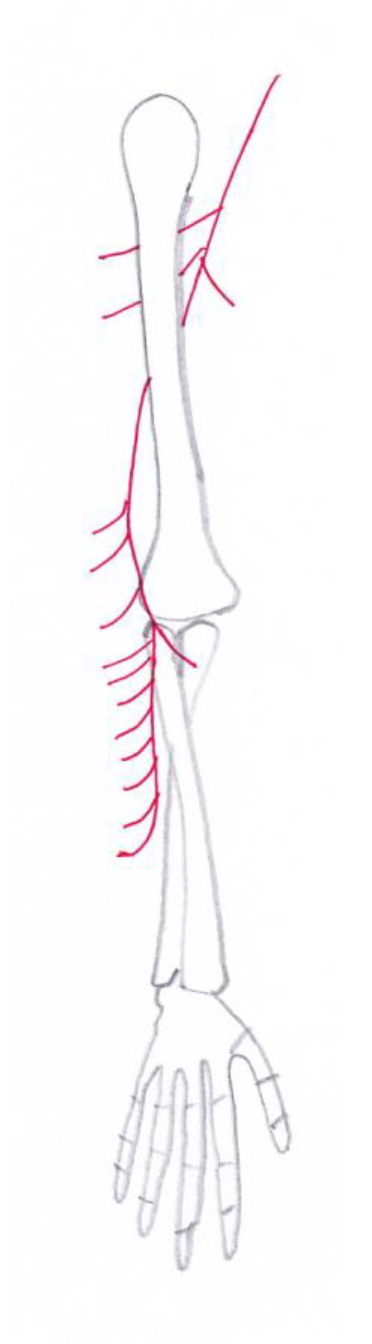
Figure 11: Course of the radial nerve
The posterior cutaneous nerve of forearm arises in from the radial nerve in spiral groove
Its superficial branch supplies skin on lateral dorsum of hand over thumb, index and middle fingers.
Performing a radial nerve block
Radial nerve anatomy is shown in Figure 11. Blockade of the radial nerve is not normally performed in the forearm. The block is ideally performed proximal to the elbow before the nerve has divided. At the elbow, the radial nerve (Figures 12 and 13) can be viewed as an elliptical structure that divides into superficial and deep branches. It sits superficial to the humerus, between the brachioradialis and brachialis muscle. It divides into superficial and deep branches proximal to the elbow. Below the elbow, the deep branch is seen lying immediately superficial to the radius.
Place the ultrasound in the antecubital fossa and scan lateral and proximal. Adjust the angle of the probe until the best image of nerve is obtained. One can use a nerve stimulator but high stimulation currents may be required. Insert the needle in-plane from either side of the arm (Figure 14). When the needle-tip is seen next to the nerve, aspirate and inject the local anaesthetic, looking for spread around the circumference of the nerve and repositioning as necessary. See Table 4 for details of LA and desired twitch.
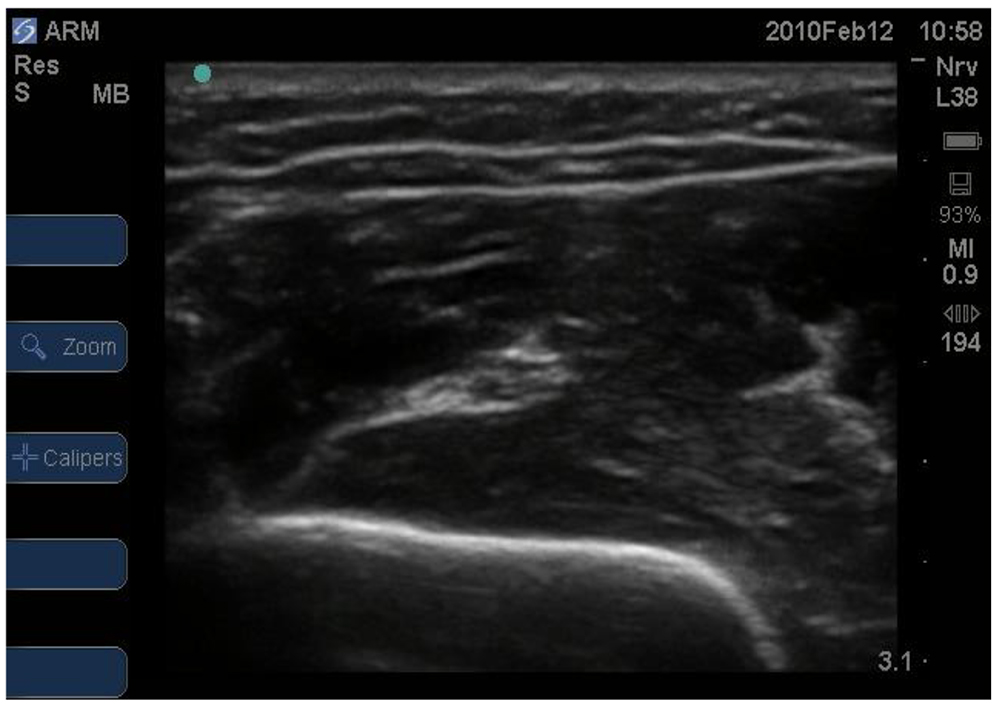
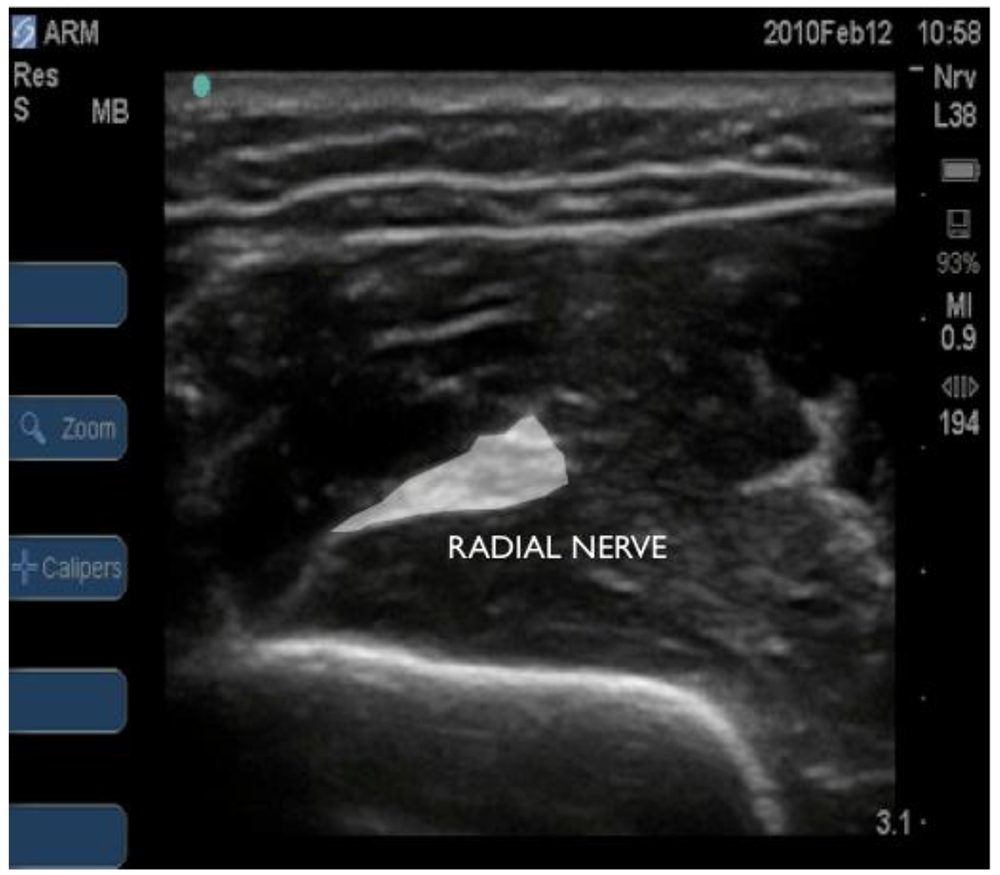
Figure 12: Ultrasound view of radial nerve just proximal to elbow. Deep and superficial branches not obvious.
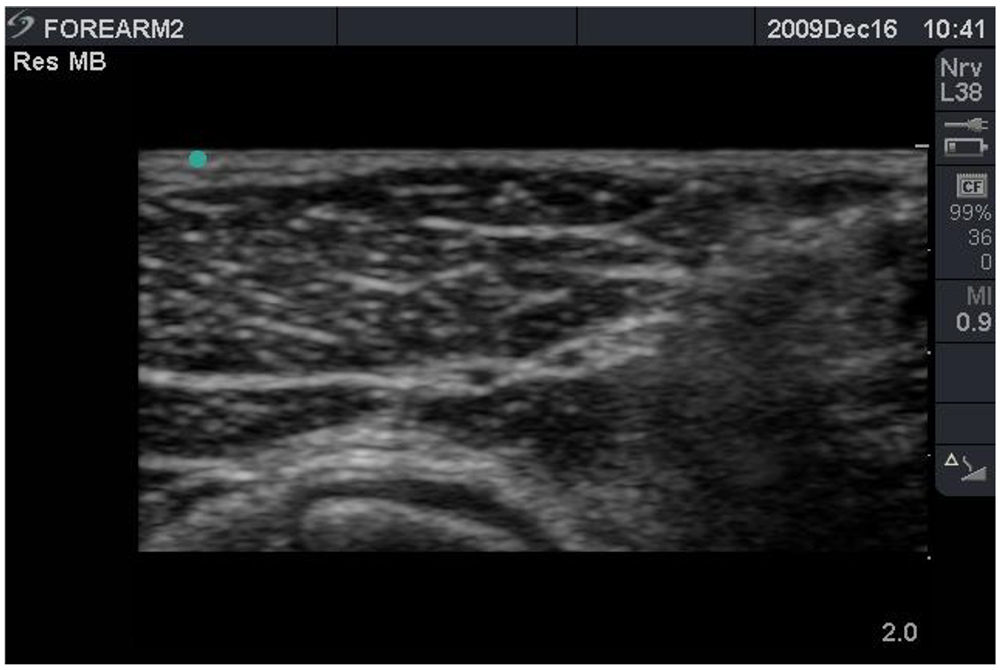
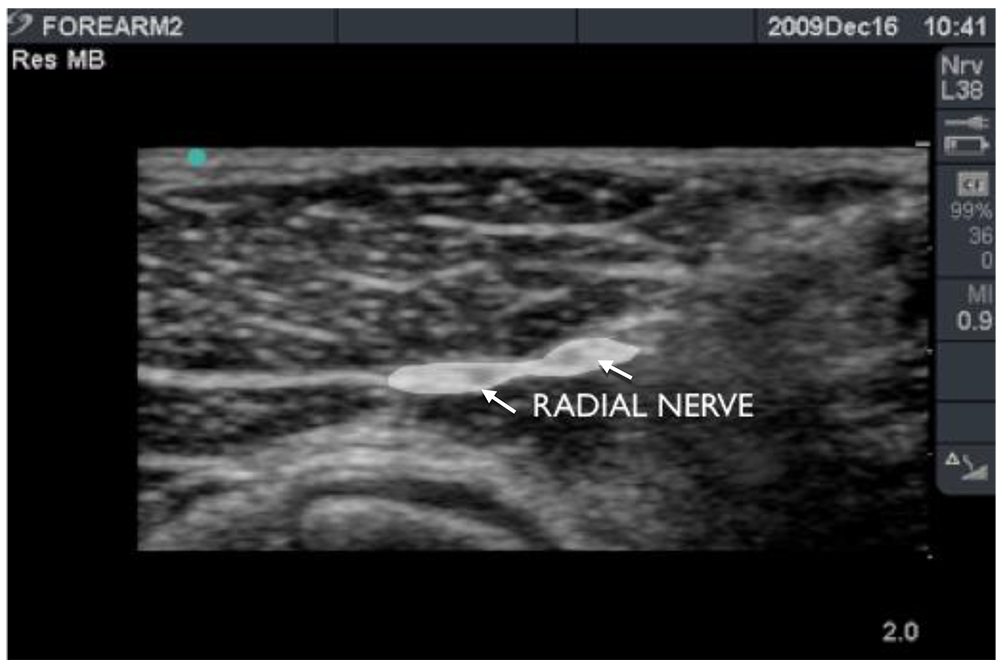
Figure 13: Ultrasound view of radial nerve (arrows) just proximal to elbow. Radial nerve can be seen to have divided. An effective block can still be achieved so long as LA surrounds both branches of the nerve.

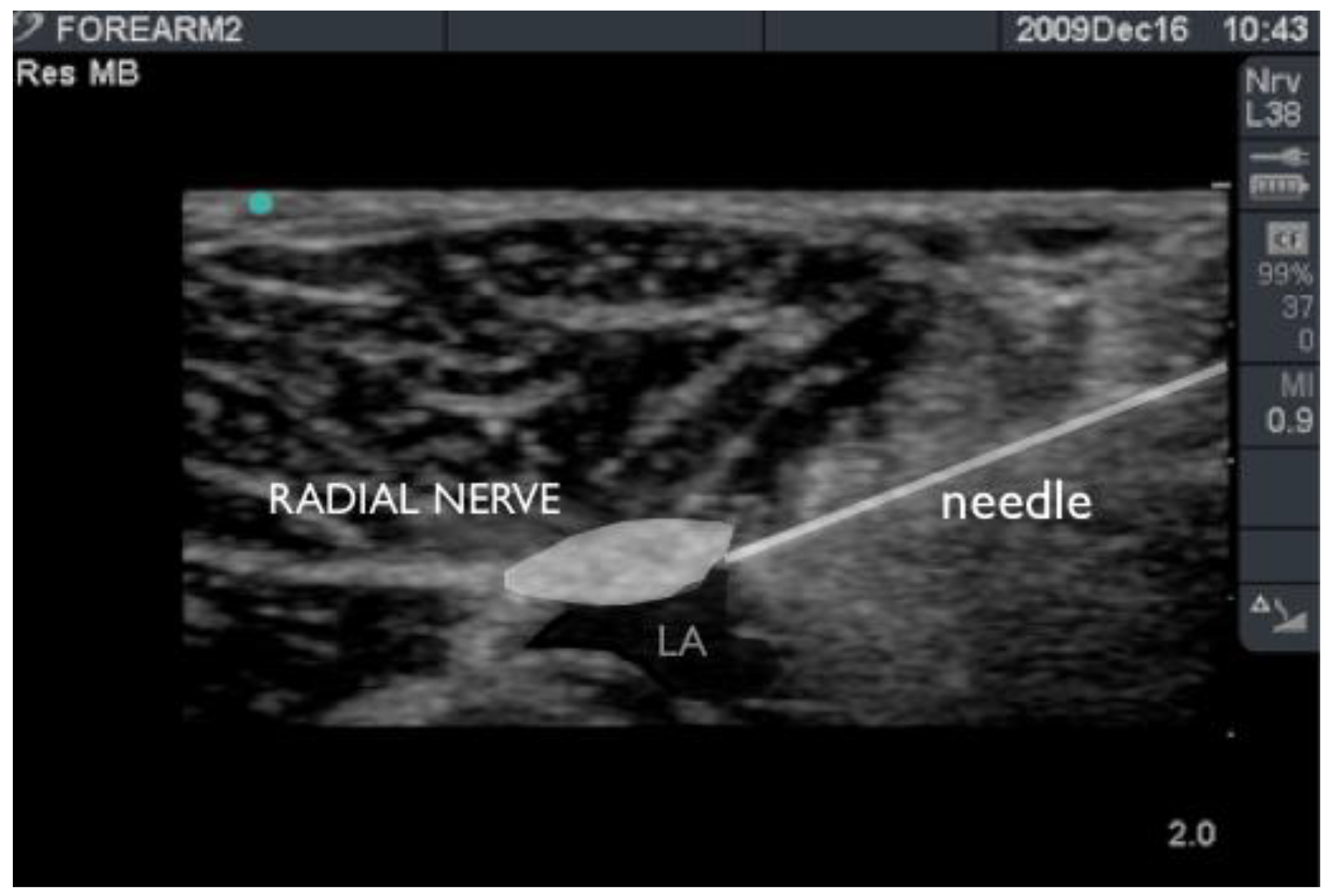
Figure 14: Needle-tip adjacent to radial nerve just proximal to elbow. Hypoechoic local anaesthetic spread (LA) can be seen deep to the nerve.
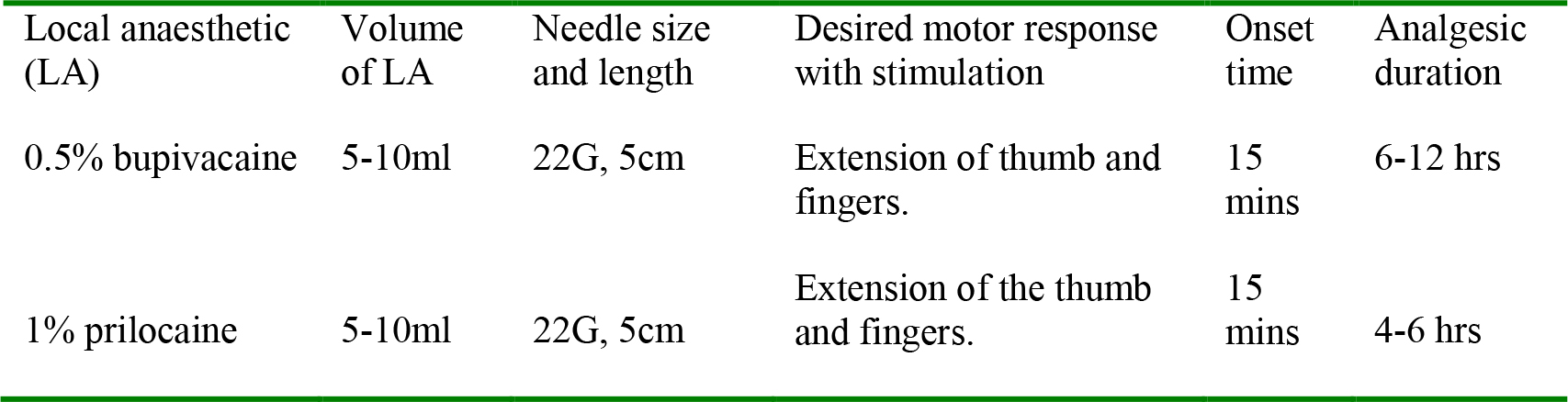
Table 4: Radial nerve block
OTHER NERVES
To block the medial cutaneous nerve of the forearm, local anaesthetic is injected superficially between the head of pronator teres and the biceps tendon.
The musculocutaneous nerve gives rise to the lateral cutaneous nerve of the forearm which is blocked by a subcutaneous injection of local anaesthetic between the biceps tendon and brachioradialis.
The posterior cutaneous nerve of the forearm is a branch of the radial nerve. It is blocked by a subcutaneous injection of local anaesthetic between the lateral epicondyle of the humerus and the olecranon.
Ultrasound may be used to aid muscle, tendon and bony landmark identification.
OUR EXPERIENCE
- We keep the screen in front of us during each procedure (Figure 15).
- We perform forearm blocks in awake and anesthetised patients.
- All nerves can be blocked with as little as 1ml of 0.5% bupivacaine or levobupivacaine but generally we use enough to surround the nerve (usually 5-8ml) to guarantee anaesthesia of the nerve.
- We use 20ml syringes for all our injections so as to appreciate different resistances more consistently. Although judging resistance is very subjective, if resistance to injection is high, then the needle tip may be intrafascicular risking nerve injury.
- We use 22G 5cm peripheral nerve block needles for all our injections allowing easy manipulation of the needle with the syringe attached via extension tubing and potentially less risk of nerve penetration due to the short bevel.
- We use the in-plane approach for all three major nerves as it is relatively straightforward.
- Initial injections should be only 0.5-1ml. We first aspirate and inject only if there is little resistance. If the nerve is seen on US to increase in size, the patient experiences paraesthesia or both then we stop injecting, withdraw the needle and start again. This is to try to reduce the risk of nerve damage due to intraneural injection, although of course the damage may have already been done.
- All nerves can be blocked with as little as 1ml of 0.5% bupivacaine or levobupivacaine but generally we use enough to surround the nerve (usually 5-8ml) to guarantee anaesthesia of the nerve.
- We do not routinely use the nerve stimulator due to the easily identified anatomy.
- We do not place catheters in forearm blocks because post-operative pain beyond the duration of a single shot block does not appear to be a major problem. If required however we place catheters at the infraclavicular site as this is well away from the surgical site.
- Our surgeons request an upper arm tourniquet so we usually perform a low dose supraclavicular block with 10ml of 1% prilocaine or 1% lidocaine, or use a Bier’s block or general anaesthetic depending on the clinical situation. The patient then regains use/control of their elbow within a few hours while the forearm blocks using the longer acting LA provide prolonged post-operative analgesia at the surgical site.

Figure 15: Operator-patient-scanner set-up for in-plane approach to the median nerve in the forearm.
SUMMARY
The three main nerves of the forearm – median, radial and ulnar – can easily be blocked using ultrasound-guidance with or without nerve stimulation. An in-plane needle approach is recommended. The volume of local anaesthetic required is usually 5-8ml per nerve. Circling the nerve with local anaesthetic gives the greatest chance of block success. Skilled performance of these blocks offers the potential for excellent post-operative analgesia for patients undergoing hand surgery.
Remember:
- A sound knowledge of neuroanatomy is essential in choosing which nerves to block based on the surgical site.
- The ulnar nerve should be blocked above or below the elbow, but never at the elbow where there is a risk of pressure-related nerve injury.
- The radial nerve should be blocked before it divides.
ANSWERS TO QUESTIONS
- Which of the following statements is correct?
- F At the elbow the median nerve can be viewed medial to the brachial artery.
- F The ulnar nerve should not be blocked at the elbow as this risks pressure-induced nerve injury due to the confined space of the ulnar groove.
- T
- T
- The ulnar nerve supplies flexor carpi ulnaris, flexor digitorum profundus, adductor pollicis, flexor pollicis brevis, dorsal interossei, palmar interossei, 3rd and 4th lumbricals, abductor digiti minimi, opponens digiti minimi and flexor digiti minimi.
- What movement can be elicited with stimulation of the following nerves?
- Median – Finger flexion, wrist flexion & pronation
- Ulnar – Thumb adduction, ring & little finger flexion
- Radial – Wrist & finger extension, especially thumb
FURTHER READING
- Tsui B. Atlas of ultrasound and nerve stimulation-guided regional anaesthesia. 2007 Springer.
- www.usra.ca
- www.nysora.com
- Gray A, Schafhalter-Zoppoth I. Ultrasound guidance for ulnar nerve block in the forearm. Reg Anesth Pain Med 2003;28:335-9
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/