Regional Anaesthesia

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation. Please answer True or False:
- With regards to the anatomy of the spine and use of ultrasound:
a. Identification of the correct lumbar intervertebral space by physical examination has been found to be accurate only 29% of the time
b. Ultrasound has been shown to reliably predict depth to the epidural space 60% of the time
c. The conus medullaris has been shown to extend beyond L1/2 interspace on MRI in less than 5% of patients
d. Ultrasound has been demonstrated to decrease the number of passes required for a successful block
e. Tuffier’s line intersects the spine at the level of T4 - With regards to the technique of neuraxial ultrasound:
a. The best images of the spine are gained using a low frequency curvilinear probe due to their ability to visualize deep structures
b. Convention dictates that cephalad structures should appear on the right of the ultrasound image
c. Metalwork is a contraindication to neuraxial anaesthesia even with ultrasound
d. Only bone produces acoustic drop out with ultrasound
e. Ultrasound assisted neuraxial techniques are presumed to be associated with fewer side effects than non- ultrasound assisted neuraxial techniques - With regards to images seen during neuraxial scanning:
a. A saw-tooth pattern will be visible
b. A bunch of grapes will be visible
c. The anterior complex will be visible
d. Flying fish can be seen
e. An equal sign can be seen
Key Points
- Ultrasound can increases the correct identification of the intervertebral space
- Low frequency curvilinear post is best to use for neuraxial scanning
- Familiarity with the key ultrasound images is essential
- Scanning and inserting the needle under direct ultrasound guidance is possible but is technically very difficult
INTRODUCTION
Central neuraxial blockade is traditionally taught and performed using a landmark based technique, but is easily amenable to being aided by ultrasound. In this tutorial we will discuss:
- Why would you use ultrasound for neuraxial procedures?
- What can be seen on ultrasound for neuraxail procedures?
- How to perform neuraxial procedures using ultrasound?
- Specific patient groups where ultrasound can help
WHY WOULD YOU USE ULTRASOUND FOR NEURAXIAL PROCEDURES
Ultrasound is a portable and safe technology that is increasingly used to assist in performing anaesthesic procedures. The use of ultrasound has been integrated into the routine practice of a range of invasive procedures (e.g. vascular access and regional/ nerve blocks) with the main proposed benefits being: increased success rate and reduced complication rate. As we become more comfortable and knowledgeable with ultrasound, we are able to transfer its application and benefits to other procedures that were also previously landmark based.
Central neuraxial blockade is traditionally taught and performed using a landmark based technique. Current practice uses Tuffier’s line (an imaginary line drawn between the iliac crests that theoretically intersects the body of L4) and palpation of spinous processes in order to perform the procedure. However, Tuffier’s line is not a reliable marker of the appropriate spinal level in many people. One study showed that even experienced anaesthetists accurately identified the correct interspace only 29% of the time, with 51% of cases being more cephalad than they had thought1. With ultrasound assistance, the margin of error for correct identification has been estimated to never be more than one level, whereas it has been as many as four levels using palpation alone2. Ultrasound guided determination of the interspinous level has been shown to correlate with MRI 76% of the time3. Additionally, previous studies have shown that a significant proportion of the population has a conus medularis that extends below the body of L1: 19% when examined using MRI, and between 28 and 58% when studied by anatomical dissection1. So, if the conus extends lower than one might expect along with an intervertebral level identified by palpation being higher than expected, spinal anaesthetic placed at a site identified by palpation alone could be expected to have a higher potential of causing conus damage4.
The majority of patients receiving a spinal or epidural anaesthetic technique have easily identifiable landmarks and therefore carry a low risk of injury from the procedure. However, some patients have landmarks that are difficult to palpate, or abnormal anatomy such as scoliosis, potentially making a neuraxial block more challenging. Blocks that are more difficult to perform are associated with an increased risk of complications5, 6. Use of ultrasound can reduce the level of difficulty by giving the user a clear point for needle insertion and guidance to the angle, direction and depth of insertion. Ultrasound pre-scanning has been shown to almost halve the number of needle passes to achieve a successful block5 and also to reduce the number of epidurals that require re-siting7. A recent meta-analysis has concluded that overall, the evidence strongly suggests that pre-procedure neuraxial ultrasound prevents the occurrence of several well recognised mechanisms of injury, though to prove an actual reduction in already low complication rates would require a very large study6.
WHAT CAN BE SEEN ON ULTRASOUND FOR NEURAXIAL PROCEDURES
Ultrasound can help in understanding a patient’s underlying anatomy, especially in those with anatomical abnormalities that would not otherwise be appreciated by surface landmarks. [For principles of ultrasound, please see ATOTW 199 and 218.]8
The important structures that can be identified on ultrasound are:
- Bone: which will appear bright white with nothing visible deep to it (‘drop-out’) as ultrasound is unable to penetrate this.
- Ligaments: will also appear bright white but the drop-out will not be complete; structures deep to it will be visible in the gloom.
- Dura: the dura itself may produce a signal in some patients but is not a reliable finding. The spinal cord and CSF do not reflect ultrasound well and will be notable by its absence on the image.
- Soft tissue and muscle: these structures will also be identifiable dorsal to the spine.
HOW TO PERFORM NEURAXIAL PROCEDURES USING ULTRASOUND Pre-scan
It is worth initially scanning patients whom you expect to have normal anatomy to become comfortable with US assessment of the spine.
- This allows the correct interspace level and the midline of the patient to be determined, allowing a more accurate initial puncture point to be marked.
- An approximation of epidural or intrathecal depth can be made, allowing decisions about needle type and length to be made prior to starting the procedure.
- Guidance is given to the angle at which to insert the needle, both in the cephalad-caudad plane and the horizontal plane in order to reach the target with fewer needle passes.
The structures of interest usually lie deep, particularly in the obese patient, and a low-frequency curvilinear transducer gives the best images. An additional benefit is that the angle of view with the curvilinear probe is wide helping to identify structures from several adjacent vertebrae. Holding the probe low down at its base whilst bracing your hand holding the probe against the patient’s back allows small movements and changes in the angle of the probe to be made more easily thus reducing arm fatigue.
The first scan aims to identify the interspace at which you are planning to perform your block. Hold the transducer longitudinally so that its long axis is in a vertical plane, parallel to the spine – the parasagittal view (Figure 1). Start a few centimetres lateral to midline of the spine at a level cephalad to the iliac crests. By convention, the probe should be orientated so that the cephalad aspect is on the left hand side of the image. As the transducer is then moved medially, bony shadows with their drop-out will appear representing the tips of the transverse processes of the vertebrae (blue arrows). You may see the ‘trident sign’; three shadows cast by three adjacent transverse processes.
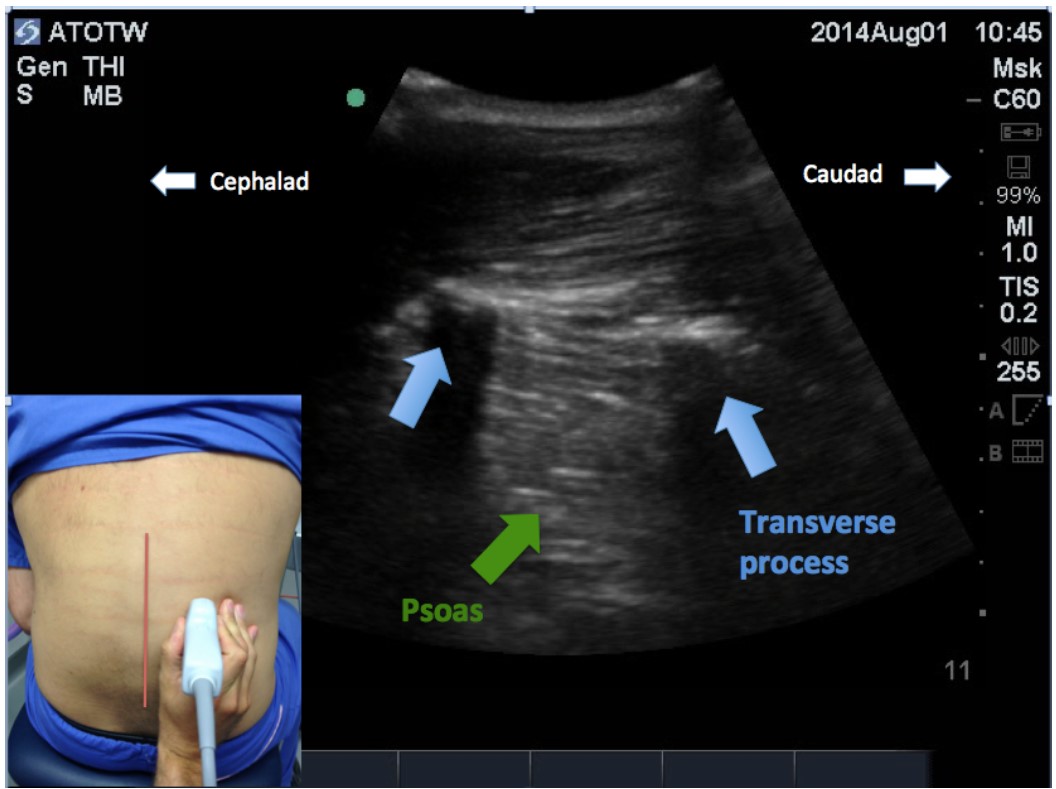
Figure 1: Parasagittal view approximately four centimeters off the midline, cephalad to the iliac crests. The tips of the transverse processes are visible as a bright crescent with an acoustic dropout extending deeper. The psoas muscle is seen between and deeper to the transverse processes. (Midline of spine indicated by red vertical line)
As the transducer is moved further medially, a ‘saw tooth’ pattern will become visible (Figure 2). This occurs when the beam is aligned with the articular processes of the vertebrae, which in this thin slice, would appear on ultrasound to be a continuous bony structure.
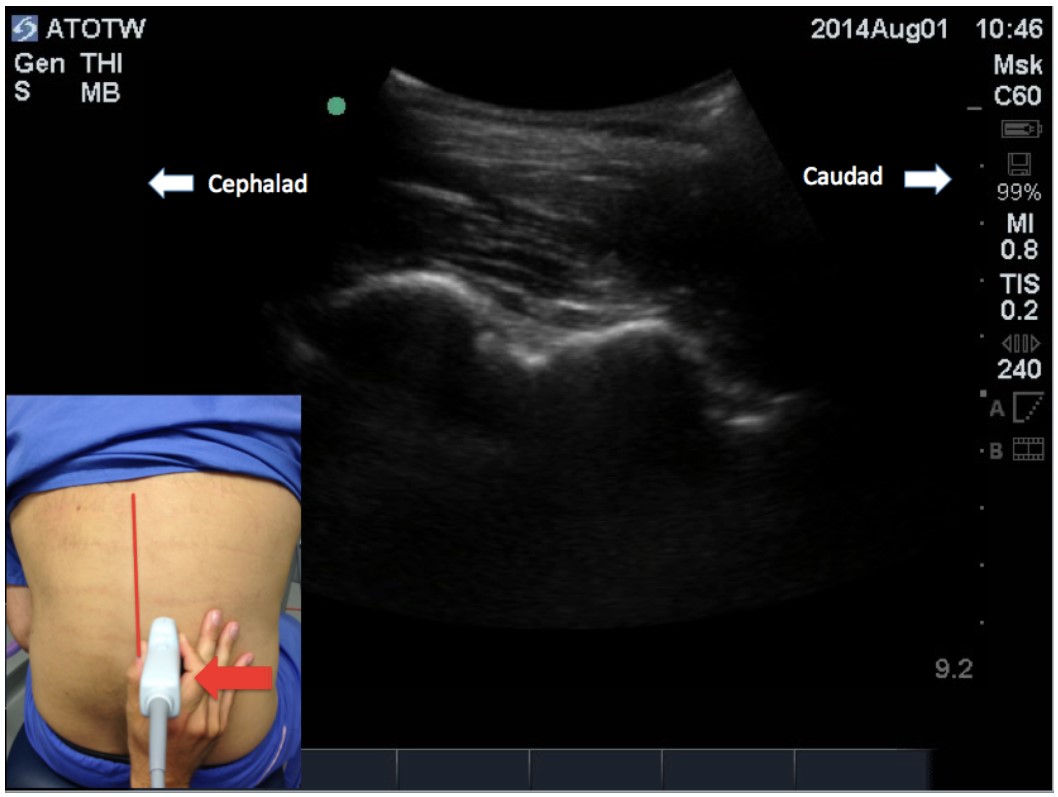
Figure 2: Parasagittal view more medial to previous view in figure 1. A continuous bony structure with complete acoustic dropout beneath is seen at a more shallow depth to the transverse processes of the previous view. (Midline of spine indicated by red vertical line)
At this point, if the probe is angled inwards towards the midline, the beam will move off the articular processes and fall on the vertebral laminae, giving an interrupted line of slanting bony shadows. This is the paramedian sagittal oblique view (Figure 3).
Deeper between the shadows thrown by the laminae (green arrows), another horizontal hyperechoic line should be visible. This is the reflection of the ultrasound off the posterior vertebral body after it has passed through the gap between the laminae and through the ligamentum flavum, the dura and spinal cord. The reflection is known as the anterior complex. It must be remembered, however, that the anterior complex is not the intended target for the needle during the anaesthetic that follows; visualising it demonstrates that the ultrasound beam can pass through the posterior dura that is targeted, and continue further to reflect off the deeper boney structure that shows up better on ultrasound.
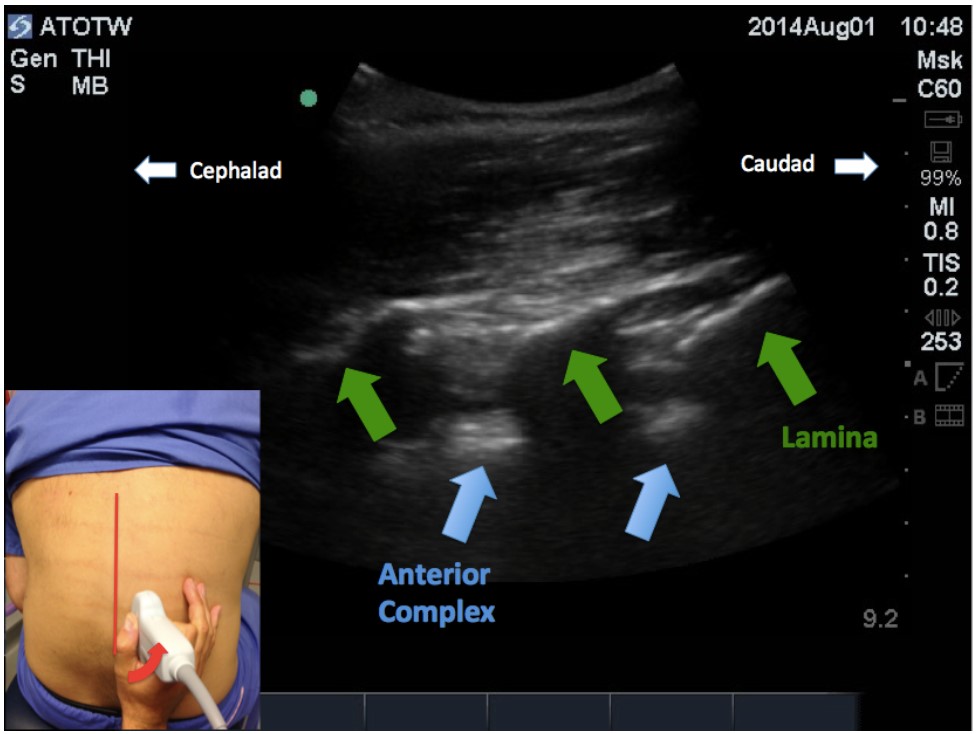
Figure 3: Paramedian sagittal oblique view. Angulation of the probe towards the midline shows the spaces between adjacent laminae. This view shows the angle at which a paramedian approach for a spinal or epidural anaesthetic would be placed.
To identify the correct intervertebral space level from here, the sacrum must be identified. Keeping the probe at the same angle, slide it in a caudad direction, the interrupted line is eventually replaced in the caudad aspect by a single long uninterrupted hyperechoic structure (Figure 4). This is the sacrum, and the gap between the more cephalad lamina and the sacrum is the L5-S1 interspace. Now sliding the transducer cephalad (again at the same angle), each lamina and interspace level can be counted off, and the interspace required for needle insertion can be identified and marked. Additionally, the parasagittal line that the probe has been moved along could also be marked, as this is the starting point for a paramedian approach to the neuraxis.
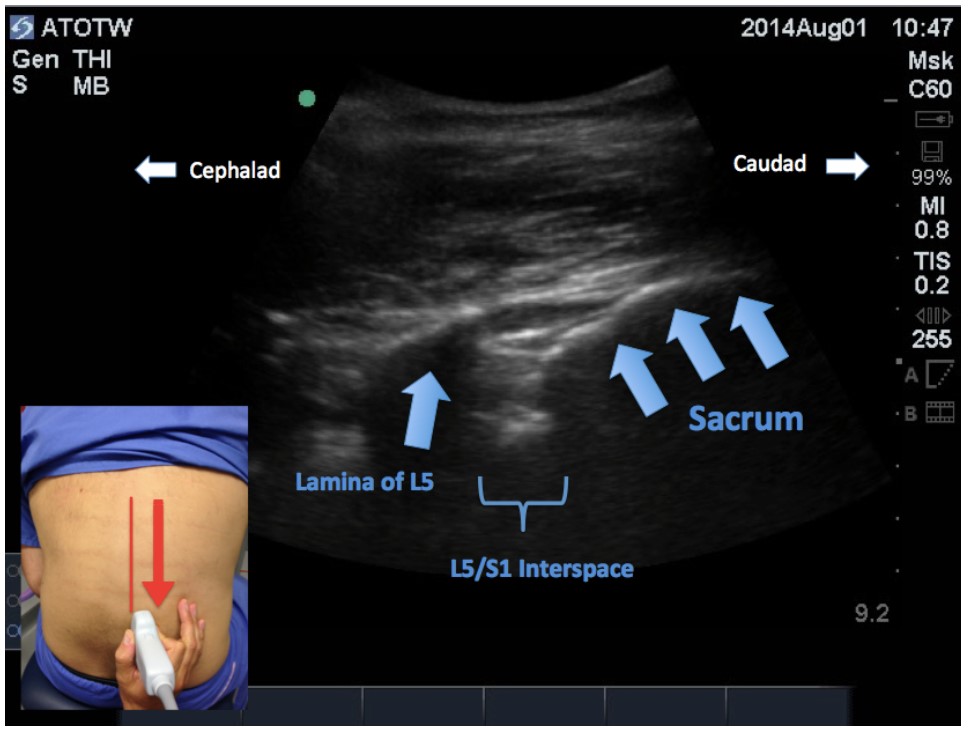
Figure 4: Paramedian sagittal oblique view of the sacrum and L5 lamina.
The transducer is then turned 90 degrees, keeping the midpoint of the transducer at the intervertebral level selected; this is the transverse view, and is the view that is best for identifying the midline and the depth to space. It gives what is effectively a cross sectional view of the spine. Sliding the probe slightly up or down, between the spinous processes and angling the probe slightly cephalad or caudad will reveal the classic ‘flying bat’ ultrasound view (figures 5 and 6).
The interspinous ligament should be identified as a hyperechoic structure in the midline with an incomplete drop out. Deeper within the incomplete drop out, the hyperechoic horizontal line of the anterior complex should be visible. At this position, with the probe at this angle, an ultrasound beam can traverse the ligaments and other structures of the spine to reflect back to the probe, and therefore a needle following the same path should be able to reach the epidural space or dural sac along that same route. In this view, the depth that the needle should be placed can also be estimated. If an imaginary line is drawn between the bases of the articular processes or between the transverse processes, this would approximate the position of the ligamentum flavum and the depth to the space can be measured using the calipers on the ultrasound machine. On occasion, the ligamentum flavum and dorsal dura are seen as a hyperechoic line which, along with the hyperechoic line of the anterior complex, produces the “=” sign. The distance between lines of the “=” sign approximates the diameter of the spinal canal.
If the transducer was placed directly over a spinous process (Figure 7), the laminae and spinous process would cause acoustic dropout with very little useful information being available, other than the position of the midline.
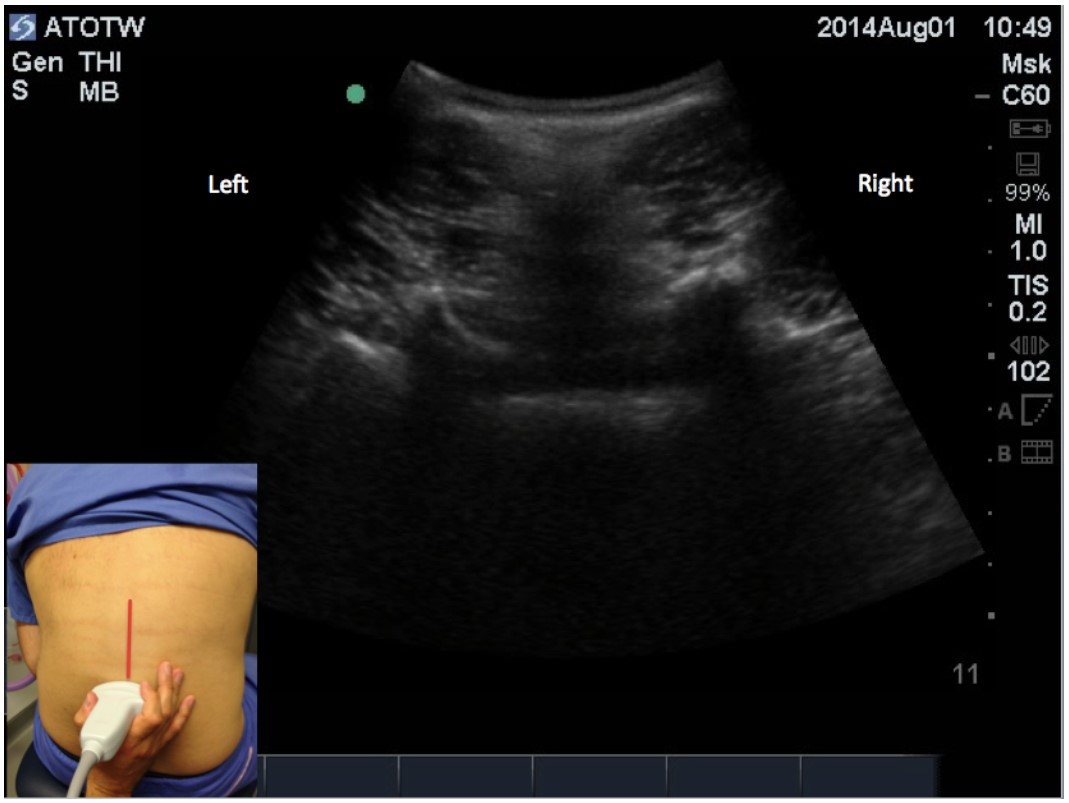
Figure 5: Transverse view between spinous processes.
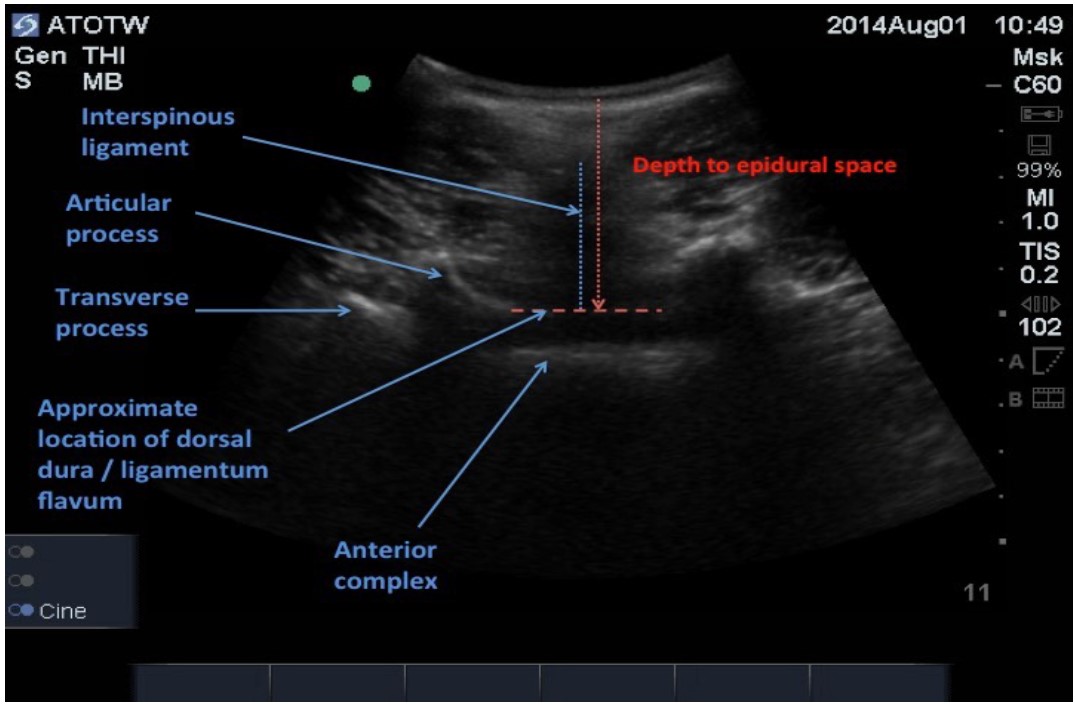
Figure 6: Transverse view between spinous processes demonstrating visable structures and measurements. The depth to the epidural space (as read off the scale on the right hand side of the ultrasound screen) is approximately 5 cm.
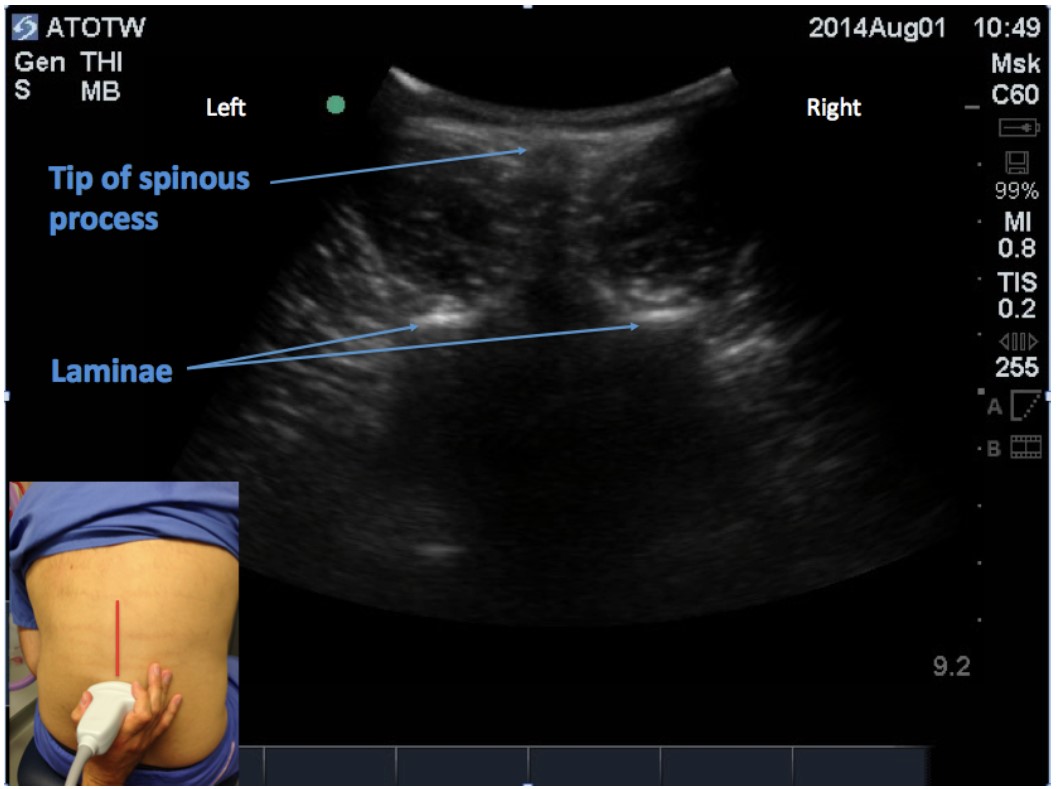
Figure 7: Transverse view with the transducer directly over a spinous process.
Upon completion of the pre-procedure scan, the exact intervertebral level is now known and marked, then the midline and approximate depth to space are marked and measured, and the entry point for the needle and the best angle at which to insert it have been mentally noted.
The University of Toronto has produced a three-dimensional interactive tool to help with learning the images to look for during the pre-procedure scan available at http://pie.med.utoronto.ca/VSpine/VSpine_content/VSpine_ultraSoundGuided_lumbar.html.
A simplified technique
Because the technique of performing neuraxial ultrasound as described above has a significant learning curve, a simplified technique – the paraspinous approach – has recently been described9. This is somewhat easier to perform, particularly in difficult or obese patients where the only landmark visible on ultrasound is the midline. After identifying the midline on the transverse view, the spinous processes are marked and the needle is placed one centimeter laterally and superiorly to a spinous process. The approach is then similar to a shallow angled paramedian approach to the neuraxis, redirection of the needle being guided by the depth at which bone is contacted.
Real-time ultrasound guided neuraxial anaesthesia
Real time ultrasound guided techniques are technically more difficult and should be reserved for the more experienced ultrasound user. It gives the added benefit of ensuring the needle is on the correct trajectory in real time but becomes technically difficult as these techniques, particularly epidural procedures, are usually two handed techniques. Having a second person to hold the probe and perform the scan adds complexity and means that the needle operator loses some of their orientation. For loss-of-resistance techniques, pre-sprung syringes could be a potential solution.
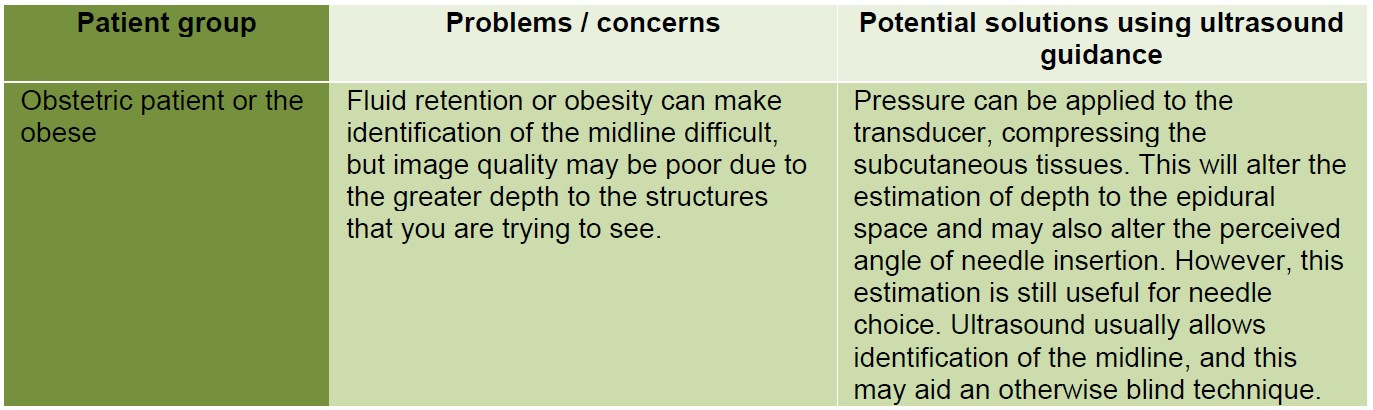
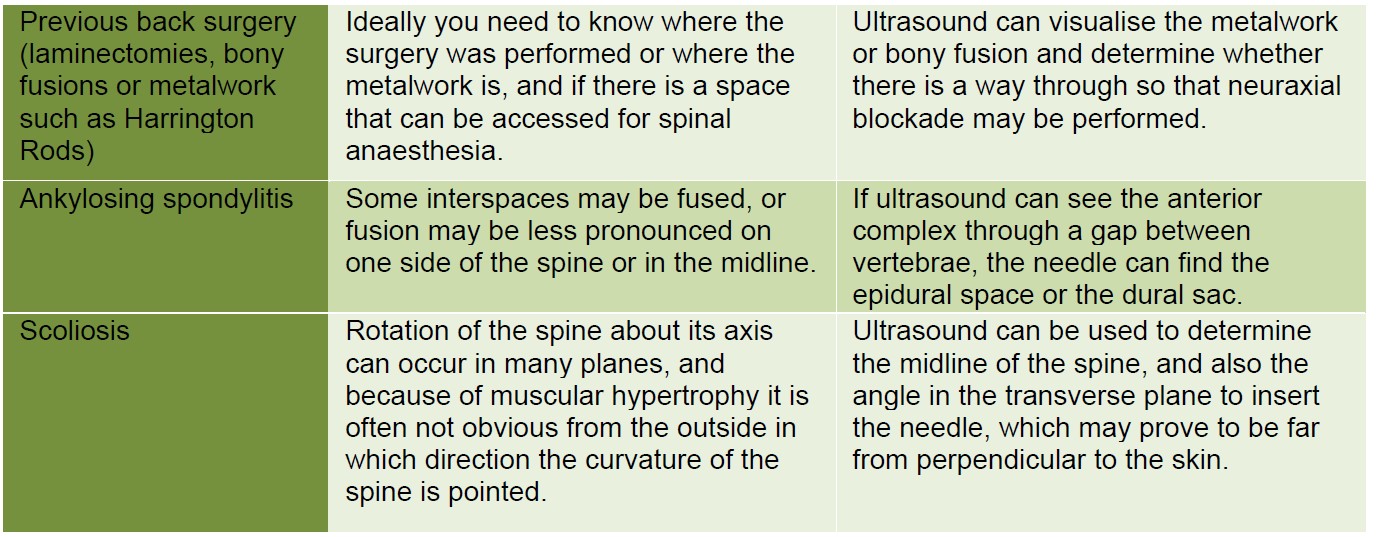
SPECIFIC PATIENT GROUPS WHERE ULTRASOUND CAN HELP
SUMMARY
- Landmark and palpation-based marking of intervertebral levels are often inaccurate. They frequently result in a spinal anaesthetic block being sited at a higher intervertebral level than is appreciated.
- Ultrasound machines are now more widely available and are used for a variety of anaesthetic procedures.
- Pre-procedure ultrasound scanning of the back can help identify the ideal site, angle of needle insertion and the approximate depth to the epidural space.
- Use of ultrasound can result in fewer needle passes, increased patient comfort, and is likely to improve patient safety.
- Real time ultrasound placement of spinal or epidural techniques has been described but is
ANSWERS TO QUESTIONS
- With regards to the anatomy of the spine and use of ultrasound:
a. True
b. False The actual figure is higher at 76%3.
c. False The real figure is higher at 19%1
d. True
e. False Tuffier’s Line is said to cross the spine at the level of the body of L4. Ultrasound scanning shows that this is frequently not actually the case. - With regards to the technique of neuraxial ultrasound:
a. True Deeper structures are seen better with a low frequency probe. Additionally, a curvilinear probe looks at a wider field , so that several vertebrae can be seen in one view.
b. False By convention, the probe is orientated in the sagittal views so that cephalad structures are on the left.
c. False The presence of metalwork is not a contraindication to neuraxial procedures, but it may well interfere with the images obtained on ultrasound.
d. False Ligaments will produce incomplete dropout, metalwork will also produce complete drop-out.
e. True Although there is not any evidence of reduced complications (due to the difficulty of designing such a study), there is evidence of improved patient comfort and reduced re-siting of labour epidurals5.
3. With regards to images seen during neuraxial scanning:
a. True A saw-tooth pattern will be visible with medial parasaggital view (Figure 2).
b. False A bunch of grapes is seen during a supraclavicular block
c. True The reflection of the ultrasound off the posterior vertebral body after it has passed through the gap between the laminae and through the ligamentum flavum, the dura and spinal cord is known as the anterior complex.
d. False The classic ‘flying bat’ ultrasound view can be seen (Figures 5 and 6)
e. True On occasion, the ligamentum flavum and dorsal dura are seen as a hyperechoic line which, along with the hyperechoic line of the anterior complex, produces the “=” sign.
REFERENCES AND FURTHER READING
- Broadbent CR, Maxwell WB, Ferrie R et al. Ability of anaesthetists to identify a marked lumbar interspace. Anaesthesia 2000;55:1122-6.
- Furness G, Reilly MP, Kuchi S. An evaluation of ultrasound imaging for identification of lumbar intervertebral level. Anaesthesia 2002; 57: 277-80.
- Watson MJ, Evans S, Thorp JM. Could ultrasonography be used by an anaesthetist to identify a specified lumbar interspace before spinal anaesthesia? Br J Anaesth 2003;90 (4): 509-511.
- Reynolds F. Damage to the conus medullaris following spinal anaesthesia. Anaesthesia 2001; 56: 238-47.
- Grau T, Leipold RW, Conradi R, et al. Efficacy of ultrasound imaging in obstetric epidural anesthesia. J Clin Anaes 2002; 14; 169–175.
- Perlas A, Chaparro LE, Chin KJ. Lumbar neuraxial ultrasound for spinal and epidural anaesthesia: a systematic review and meta-analysis. Reg Anesth Pain Med 2014 Dec.
- Grau T, Leipold RW, Conradi R et al. Ultrasound control for presumed difficult epidural puncture; Acta Anaesthesiol Scand 2001; 766–771.
- MacGregor M, Kelliher L, Dr J Kirk-Bayley. The physics of ultrasound parts 1 and 2. ATOTW 199, October 2010; ATOTW 218, March 2011.
- Chin KJ, Perlas A, Chan V. The ultrasound-assisted paraspinous approach to lumbar neuraxial blockade: a simplified technique in patients with difficult anatomy. Acta Anaesthesiol Scand 2015; 59: 668-73.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/