Basic Sciences

QUESTIONS
- The following is true about magnetic fields:
- MRI scanners generate magnetic fields between 0.2 and 3.0 Tesla
- 1 Tesla is the equivalent of 10 000 Gauss
- The Earth’s magnetic field is approximately 0.5 – 1 Gauss
- MRI superconductor coils are immersed in liquid oxygen in order to keep them below 4.2 Kelvin
- The strength of the magnetic field remains the same as you move away from an MRI scanner
- With regards to magnetic resonance imaging:
- The T-weighting of an image refers to the exact dosage of contrast agent given to the patient.
- In T1 weighted images fluid structures will appear darker
- In T2 weighted images fluid structures will appear white
- The negative charge of the hydrogen atom in water is most commonly used to generate MR images
- The contrast agent Gd-DTPA can commonly cause anaphylaxis in patients undergoing MRI scans
- The following are significant safety concerns in the MRI examination room:
- Patient injury from metal projectiles
- Hypothermia due to the cold environment
- Burn wounds related to equipment cables
- Anaphylaxis from the use of intravenous contrast agent
- Hearing damage due to high noise levels
- With regards to the management of patients for MR imaging:
- In the event of a cardiac arrest, the magnet should be switched off in order for safe resuscitation to take place
- Patients with neurovascular aneurysm clips should never have MRI scans
- Cardiac pacemakers are at significant risk of failure within the 5 Gauss line
- Patients with angina should keep their GTN patches on during anaesthesia for MRI scans
- Intensive care patients should not have MRI if their tracheal tube contains a metal spring in the pilot balloon
INTRODUCTION
Magnetic resonance imaging (MRI) produces high quality images of the body in cross section and in three-dimension. It detects the effects of induced changes in the nuclei of specific elements within the body and is particularly useful for the imaging of soft tissues, providing greater contrast between different types of soft tissue than computerised tomography (CT). It is the technique of choice for many neurological, cardiovascular, oncological and musculoskeletal conditions.
ESSENTIAL KNOWLEDGE FOR MAGNETIC RESONANCE IMAGING
The physics of magnetic resonance imaging
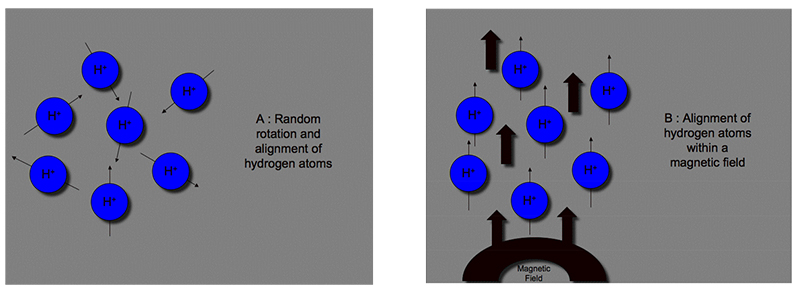
MRI relies on the fact that some atoms within the human body possess an odd unpaired proton. The proton nucleus of the hydrogen atom is one of the most abundant examples, being a major constituent of water. It responds particularly well to the application of an external magnetic field and is therefore one of the simplest atom to use for MRI. Another example is phosphorus, which as a component of adenosine triphosphate, allows for many metabolic processes to be studied.
These nuclei possess a spin that results in a local magnetic field because of their charge, allowing them to act like small magnets. The alignment of these nuclei is usually random (Figure A), however when a strong electromagnetic field is applied to the body they align themselves with that field. (Figure B)
These nuclei can be turned out of alignment with the magnetic field by applying brief bursts of radio- frequency energy, creating an electromagnetic field perpendicular to the first magnetic field. When the electromagnetic field is removed, the radio-frequency energy taken up by the nuclei is released slowly as they relax back into alignment. The rate at which realignment takes place depends on the type of nucleus, or element being measured, and thus the emitted signal depends on the molecular properties of the tissue.1
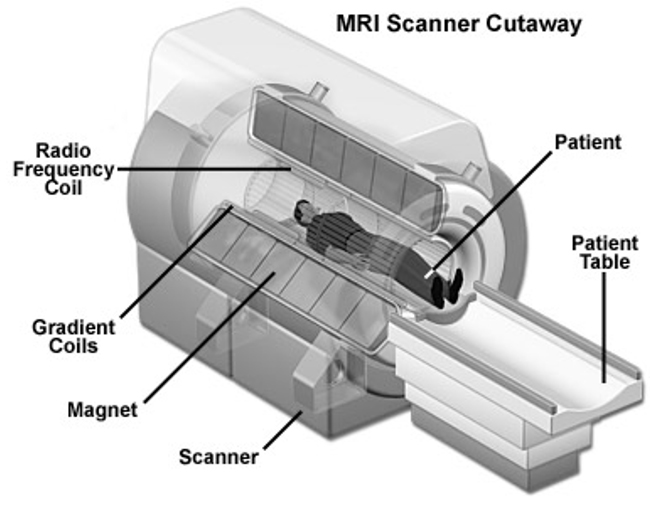
This low radiofrequency radiation that is emitted induces an electrical signal within a set of three orthogonal gradient coils in the MRI machine. They are positioned in the transverse (X and Y) and longitudinal (Z) planes allowing for encoding of spatial information. The detected signals are therefore able to form a three-dimensional image of the body. It is these gradient coils that are rapidly turned on and off during an MRI study that is responsible for the loud banging noises.2
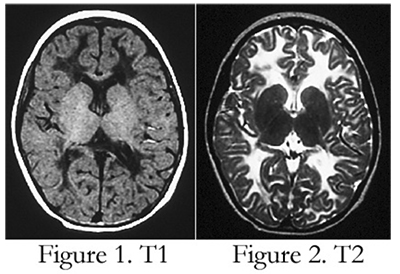
Different tissues within the body have different relaxation rates. ‘T’ refers to the relaxation time constant, and images may be T1 weighted (generated a few milliseconds after the electromagnetic field is removed) or T2 weighted (generated later than T1), depending on the characteristics of the tissue you wish to look at. Nuclei in hydrogen take a long time to decay to their original position, so fluid will appear dark (minimal signal) in a T1 weighted (early) image (Figure 1), but white in the later T2 image as the signal appears. 3 (Figure 2)
Because the signal that makes up the final MR image is very weak, any external radiofrequency sources can greatly interfere with its detection by the gradient coils. To prevent this the MRI machine is contained within a radiofrequency shield called a Faraday cage. This is built into the fabric of the MR room. To allow infusion lines or monitoring cables to enter the MR room, a hollow brass tube or ‘waveguide’ is built into the Faraday cage passing through into the control room.2
The Magnetic field
MRI requires strong magnetic fields between 0.2 and 3.0 Tesla that are generated by superconductors. To minimise the electrical resistance of the superconducting coils, they are immersed in liquid helium and cooled to below 4.2 Kelvin.1
1 Tesla = 10 000 Gauss (Earth’s magnetic field = 0.5 – 1.0 Gauss)
= 1 weber/m2
The magnetic field strength falls away exponentially from the magnet. A safety line is usually demarcated at the level of 0.5mTesla (5 Gauss) within which pacemakers will malfunction, and therefore unscreened personnel should not enter (see hazards section below).2
A second line is demarcated at 50 Gauss within which a significant attractive force will be encountered on all ferromagnetic objects, which risk becoming dangerous projectiles. Such items include gas cylinders, needles, watches, floor cleaners and patient trolleys. Within this line anaesthetic infusion pumps (or any electronic or mechanical equipment) may fail due to the effects of the magnetic field.2
While these lines of demarcation are often referred to theoretically, in practice many MRI units are simply divided into a ‘safe zone’ outside the scanner, and the controlled ‘hazardous zone’ within the MR examination room.
INDICATIONS FOR THE USE OF MAGNETIC RESONANCE IMAGING
MRI is usually the preferred imaging technique in the following cases:
- Posterior fossa and infratentorial pathology
- Sinus and orbit pathology, sensorineural hearing loss and cranial nerve pathology
- Cerebral inflammatory disease including encephalitis, myelitis and meningitis
- Brain abscess
- Acute ischaemic strokes
- Spinal cord soft tissue pathology including congenital, traumatic, neoplastic and vascular abnormalities and disc pathology
- Demyelinisation and the myelopathies
- Airway malformations
- Vascular malformations
- Liver vascular pathology
- Joint soft tissue pathology
CT scanning remains more useful for bony pathology, chest examinations, intracranial haemorrhage and abdominal and pelvic applications
HAZARDS AND SAFETY CONSIDERATIONS FOR PATIENTS AND STAFF IN THE MRI UNIT
1. The presence of a strong magnetic field
The strong magnetic field poses by far the most important hazard related to anaesthesia and care of patients requiring MRI. These powerful magnetic fields are able to exert large forces on any ferromagnetic materials in close proximity. They may also induce currents in metallic objects causing local heating and may interfere with monitoring equipment. Conversely, ferromagnetic objects and electrical fields in the vicinity of the magnet will degrade the quality of the MR images produced. The safety aspects related to ferromagnetic objects as projectiles, implants, foreign bodies and as equipment will be discussed in further detail below.
The human body is conductive and movement of the body within the magnetic field will induce weak electrical currents within the tissues. Movement of blood around the body will also result in the generation of electric potentials and current.1 These currents can cause symptoms such as nausea and vertigo as a result of excitation of the semicircular canals of the inner ear, or flashing lights due to their effects on the retina.4 The patient as well as the staff positioning a patient in the scanner and moving within the immediate vicinity of the magnet bore may occasionally notice these effects.
There is currently no evidence that long-term repeated exposure to strong magnetic fields has a harmful effect on the human body, however current recommendations suggest that a time-weighted average of 200mT over any 8-hour period should not be exceeded by healthcare personnel.4 Ideally all staff should vacate the MRI examination room whilst the scan is in progress.
2. Ferromagnetic objects and the projectile effect
The attractive forces between the magnet and all ferromagnetic objects increase significantly as such objects are brought closer to the magnet. All ferromagnetic items brought within the 50 Gauss line will be subject to movement and may be rapidly accelerated into the magnetic field. Objects that are not fixed down therefore risk becoming dangerous projectiles and may cause injury to anyone in their path, as well as damage to equipment, and interference with the MR image generated.1,2,4
All staff should be fully aware of the dangers of metal objects in the scanner, and before entering the controlled area of the examination room need to remove all ferromagnetic, metallic or conducting materials from their person. Magnetised items such as credit cards and mobile phone SIM cards are at risk of being damaged by proximity to the magnetic field.
Before entering the examination room with an anaesthetised patient a careful inspection for metallic objects should be made. Items that typically might contain metals include needles, watches and jewellery, pagers, stethoscopes, anaesthetic gas cylinders, metallic trolleys, ECG electrodes, transdermal drug patches (GTN) and ventilator systems.2 After hours, floor polishers are particularly common projectiles.

3. Implants and foreign bodies
Ferromagnetic materials may also be present inside the body and are subject to similar forces that can cause them to move or malfunction with potentially fatal consequences. Implanted ferromagnetic objects may also heat up significantly during the MR examination causing local tissue damage.
Absolute contraindications to MRI include cochlear implants, intra-ocular metallic foreign bodies or shrapnel, or ferromagnetic arterial or aneurysm clips particularly neurovascular.2 Patients with cardiac pacemakers or implanted defibrillators must never undergo an MRI scan since these will malfunction within the 5 Gauss line.2
Most modern patient implants, including metal prostheses, are non-ferromagnetic. General surgical clips, artificial heart valves and sternal wires are usually deemed safe since they are fixed by fibrous tissue.2 Nonetheless, no patient should ever enter an MR examination room if there is any doubt about the safely of an implanted device or foreign body.
All patients therefore need to be screened prior to the MRI scan for the presence of metallic implants. This is the responsibility of the radiology staff, however all staff working within the MRI unit should be aware of these risks. The same precautions regarding foreign bodies and implanted devices apply to all hospital staff that work near the MRI scanner.4 Usually a standard screening questionnaire or ‘metal check’ will suffice, however X-rays may be used to search for metal implants if any doubt exists. The compatibility of any implanted devices with the MR scanner may be confirmed online via websites such as www.mrisafety.com
4. Equipment and monitoring issues
All anaesthetic equipment and monitoring in the MR room should be MRI compatible. An important distinction exists between equipment that is designated ‘MRI safe’ and that which is designated ‘MRI compatible’. MRI safe implies that a piece of equipment will not pose a danger to patients and staff if it enters an MRI examination room, but does not guarantee that it will function correctly or avoid degrading the image quality. MRI compatible equipment is both safe to enter the MR examination room and will operate normally within that environment without interference to the MR scanner.4 It is reasonable to deduce that all anaesthetic equipment used within the MRI examination room should therefore be MRI compatible.
Where non-compatible equipment is used within the magnetic field they may pose serious hazards to the patient – they may become projectile, cause burns if heated cables come in contact with the patient, or they may malfunction.4
In the past ferrous anaesthetic machines remained in the MR control room and anaesthetic breathing systems such as the co-axial Mapleson D or Bain circuit extended through the waveguide ports to the patient. MR compatible anaesthetic machines, ventilators and vaporisers are now available from most manufacturers and should be used instead.4 Anaesthetic breathing systems including the circle system, Bain circuit or Ayres T piece for children have all been used successfully.2 Piped gasses with back up cylinders made of a non-ferrous metal such as aluminium should be available.
Although MR compatible equipment is likely to be more fragile and costly it is essential that minimal monitoring standards for routine anaesthesia are complied with. Suppliers often provide basic MR compatible monitors as part of the system.
The anaesthetist must be aware of the fact that MR can interfere with accurate monitoring and monitors can similarly interfere with the MRI. The changing gradient fields and radiofrequency currents used for MRI can induce currents in monitoring leads. These can cause burns to the patient as well as interference with the monitoring.2,4 Fibre-optic or carbon fibre cabling should avoid this problem, however care must still be taken to avoid coiling of cables within the scanner, and padding should be placed between all leads and the patient’s skin.4 The converse applies too, and monitors should not emit radiofrequencies that might interfere with the image quality.5 Mains power supply should be isolated or filtered, or battery power used. Batteries are ferromagnetic, and if used, the relevant equipment should be firmly secured.2
Monitoring screens should be present in the MR control room to allow for remote monitoring of the patient so that the anaesthetist can leave the MR examination room. Monitoring cables can be passed through the waveguide ports to facilitate this. All alarms should be visual because of the noise made by the MR scanner, and the view of the monitor, anaesthetic machine and patient should be unobstructed at all times.
Electrocardiogram (ECG) monitoring cannot occur with standard electrodes and MR compatible electrodes are needed. They should be placed in a narrow triangle on the patient’s chest, and leads should be braided and short (15cm). Currents induced by blood flow through the transverse aorta will interfere with the ECG signal causing artefact in the ST-T complexes which mimics hyperkalaemia.2,4
Pulse oximeter cables should be insulated and placed as far from the scanner as possible. Finger burns have been reported with standard non-compatible pulse oximeters.2
Non-invasive blood pressure monitoring is possible if connectors are changed to plastic, and invasive pressure monitoring is possible if the pressure transducer cabling is passed through the waveguides.6 MR compatible pressure transducers are available.
Capnography and monitoring of airway pressures and gasses requires a longer sample tubing than is routine, this results in approximately a 20 second delay, which the anaesthetist should take into consideration.
Infusion pumps may fail if close to the magnet where the magnetic field strength exceeds 50 Gauss.2
5. Restricted access of the environment
The MR scanner is designed to place the patient in the centre of the magnetic field within the bore of the magnet. As a result the patient is effectively enclosed within a narrow tube to which access is extremely limited. Newer designs include open C shaped magnets that are less claustrophobic for the awake patient and allow improved access, however these are only suitable for limited investigations as they do not allow such detailed investigations and the duration of the scans is longer.2
Not only is the patient access restricted, but also the MRI suite itself is an environment in which only suitably trained staff should be working. It is often located at a distance from the hospital’s theatre facilities making readily available backup and assistance less likely.
6. High level acoustic noise
Noise levels above the safe level of 85 decibels can be produced during MRI due to the rapid switching of the gradient coils.2,4 The exact magnitude of this noise depends on the sequence of images being collected and the strength of the magnetic field.
Staff working in MRI units should protect themselves by remaining in the MR control room during sequence acquisition, or by wearing earplugs should they need to remain in the examination room.
All patients should be given ear protection, regardless of if they are awake or anaesthetised.2,4
The anaesthetist should be aware that high ambient noise levels may mask normal auditory alerts such as monitor alarms or sound the sound of partial airway obstruction, so vigilance and attention to visual cues is essential.7
7. Scavenging of anaesthetic gasses
Volatile anaesthetic agents and nitrous oxide may be used for general anaesthesia in MR units. MR compatible scavenging systems are available and these gases should therefore be scavenged in the usual way to comply with the local regulations for these substances.4 (Control of Substances Hazardous to Health or COSHH regulations in the United Kingdom)
8. Quenching of superconducting magnets
The coils used in MR magnets need to be kept cold in order to maintain superconductivity. This is achieved by immersing them in liquid coolants or cryogens, liquid helium being the most commonly used in modern MRI units.
Quenching is a process involving the rapid boil-off of the cryogen that causes an immediate loss of superconductivity. This may occur spontaneously as a system error during installation, services and power ups, or may be deliberately induced in order to shutdown the magnetic field.4 If this happens, the magnetic field will be lost and a large volume of helium gas will be produced. This is normally vented to the outside atmosphere through a quench pipe.
In the event of damage to the quench pipe, the build-up of helium within the scanning room could potentially lead to asphyxiation. Oxygen sensors must be present in the scanning room to alert the staff in the control room to a hypoxic environment. All Staff working in an MRI unit should be aware of the emergency procedures for quenching.4
9. Hazards of MRI during pregnancy
The MRI unit may pose hazards to the developing foetus, including exposure to strong magnetic fields, high noise levels and unscavenged anaesthetic gases. Although limited evidence exists, in the United Kingdom it is currently recommended that pregnant women should ideally not be scanned during the first trimester of pregnancy.4
Pregnant staff working within the MRI unit should be advised of the risks posed by this environment, and given the option of not entering the inner controlled area during their first trimester.
10. Use of contrast agents
The most commonly used intravenous MR contrast agent is gadolinium dimeglumine (Gd-DTPA or Magnevist). It is used to increase the signal intensity on T1 weighted scans and reduce the signal intensity on T2 weighted scans. It is often used in contrast-enhanced MR angiography and to help identify tumours. Since it does not normally cross the blood brain barrier it may be used to demonstrate areas where it has broken down and to delineate intracranial pathology.2
Gd-DTPA is used in doses of 0.2 ml/kg and has minor side effects including nausea, vomiting and pain on injection. There are rare complications of gadolinium called nephrogenic systemic fibrosis or nephrogenic fibrosing dermopathy, seen in association with renal impairment; all patients should have an assessment of renal function before MRI, either by history or by urea and creatinine assay. There has been one incidence of anaphylactoid reaction reported.4
11. Maintenance of body temperature
A theoretical problem during sedation or anaesthesia of infants and neonates for MRI is the maintenance of body temperature within this cooled environment. Passive heat loss should be prevented by minimizing exposure and by returning the infant to a warm environment as soon as possible.2
Recent studies examining the effect of MRI on body core temperature in sedated infants and children have suggested that this problem is not as significant as once thought. Radiofrequency radiation produced by the MR scanner and absorbed by the patient causes an increase in body temperature, suggesting that active heating is unnecessary and may in fact cause hyperthermia. This rise in temperature was more profound in 3 T than in 1.5 T examinations.8
PATIENT MANAGEMENT FOR MAGNETIC RESONANCE IMAGING
Magnetic resonance imaging requires a patient to lie still in a noisy and restricted space for prolonged periods of time. By far the greater majority of patients should be able to achieve this without the intervention of an anaesthetist. Understandably this may not be possible for certain groups of patients, particularly young children.
All cases referred for general anaesthesia should be evaluated and have the risks of anaesthesia weighed against the benefits of the investigation. Not all patients require general anaesthesia. For example, with regards to infants and children, other management strategies may be commonly utilised:
- Behavioural techniques, including reassurance, communication through informative booklets, videos and visits to the unit, rehearsal of scans and the skills of play specialists.9
- Natural sleep techniques, including the ‘feed and wrap’ method for neonates, and sleep deprivation prior to a scan for toddlers.9
- Sedation techniques, lead by specialist and experienced nurse lead sedation services have been shown to be both highly successful and very safe.10
The following groups2,4 are more likely to require general anaesthesia:
- Infants and children
- Patients with learning difficulties
- Patients with certain seizure or movement disorders
- Patients with claustrophobia
- Critically ill patients
- Patients undergoing neurological examinations, particularly where raised intracranial pressure is a concern (sedation is contraindicated as it can be potentially dangerous)
CONDUCT OF GENERAL ANAESTHESIA FOR MRI
All patients for MRI should be pre-assessed by their anaesthetist and starvation guidelines should be the same as for any general anaesthetic. A metal check must be performed by the radiology staff prior to induction of anaesthesia. The choice of anaesthesia technique depends on factors such as the length of the scan, the age of the child, associated co-morbidities such as raised intracranial pressure, or the need for a breath hold as for cardiac MRI scans. Small infants <5kg that require anaesthesia are best managed by intubation and ventilation; older children may be managed by spontaneous ventilation with an LMA.
Induction of anaesthesia should occur in a dedicated room adjacent to the MR examination room. This induction room should contain all standard anaesthetic equipment, monitoring, drugs and resuscitation equipment. It can also be used as a post anaesthesia recovery area if necessary. Prior to induction, patients should be placed on a non-ferrous trolley (without oxygen cylinders) so that they can be safely transferred to the MR room once they are anaesthetised. Before this transfer a brief second metal check should occur to look for loose objects such as needles, oxygen cylinders and stethoscopes etc, which may have strayed onto the patient’s trolley.
In the MR examination room the patient can be transferred onto the MRI scanner and maintenance of anaesthesia and monitoring should be recommenced immediately. A check to ensure that the airway is secure is important since once inside the scanner, the patient will be relatively inaccessible. Patients having head scans will have a receiver coil placed over their heads, which further reduces access. Maintenance of anaesthesia may be either inhalational or intravenous.2 If volatiles are given, the vaporiser should be MR compatible. TIVA is an acceptable technique for MRI, but some infusion pumps may act as projectiles or malfunction close to the magnetic field. Keeping these pumps in the control room and passing the connecting lines through the waveguide will avoid this. Ear protection should be provided for the patient prior to commencing the scan, and should be removed before waking them up. The anaesthetist may then exit the MR examination room and monitor the patient from the control room if the facilities for this exist.
Once the study has been completed, the patient should be removed from the scanner and be woken up and recovered in a suitable recovery area. Analgesia is unlikely to be required for MRI scanning, although paracetamol may be useful if the child has a sore throat or is complaining of headache. Many children may be managed as day cases for MRI scans, depending on their associated co-morbidities, and may be discharged from the recovery or ward area once they meet the normal discharge criteria for day case procedures.
CONSENT FOR ANAESTHESIA FOR MRI
Unlike anaesthesia for invasive surgical procedures where the consent for anaesthesia is implied by the act of consenting for the surgery, and contrary to routine MRI where written consent is not required, the consent for MRI under general anaesthesia remains a complex issue. In order to obtain truly informed consent input should ideally be provided from the referring clinician who has requested the investigation, the radiologist who is performing the scan, and the anaesthetist responsible for the general anaesthesia.11
Recent review of this issue has suggested that it is the referring clinician who is best suited to explain the intended benefits, side effects and risks of the procedure, and thus to obtain written consent.11
Nevertheless it remains incumbent upon the responsible anaesthetist to review the anaesthetic plan and risks with the patient prior to the procedure.
EMERGENCIES IN THE MRI SUITE
Owing to the presence of a strong magnetic field and the risk of projectiles, as well as the restricted access imposed by the MRI scanner, it is impossible to manage emergencies and resuscitation within the scanning room and 5 Gauss line.
In the event of an emergency the patient should be removed from the magnetic field as quickly as possible and transferred to the induction room, which should be close to the scanner and will contain the necessary anaesthetic and resuscitation equipment and drugs.4
The resuscitation team should know not to enter the 5 Gauss line of the inner controlled area, and in the event of an emergency should be directed by radiology staff to the induction/resuscitation room.
INTENSIVE CARE PATIENTS REQUIRING MRI
MRI of critically ill adults and children is becoming both an important diagnostic and prognostic tool. These patients require special expertise, planning and time to be safely examined by MR.12
One notable challenge includes the multiple drug infusions that these patients might require, inotropic therapy being of particular concern. All unnecessary infusions should be discontinued. Those that are required should be infused through extensions of adequate length, which can be passed through the ‘waveguide’ to a pump remaining in the MR control room. Non-compatible MR syringe drivers used within the MR examination room may deliver incorrect drug doses with significant patient safety dangers.2 If MR compatible infusion pumps exist they may be used in the MR examination room, however the anaesthetist may need to remain in the room if the pumps rate needs to be changed.
Critically ill patients also require a higher standard of monitoring. All monitoring equipment should be changed to MR compatible versions within the anaesthetic induction room before entering the MR examination room. Arterial pressure transducers can be passed through the waveguide if not compatible.6 Pulmonary artery catheters with conductive wires in contact with heart muscle and epicardial pacing wires pose a theoretical risk of micro-shock; these should be removed prior to the examination. Central venous catheters pose no risk to the patient. All in-dwelling catheters should be disconnected from electrical connections and external accessories before entering the MR examination room.13
Lastly, care should be taken to ensure that no surgical interventions undertaken have left the patient with internal metal work. Often where the patient’s history is vague, a pre-MR X-ray screen might be required. Many tracheostomy tubes are not MR compatible and will need to be changed prior to the examination. The pilot balloons of cuffed tracheal tubes may contain a small ferromagnetic spring that will need to be taped securely away from the area being scanned.2
CONCLUSION
MRI is now a routine investigation, and as the demand for MRI scans increases so will the need for general anaesthesia in this environment and for MRI scans of more challenging patients. New scanning techniques are being developed in the areas of orthopaedic soft tissue imaging and dynamic cardiac imaging.14 Operating theatres and intensive care units incorporating open MRI scanners are being developed and introduced.15 Scanners that permit access to the patient allow for perioperative scanning. This is an area of anaesthetic practice that will grow in the future, and in order to maintain the current levels of patient care and safety, all anaesthetists should remain familiar with the challenges posed by this unique environment.
SELF-ASSESSMENT ANSWERS
- Question 1
- True
- True
- True
- False – superconductor coils are immersed in liquid helium to maintain a low temperature
- False – the strength of a magnetic field decreases exponentially as one moves away from the scanner
- Question 2
- False – T weighting refers to the relaxation time constant of the atom being used in the MRI study
- True
- True
- False – Hydrogen has a positive charge that is used as the basis for most MRI studies
- False – There is a very low risk of anaphylaxis with the contract agent Gd-DTPA
- Question 3
- True
- False – Hypothermia is uncommon, and MRI may cause the patients temperature to increase
- True
- False – Anaphylaxis with Gd-DTPA is uncommon
- True
- Question 4
- False – In the event of a cardiac arrest the patient should be moved quickly to the induction (anaesthetic?) area for resuscitation. Switching the magnet off will cause quenching and put the resuscitation team at risk
- True
- True
- False – GTN patches should be removed prior to MRI scanning
- False – The metal spring in the pilot balloons of tracheal tubes may be used in the MRI scanner, but should be taped away from the area being studied. Armoured ETT’s with a metal coil down their length should not be used due to the risk of dislodgement from the magnetic pull on the metal and because the metal interferes with/distorts the MRI image produced.
ONLINE RESOURCES
- Guidance to the compatibility of medical devices within the MRI unit. http://www.mrisafety.com
- The association of Anaesthetists of Great Britain and Ireland: Provision of Anaesthetic services in Magnetic Resonance Units. http://www.aagbi.org/publications/guidelines/docs/mri02.pdf
REFERENCES
- Davis PD, Kenny GNC. Basic Physics and Measurement in Anaesthesia, Fifth Edition. Butterworth – Heinemann, 2002; 269 – 71
- Peden CJ, Twigg SJ. Anaesthesia for magnetic resonance imaging. Continuing Education in Anaesthesia, Critical Care and Pain. 2003; 3: 97 – 101
- Bricker S. The Anaesthesia Science Viva book, First edition. Greenwich Medical Media Ltd, 2004; 256 – 57
- Association of Anaesthetists of Great Britain and Ireland. Provision of anaesthetic services in magnetic resonance units. May 2002. Website: www.aagbi.com
- Roth JL, Nugent m et al. Patient monitoring during Magnetic resonance imaging. Anaesthesiology. 1985; 62: 80 – 83
- Taber KH, Thompson J et al. Invasive pressure monitoring of patients during magnetic resonance imaging. Canadian Journal of Anaesthesia. 1993; 40: 1092 – 5
- Sesay M, Tauzin-Fin P et al. Audibility of anaesthesia alarms during magnetic resonance imaging: should we be alarmed? European Journal of Anaesthesiology. 2009; 26: 117 – 122
- Machata AM, Willschke H et al. Effect of brain magnetic resonance imaging on body core temperature in sedated infants and children. British Journal of Anaesthesia. 2009; 102: 385 –9
- Sury MRJ, Harker H et al. The management of infants and children for painless imaging. Clinical Radiology. 2005; 60: 731 – 741
- Sury MRJ, Hatch DJ et al. Development of a nurse-led sedation service for paediatric magnetic resonance imaging. The Lancet. 1999; 353:1667 – 71
- Wellesly H, Chong WK, Segar P. Who should obtain written consent for magnetic resonance imaging under general anesthesia? Pediatric Anesthesia. 2009; 19: 961 – 63
- Tobin JR, Spurrier EA, Wetzel RC. Anaesthesia for critically ill children during Magnetic Resonance Imaging. British Journal of Anaesthesia. 1992; 69: 482 – 86
- Kampen J, Tonner PH, Scholz J. Patient safety during anaesthesia for magnetic resonance imaging. European Journal of Anaesthesiology. 2004; 21: 320 – 35
- Odegard KC, DiNardo JA et al. Anaesthesia considerations for cardiac MRI in infants and small children. Paediatric Anaesthesia. 2004; 14: 471 – 6
- Whitby EH, Paley MN et al. Low field strength magnetic resonance imaging of the neonatal brain. Archives of diseases in childhood. 2003; 88: 203 – 8
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/