Regional Anaesthesia

KEY POINTS
- Popliteal block is a distal block of the sciatic nerve, which in combination with a saphenous nerve block will provide regional anaesthesia and/or analgesia for foot and ankle surgery.
- Division of the sciatic nerve into its branches, the common peroneal nerve and the tibial nerve, typically takes place around 6.5 cm above the popliteal crease.
- A catheter can be inserted to prolong the duration of analgesia.
INTRODUCTION
The majority of the sensory and motor innervation of the foot and lower leg is provided by the sciatic nerve. There is a smaller sensory-only component provided by the saphenous nerve, which itself is derived from the femoral nerve. Blockade of the sciatic nerve in the popliteal fossa is a common technique to provide regional anaesthesia and analgesia for foot and ankle surgery. This block has the advantage over more proximal approaches to the sciatic nerve in that it preserves hamstring motor function. It may still result in a foot drop, occasionally causing mobility issues, which can result in delayed discharge particularly in elderly patients. The popliteal block, as a more distal approach to blockade of the sciatic nerve, also reduces the chance of nerve damage.
In order to provide complete analgesia or anaesthesia below the knee, popliteal sciatic blockade should be used together with a femoral or saphenous nerve block. If a tourniquet is required for awake surgery the tourniquet should be applied on the calf as a popliteal sciatic block will not provide a more proximal block. The use of ultrasound allows direct real-time visualization of the nerve(s) and deposition of local anaesthetic (LA) and so can improve the chance of successful nerve blockade.1
ANATOMY
The Sciatic Nerve
The sciatic nerve (SN) is derived from the ventral rami of the lumbo-sacral plexus L4-S3. It exits the pelvis as the most lateral structure via the greater sciatic foramen below piriformis, and travels between the greater trochanter and ischial tuberosity to descend in the posterior aspect of the thigh towards the popliteal fossa2 (Figures 1 and 2).
It is the largest and broadest nerve in the body and at its greatest extent it can be over 2 cmwide and 0.5 cm thick.3–5 The tibial nerve (TN) is formed of fibres from the anterior divisions of anterior rami of the sciatic nerve whilst the common peroneal nerve (CPN) is formed from the posterior divisions of the anterior rami of the sciatic nerve. Both are encased within a common fascial sheath until they divide into their respective components.2 Of particular note, the TN and CPN do not exchange fibres within the sheath.4
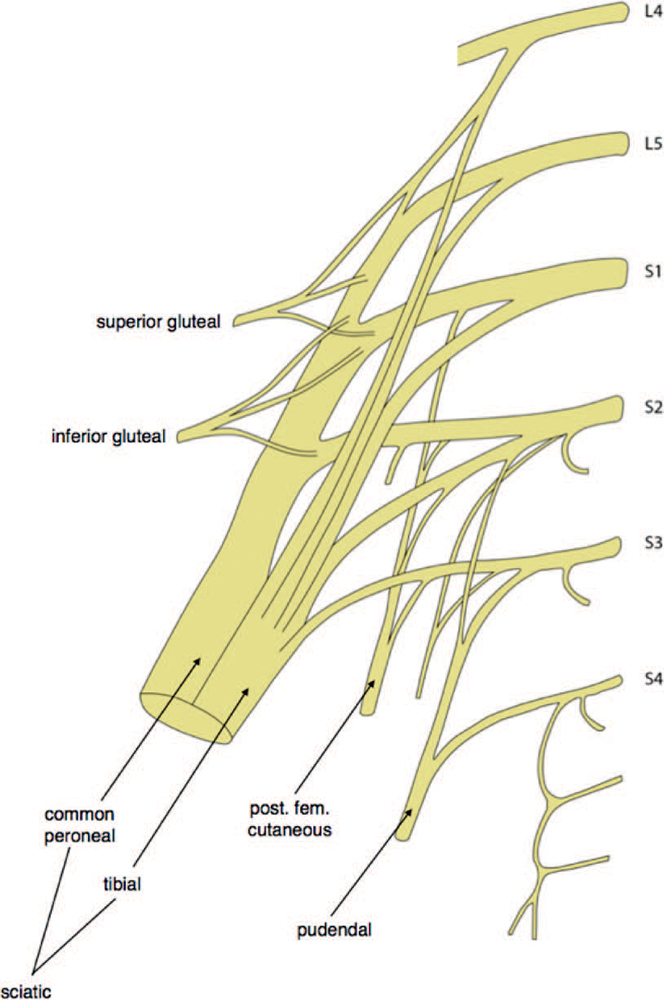
Figure 1. Simplified anatomy of the lumbo-sacral plexus. Note the sciatic nerve arising from L4, L5, S1, S2, and S3 nerve roots. Source: Courtesy of Joanna Levy.
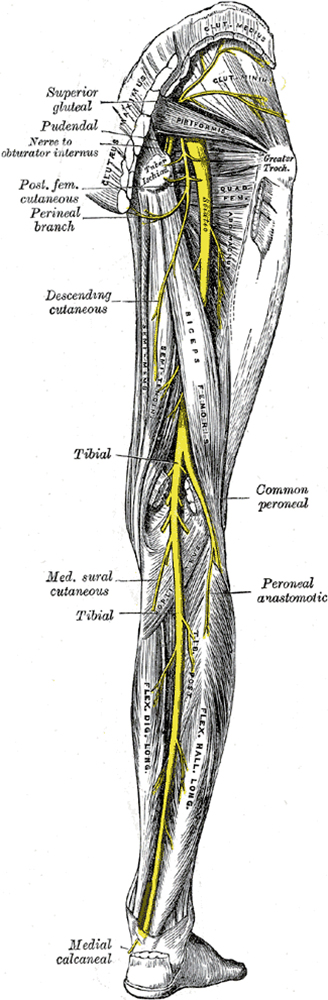
Figure 2. The course of the sciatic nerve. Source: Gray’s Anatomy of the Human Body 20th ed. (Public domain.) http://www.bartleby.com/107/ illus832.html.
Anatomical Variations
Division typically takes place around 6.5 cm from the popliteal fossa crease, although there is significant anatomical variationanywhere from roughly 5 cm to 18 cm above the popliteal crease.2,4 In a small group of patients high division of the SN may takeplace in the pelvis, and occasionally trifurcation may occur with an additional muscular branch to the soleus.3 Ultrasound will aid inidentification of unusual anatomy that might otherwise be missed with a landmark or nerve-stimulator technique (Figure 3).
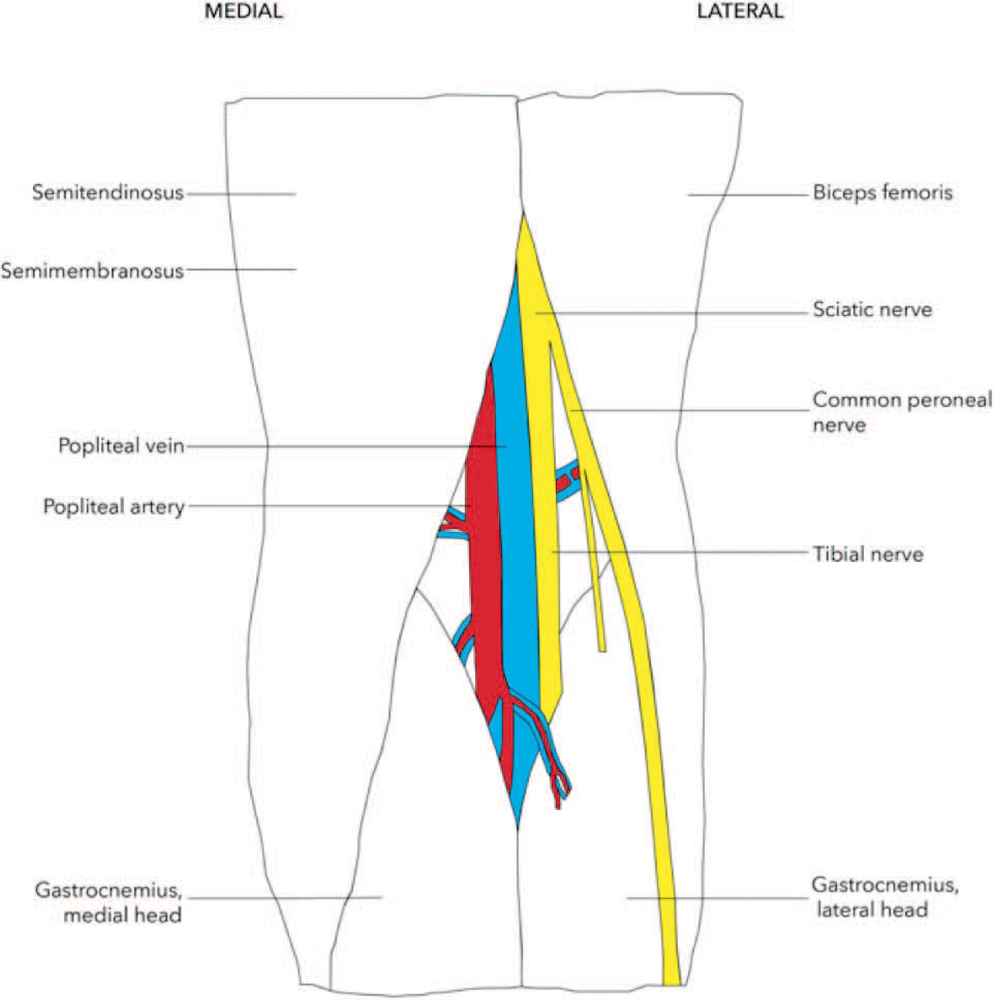
Figure 3. Simplified anatomy of the right popliteal fossa. Source: Courtesy of Joanna Levy.
The Course of the Tibial and Peroneal Nerves
The popliteal fossa is formed in the posterior knee of the biceps femoris muscle superolaterally, the semitendinosus superomedially, and the lateral and medial heads of the gastrocneumius inferiorly.5 On entering the popliteal fossa both nerves are located superficial and lateral to the popliteal artery and vein. The TN, which is usually the largest branch, lies more medially, closely related to the vessels, whilst the CPN lies laterally and more superficially (Figure 4).
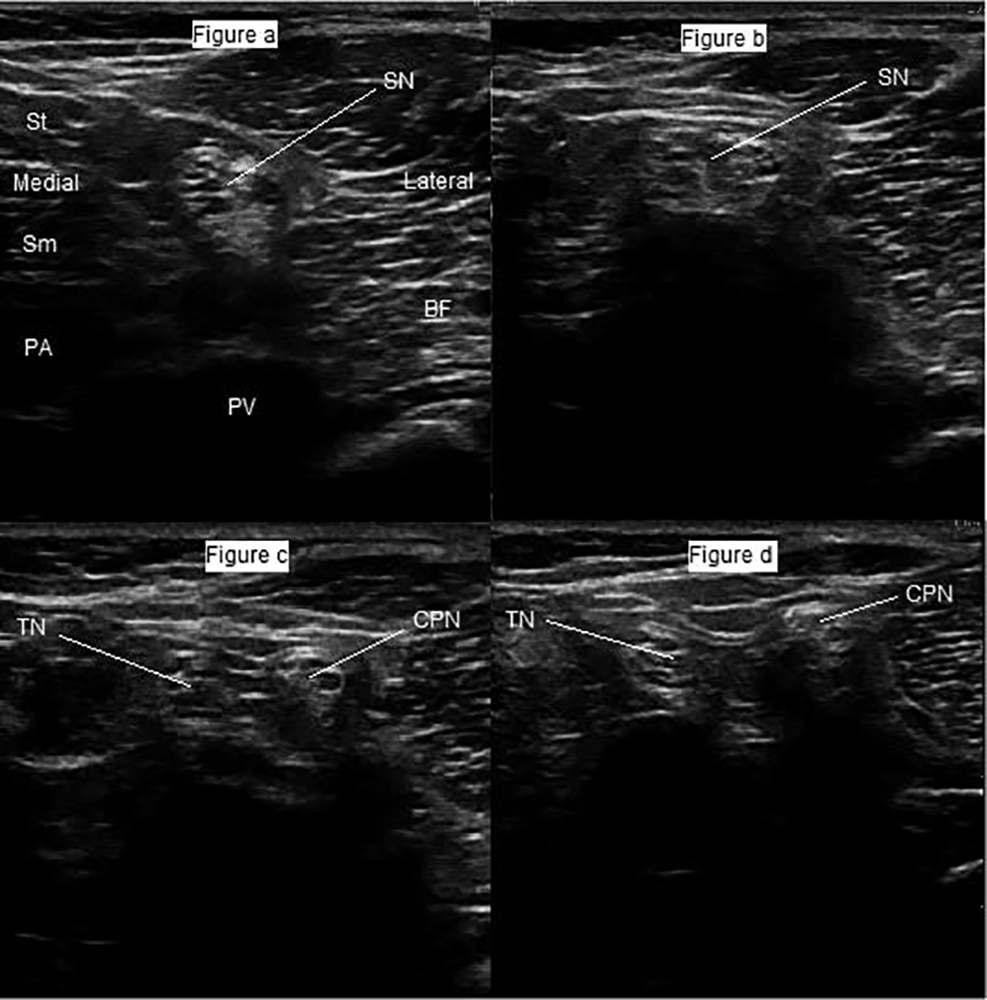
Figure 4. The course of the sciatic nerve from proximal to distal (sequential scans from a to d) as it divides into the tibial nerve and common peroneal nerve. SN indicates sciatic nerve; PA, popliteal artery; PV, popliteal vein; Sm, semimembranosus muscle; St, semitendinosus muscle; BF, biceps femoris muscle; TN, tibial nerve; and CPN, common peroneal nerve. Source: Dr David Levy’s and Dr Andrew McEwen’s archive.
The tibial nerve
Within the leg the TN gives off the medial sural cutaneous nerve before descending posteromedially to supply the posterior muscles of the leg and the skin on the heel of the foot via the lateral and medial plantar nerves. The sural nerve is formed from the medial sural cutaneous nerve and a peroneal anastomotic branch. It supplies skin on the posterior and lateral aspects of the leg and lateral side of the foot.5,6
The common peroneal nerve
The CPN descends laterally in the popliteal fossa, supplying skin on the superolateral part of the posterior leg, before winding around the neck of the fibula to give off superficial (SPN) and deep (DPN) branches. The peroneal nerves supply the muscles of the anterior leg. The SPN supplies skin on the distal third of the anterior surface of the leg and dorsum of the foot whilst the DPN supplies the skin of the first web space.5,6
The saphenous nerve (branch of the femoral nerve)
Of note, the skin on the medial aspect of the leg and foot is supplied by the saphenous nerve, a branch of the femoral nerve which courses along the tibial side of the leg in close association with the great saphenous vein.5,6 The saphenous nerve only provides sensory innervation to the lower leg.
Figure 5 demonstrates the cutaneous innervation of the lower limb.
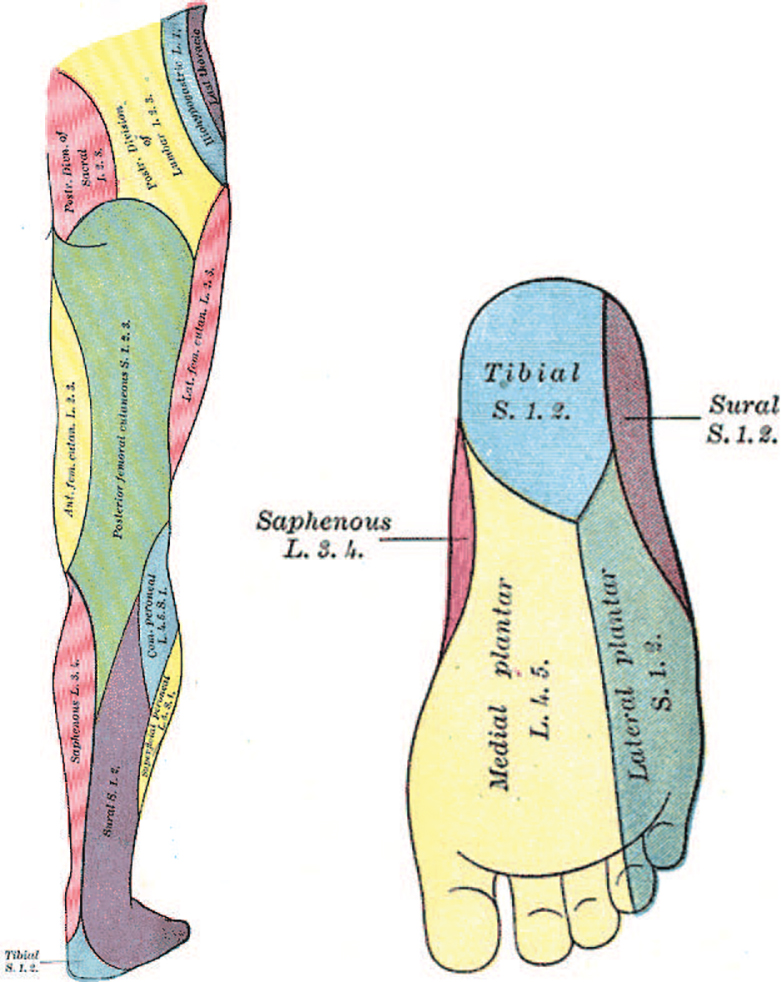
Figure 5. Distribution of cutaneous nerves of the lower limb and foot. Source: Gray’s Anatomy of the Human Body 20th ed. (Public domain.) http://www.bartleby.com/107/illus831.html and http://www.bartleby.com/107/illus834.html.
INDICATIONS
This is not intended to be an exhaustive list, but the following operations may benefit from a popliteal block. A femoral or saphenous nerve block may also be necessary if surgery involves the medial aspect of the leg or foot. Please see ATOTW Tutorial No. 301: Ultrasound-guided adductor canal block (saphenous nerve block) and ATOTW Tutorial No. 284: Ultrasoundguided femoral nerve block.
- Foot and ankle surgery
- Vascular surgery
- Lower limb angioplasty
- Analgesia for posterior knee surgery (posterior knee pain)
CONTRAINDICATIONS
Absolute
- Patient refusal
- Inflammation or infection over injection site
- Allergy to LA
Relative
- Anticoagulation or bleeding disorders
- Preexisting peripheral neuropathies
- Where sensory block may mask compartment syndrome
COMPLICATIONS
These are the same as for any regional anaesthetic technique:
- Block failure
- Haemorrhage/bruising/haematoma
- Infection
- Nerve damage
- LA toxicity
- Allergy to LA
LA Choice
The choice, concentration, and volume of LA should be tailored to the specific goals of surgical anaesthesia, postoperative analgesia, speed of onset, duration of block, and motor-sparing effects.
Levobupivacaine (0.25%-0.5%) and bupivacaine (0.25%-0.5%) provide slower onset and long-duration blocks—they are commonly used in the United Kingdom. An alternative, ropivacaine (0.2%-0.75%), provides a moderately fast onset with long duration of action. For more rapid onset but shorter duration blocks, lignocaine (1%-2%) or prilocaine (1%) can be employed.
There is no significant difference in onset or duration of action for bupivacaine when compared to levobupivacaine. Mean onset time has been found to be between 15 and 35 minutes with a duration of sensory block of 13 ± 1 hours with first pain medication generally required at between 14 and 15 hours postblock.7–9 Ropivacaine 0.75% in one study was shown to act in as quickly as 13 minutes with a duration of analgesia of up to 16 hours.8
NERVE-STIMULATOR TECHNIQUE VERSUS ULTRASOUND-GUIDED TECHNIQUE
Ultrasound-guided popliteal block has been shown to have a higher success rate, require less time to perform, and be associated with less peri-procedural pain when compared to a nerve-stimulator technique.1,10 Ultrasound technology used for insertion of catheters has been shown to be associated with a higher success rate and fewer vascular punctures and is more cost effective as it reduces time for catheter placement and reduces subsequent nurse-patient contact.11,12 For these reasons ultrasound should be considered the ‘‘gold standard’’ when performing a popliteal block.
PREBLOCK PREPARATION
Before starting ensure there are appropriate indications for a popliteal block and no contraindications. Consent the patient and advise them on the likely duration of block.
Ensure that the site/side is clearly marked, the patient is monitored, intravenous access obtained, and appropriate, assistance, equipment, and resuscitation drugs are available. For complete details on preparation for peripheral nerve blocks please see ATOTW Tutorial no. 134: Peripheral nerve blocks—getting started.
Equipment
- Ultrasound machine with high-frequency probe
- 22 gauge 80- or 100-mm short-beveled insulated ultrasound needle
- Skin antiseptic
- Sterile gloves
- 1 to 5 mL of short-acting LA for skin
- LA for the block (usually 20 ml) A safe dose should be calculated based on the weight of the patient.
Patient Positioning
Where possible this block should be performed on an awake or lightly sedated patient. This aids the recognition of inadvertent intraneural injection, which may be detected by the patient reporting pain on injection. In addition, it can aid in early recognition of LA toxicity should the patient complain of perioral tingling or tinnitus, or become confused.
- Confirm operative site and side with patient and check the limb is marked and corresponds with information on consent form. In our institution we perform a ‘‘Stop Before You Block’’ check (https://www.rcoa.ac.uk/sites/default/files/CSQ-PS sbybsupporting.pdf).13
- Apply full standard monitoring and secure intravenous access.
- If required, proceed with central neuraxial blockade, sedation, or a general anaesthetic according to the anaesthetic plan.
- The block may be performed in a prone, lateral, or supine position. When supine the knee may be flexed or alternatively straight with a support under the lower leg and ankle to suspend it high enough to accommodate the ultrasound probe (Figures 6 and 7).
- It is our preference to perform the block in a lateral position with the operative side (side to be blocked) uppermost.
- With the patient lateral we then position the ultrasound machine in front of the patient, whilst standing behind the patient. This ensures a good position for the operator to view the screen and perform the block comfortably.
- Clean the site with antiseptic and allow to dry.
- A high-frequency ultrasound probe can be placed in a transverse orientation in the popliteal crease set to an initial depth of 4 to 6 cm (Figures 6 and 7).
Extra caution: Should the prone position be used, particular care should be exercised to ensure the correct side is blocked once the patient is turned to lie on their abdomen.

Figure 6. Lateral positioning for popliteal nerve block. Source: Dr David Levy’s and Dr Andrew McEwen’s archive.

Figure 7. Supine positioning for popliteal nerve block. Source: Dr David Levy’s and Dr Andrew McEwen’s archive.
PRACTICAL CONDUCT OF THE BLOCK
Scanning Technique
- The ultrasound probe should be held transversely to the thigh to gain a short-axis view of the nerves and vessels (Figures 6 and 7).
- Identify the popliteal artery and vein in the popliteal fossa. The TN should be seen superficial to the vein appearing as a bright echogenic structure. The CPN lies laterally (Figure 8).
- Both nerves are highly anisotropic (they appear bright when the probe is perpendicular to them, but become indistinct with a change in the angle of the probe) and so tilting the probe so that it is 908 to the nerves will improve visualisation significantly.
- Optimise image, adjusting depth, gain, and frequency settings.
- Scan proximally to identify where the CPN and TN converge to form the SN.
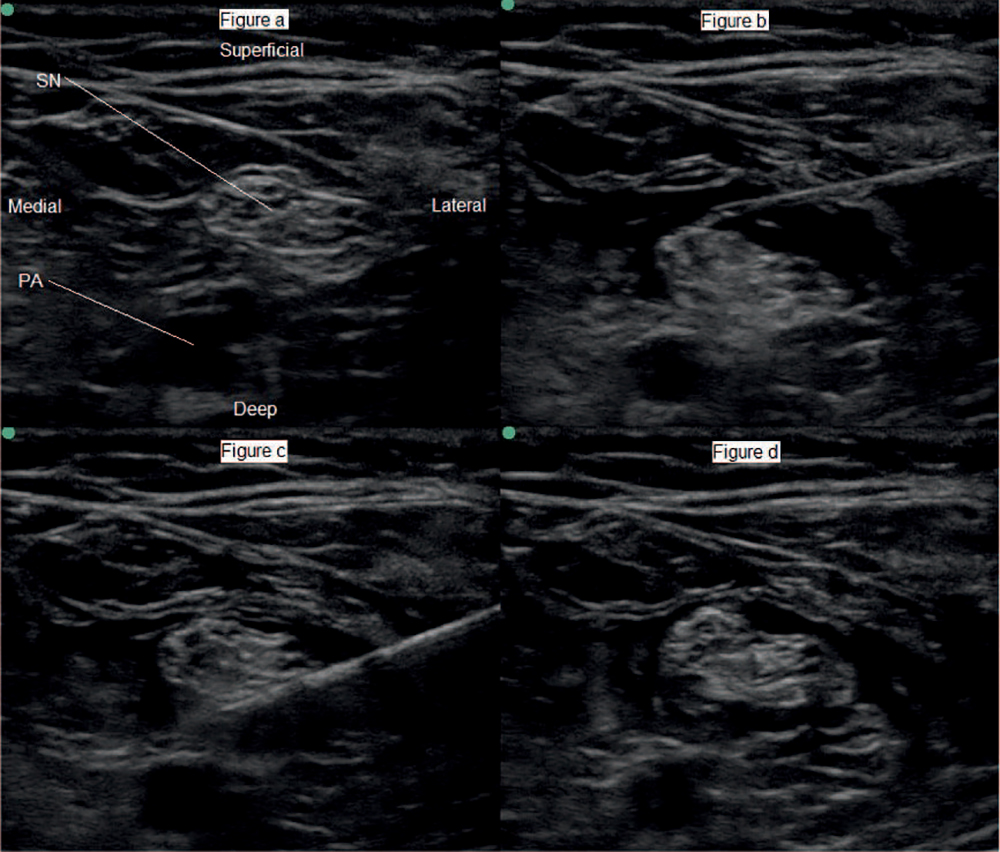
Figure 8. (a) Ultrasound image of the sciatic nerve. (b and c) Needle placement superficial and deep to the sciatic nerve with spread of local anaesthetic around the nerve. (d) Circumferential spread of local anaesthetic around the nerve (seen as a hypoechoic rim around the nerve). Note the sciatic nerve is just about to part into the two nerve components. SN indicates sciatic nerve; PA, popliteal artery. Source: Dr David Levy’s and Dr Andrew McEwen’s archive.
Needle Insertion
- It is convenient to block the SN with a single injection but the CPN and TN may also be blocked individually and block is best performed where the nerve(s) are easiest to identify.
- Should onset of anaesthesia or analgesia be important, the CPN and TN may be targeted individually as this is associated with a relative reduction in onset time of approximately 30%.14
- Inject a small amount of 1% lignocaine to anaesthetise the skin.
- The local anaesthetic needle may be used as a ‘‘finder’’ needle to verify that the angle of approach is correct.
- An in-plane approach should be used with the needle inserted from the lateral aspect of the thigh at a depth corresponding with where the nerve has been identified on ultrasound (Figure 8). The following are advantages of this approach:
- This allows the entire length of the needle to be seen, potentially reducing the chance of damage to adjacent structures.
- It will ensure the needle is as parallel to the ultrasound probe as possible and therefore improve its visualisation (steeper angles reflect ultrasound beams away from the transducer, decreasing the visibility of the needle).
- An alternative approach is out-of-plane. Most anaesthetists will be familiar with using a needle and ultrasound probe in this manner. However it may be difficult to ensure that the needle tip is always seen.
- Use 1 to 2 mL of LA to confirm correct injection site.
- Inject a total volume of 20 mL of LA around the SN; this can be divided if blocking individual nerves.
- Injection should take place slowly and be divided into 5-mL aliquots at a time. Each 5 mL injection should be followed by aspiration. Injection should stop immediately if there is aspiration of blood, or resistance/pain on injection.
- Circumferential spread of LA can improve the chances of successful sensory block.15
- An alternative method involves a single injection of LA underneath the common paraneural sheath, which may serve as a barrier to LA uptake.16–18
- A self-injection technique can be used, maximising the spread of LA through a number of small boluses and reducing the chance of communication error.19 Several techniques have been described, but in essence this method involves holding the needle and syringe in the same hand to allow the operator to depress the plunger of the syringe when required whilst simultaneously using the ultrasound probe with the other hand.
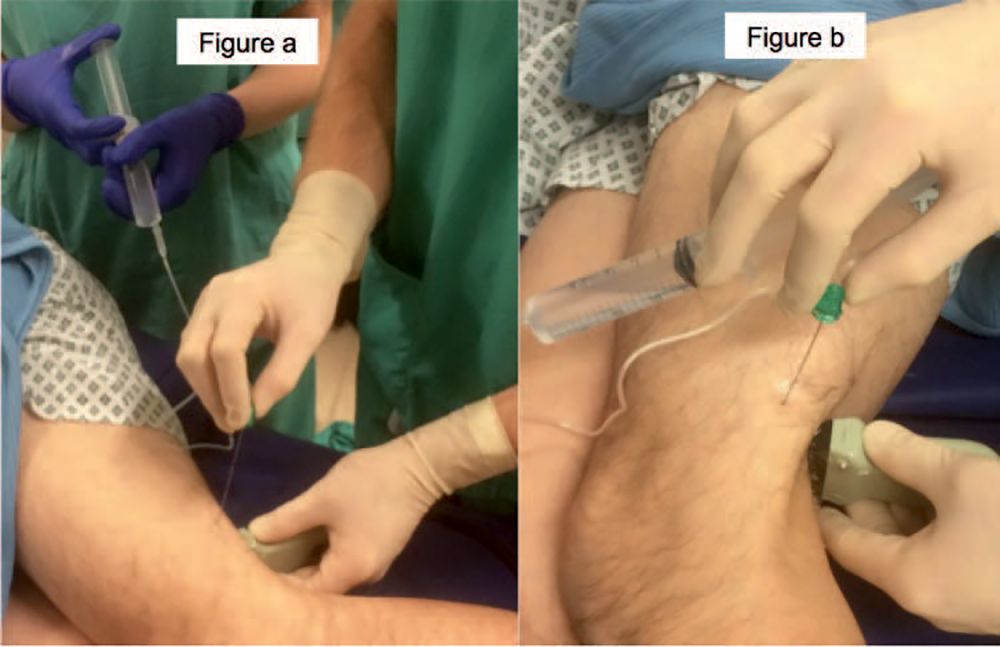
Figure 9. (a) Injection of local anaesthetic by assistant. (b) Self-injection of local anaesthetic. Source: Dr David Levy’s and Dr Andrew McEwen’s archive.
- Alternatively, the operator can control the ultrasound probe and needle whilst an assistant controls delivery of LA (Figure 9).
- Spread of LA should be visualised at all points. If spread of LA is not clearly seen consider the possibility of intravascular placement of needle, therefore requiring repositioning of the needle.
- Should longer-term analgesia be desirable, a catheter can be inserted adjacent to the SN after the initial dose has been administered. However, this is usually best done using an out-of-plane approach aiming cranially so that the catheterfollows the course of the nerve proximally. This technique is associated with few early or late complications and a good success rate.20
- At the authors’ institution, we typically use 0.125% levobupivacaine infused at a rate of 0 to 10 mL per hour when using popliteal catheters. Alternatively, bolus injections every 6 hours can be used. The disadvantage of this approach is an increase in workload. A protocol should be put in place with all staff trained in management of peripheral nerve catheters and also, importantly, the recognition and initial management of LA toxicity.
Subparaneural Injection Versus Circumferential Spread
The endpoint for blockade of the SN in the popliteal fossa is traditionally described as circumferential spread of LA around the nerve. As mentioned above, the SN is made up of the TN and CPN within a common paraneural fascial sheath (this is separate from the epineurium of the nerve). A more recent technique, made possible by high-quality ultrasound imaging, involves identification of the hyperechoic paraneural sheath. Although present for the entire length of the SN, it is most recognisable at the point at which the SN bifurcates and thus this region can be targeted as the point of insertion of the needle tip (space between the paraneural sheath and epineurium). LA should be seen to spread around the two nerves.16,17 Importantly, there should be no change in nerve diameter, as this signifies intraneural injection, which may cause long-term neurological damage. If this occurs or if high pressure is encountered during injection of LA, then the operator should stop immediately and reposition the needle tip location. The subparaneural technique is associated with a predictable block that is faster in onset and longer in duration than when the CPN and TN are blocked with conventional circumferential spread and has the advantage of not requiring multiple readjustments of the needle.17,18
However, an important point to highlight is that subparaneural injection in popliteal nerve block has limited data on its safety profile. Needle placement needs to be nearer to the nerve than in the conventional approach, increasing the potential risk of intraneural injection, and it is possible that the pressure effect of the LA may lead to neuronal ischaemia. One study, with some limitations, did suggest a possible subclinical neurological injury and this should be kept in mind when deciding upon which technique to employ.21
POSTPROCEDURE CARE
- Continue routine monitoring, with specific consideration of symptoms and signs of LA toxicity.
- Document the block, including the following information:
- That a ‘‘stop before you block’’ took place13
- Anaesthesia: awake/sedation/ general anaesthetic/spinal anaesthetic
- Side and site of nerve block
- Positioning
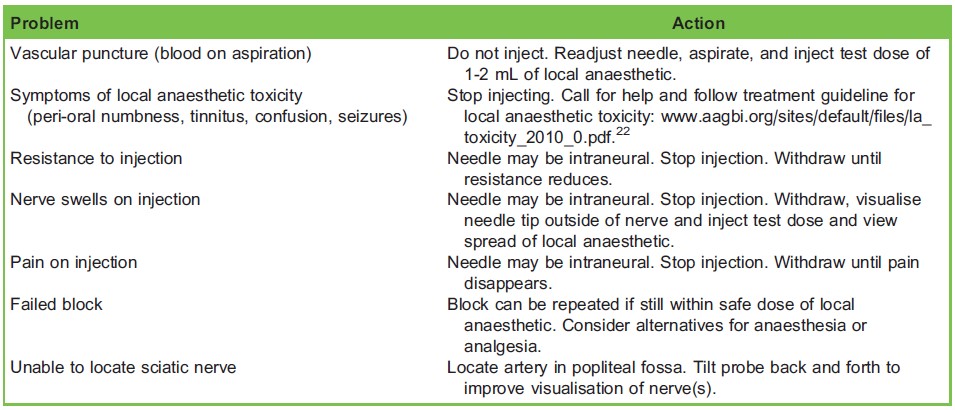
Table 1. Troubleshooting problems during performance of popliteal nerve block
-
- Ultrasound guidance
- In/out of plane
- LA to skin used
- Needle size and type
- Volume, concentration, and type of LA used
- Ease of injection, if pain was present on injection, negative aspiration
- Patients should be followed up postoperatively to ensure that normal sensation has returned at an appropriate time.
CLINICAL TIPS
- Prior to injection, colour Doppler can be used to identify nearby vessels that should be avoided. Squeezing of the calf can help to augment venous flow and help to identify the TN.
- Balloting the vessels with the probe can help to identify the popliteal vein, which may be hidden by pressure from the probe.
- The TN is typically larger and brighter, and lies more medially, close to the vessels.
- Identifying the depth of the nerve and inserting the needle at approximately the same distance away from the probe while needling in-plane will ensure the needle path is horizontal and improve needle visualisation.
- Onset of anaesthesia, if intended for awake regional anaesthesia, can take up to 30 to 45 minutes, and the patient may not demonstrate a profound motor block.
SUMMARY
- Ultrasound-guided popliteal block has been shown to have a higher success rate, require less time to perform, and be associated with less peri-procedural pain when compared to using a nerve stimulator.
- It can provide analgesia and anaesthesia for the entire lower leg when combined with a saphenous nerve block.
- If a tourniquet is required for awake surgery the tourniquet should be applied on the calf.
- A longer period of analgesia can be achieved with the insertion of a continuous popliteal catheter, potentially reducing systemic opioid administration.
ACKNOWLEDGEMENT
We thank Dr David Hay, Specialist Trainee Anaesthesia.
REFERENCES
- Van Geffen GJ, van den Broek E, Braak GJ, Giele JL, Gielen MJ, Scheffer GJ. A prospective randomised controlled trial of ultrasound guided versus nerve stimulation guided distal sciatic nerve block at the popliteal fossa. Anaesth Intensive Care. 2009;37:32-37.
- Tomaszewski KA, Graves MJ, Henry BM, et al. Surgical anatomy of the sciatic nerve: a meta-analysis. J Orthop Res. 2016;34:1820-1827.
- Adibatti M, Sangeetha V. Study on variant anatomy of sciatic nerve. J Clin Diagn Res. 2014;8:AC07-AC09.
- Saleh HAM, El-fark MMO, Abdel-Hamid GA. Anatomical variation of sciatic nerve division in the popliteal fossa and its implication in popliteal nerve blockade. Folia Morphol. 2009;68: 256-259.
- Moore KL, Agur AM. Essential Clinical Anatomy. 2nd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2002.
- Gray H. Gray’s Anatomy of the Human Body 20th ed. (1918). New York, NY: Bartleby; 2000.
- Casati A, Chelly JE, Cerchierini E, et al. Clinical properties of levobupivacaine or racemic bupivacaine for sciatic nerve block. J Clin Anesth. 2002;14:111-114.
- Sinardi D, Marino A, Chillemi S, Siliotti R, Mondello E. Sciatic nerve block with lateral popliteal approach for hallux vagus correction. Comparison between 0.5% bupivacaine and 0.75% ropivacaine. Minerva Anestesiol. 2004;70:625-629.
- Yadeau JT, Lasala VR, Paroli L, et al. Clonidine and analgesic duration after popliteal fossa nerve blockade: randomized, double-blind, placebo-controlled study. Anesth Analg. 2008;106:1916-1920.
- Danelli G, Fanelli A, Ghisi D, et al. Ultrasound vs nerve stimulation multiple injection technique for posterior popliteal sciatic nerve block. Anaesthesia. 2009;64(6):638-642.
- Ehlers L, Jensen JM, Bendtsen TF. Cost-effectiveness of ultrasound vs nerve stimulation guidance for continuous sciatic nerve block. Br J Anaesth. 2012;109:804-808.
- Schnabel A, Meyer-Frießem CH, Zahn PK, et al. Ultrasound compared with nerve stimulation guidance for peripheral nerve catheter placement: a meta-analysis of randomized controlled trials. Br J Anaesth. 2013;111:564-572.
- Safe Anaesthesia Liaison Group. Stop Before You Block. 2011. https://www.rcoa.ac.uk/standards-of-clinical-practice/ wrong-site-block (accessed 01/03/2019)
- Prasad A, Perlas A, Ramlogan R, Brull R, Chan V. Ultrasound-guided popliteal block distal to sciatic nerve bifurcation shortens onset time: a prospective randomised double-blind study. Reg Anesth Pain Med. 2010;35:267-271.
- Brull R, Macfarlane AJR, Parrington S, et al. Is circumferential injection advantageous for ultrasound-guided popliteal sciatic nerve block?: a proof-of-concept study. Reg Anesth Pain Med. 2011;36(30):266-270.
- Karmakar MK, Shariat AN, Pangthipampai P, et al. High-definition ultrasound imaging defines the paraneural sheath and the fascial compartments surrounding the sciatic nerve at the popliteal fossa. Reg Anesth Pain Med. 2013;38:447-451.
- Perlas A, Wong P, Abdallah F, et al. Ultrasound-guided popliteal block through a common paraneural sheath versus conventional injection: a prospective, randomized, double-blind study. Reg Anesth Pain Med. 2013;38:218-225.
- Choquet O, Brault Noble G, Abbal B, et al. Subparaneural versus circumferential extraneural injection at the bifurcation level in ultrasound-guided popliteal sciatic nerve blocks: a prospective, randomized, double-blind study. Reg Anesth Pain Med. 2014;39:306-311.
- Pappin D, Christie I. The Jedi grip: a novel technique for administering local anaesthetic in ultrasound-guided regional anaesthesia. Anaesthesia. 2011;66:840-852.
- Borgeat A, Lambert M, Theodorou P, Vienne P. The feasibility and complications of the continuous popliteal nerve block: a 1001 case survey. Anesth Analg. 2006;103:229-233.
- Cappelleri G, Cedrati VLE, Fedele LL, et al. Effects of the intraneural and subparaneural ultrasound-guided popliteal sciatic nerve block: a prospective, randomized, double-blind clinical and electrophysiological comparison. Reg Anesth Pain Med. 2016;41:430-437.
- Cave G, Harrop-Griffiths W, Harvey M, et al. Management of Severe Local Anaesthetic Toxicity. AAGBI Safety Guideline 2010.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/