Intensive Care Medicine

KEY POINTS
- Dexmedetomidine is a highly selective alpha-2 adrenoceptor agonist.
- It is a safe sedative agent that has useful analgesic and anxiolytic effects.
- It has a particular role in facilitating weaning from the ventilator and extubation, especially when standard sedation strategies have proven ineffective.
- Clinical trials have demonstrated that the benefits of dexmedetomidine compared with other more traditional agents for critical care sedation include reductions in time to extubation, duration of mechanical ventilation, and length of critical care stay.
- Bradycardia is the main recognised side effect, and there are few absolute contraindications.
INTRODUCTION
Dexmedetomidine is an alpha-2 adrenergic receptor agonist that is increasingly being recognised as an alternative sedative agent in critical care medicine. This article will discuss the relevant pharmacology and the suggested benefits of dexmedetomidine. The currently available evidence supporting its use will be appraised. The article will not discuss alternative
uses of dexmedetomidine, for example, as a sedative agent in anaesthetic practice.
PHARMACOLOGY
Dexmedetomidine is an imidazole-derivative drug. It is prepared as an isotonic solution for intravenous injection, in a range of ampoule sizes, all intended for dilution to concentrations of either 4 lg/mL or 8 lg/mL1.
Indications for Use
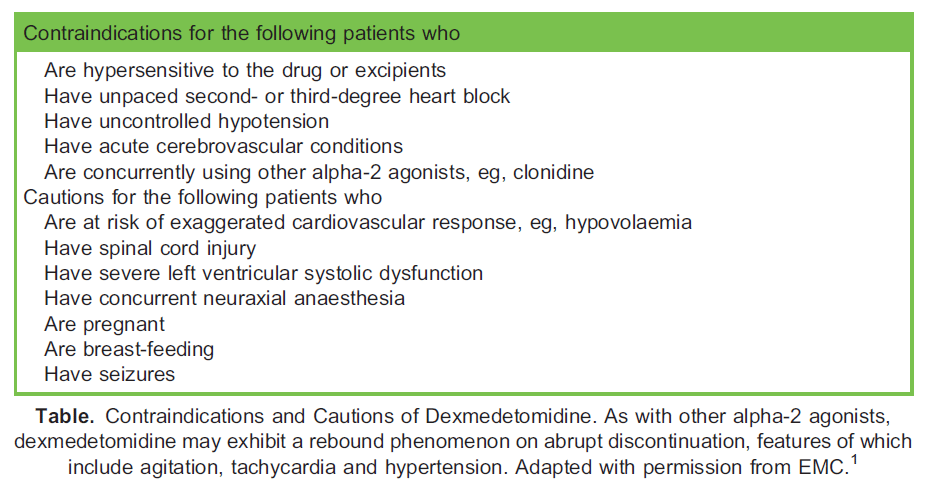
Dexmedetomidine was approved in the European Union in 2011 for use as a sedative agent for adult critical care patients requiring a level of sedation not deeper than a Richmond Agitation-Sedation Score (RASS) of – 3 (ie, arousal in response to verbal stimulation).2 A secondary indication, licensed in 2018, is for awake procedural sedation in patients whose tracheas have not been intubated.3 Evidence has also supported the unlicensed use in children for sedation in intensive care and for procedural sedation.4 The Table lists the contraindications and cautions for dexmedetomidine.
In the United Kingdom, many critical care units use dexmedetomidine as a second-line drug, where weaning from sedation and mechanical ventilation have been or are anticipated to be difficult. Dexmedetomidine has been found to have a particular role in facilitating extubation in severely agitated patients, including those who have been under the influence of novel illicit
psychoactive drugs. Usage in this circumstance often requires a higher dosing of dexmedetomidine.5
Mechanism of Action
Dexmedetomidine is a highly selective alpha-2 receptor agonist. Its major sympatholytic and sedative actions are mediated primarily via reduced transmission in the locus coeruleus, the major noradrenergic centre of the central nervous system.
Because of this, it has been argued that sedation induced by dexmedetomidine is more akin to natural sleep compared with other commonly available sedative agents, such as propofol. In addition, because of its selective pharmacodynamics, it causes anxiolysis and sedation, but largely without the respiratory depression seen with most other sedative agents. Importantly, it also produces spinal and supraspinal analgesia, via reduced nociceptive transmission, according to the gate theory. This accounts for its valuable opioid-sparing effect.
Effects on other organs are few but include a dose-dependent reduction in mean arterial pressure and heart rate, a suspected reduction in cerebral blood flow and a clinically insignificant increase in PaCO2 and nausea. The incidence of nausea has been suggested to be between 1% and 10%.1 Dexmedetomidine has not been shown to impair adrenal steroid synthesis.6
Dosing and Administration
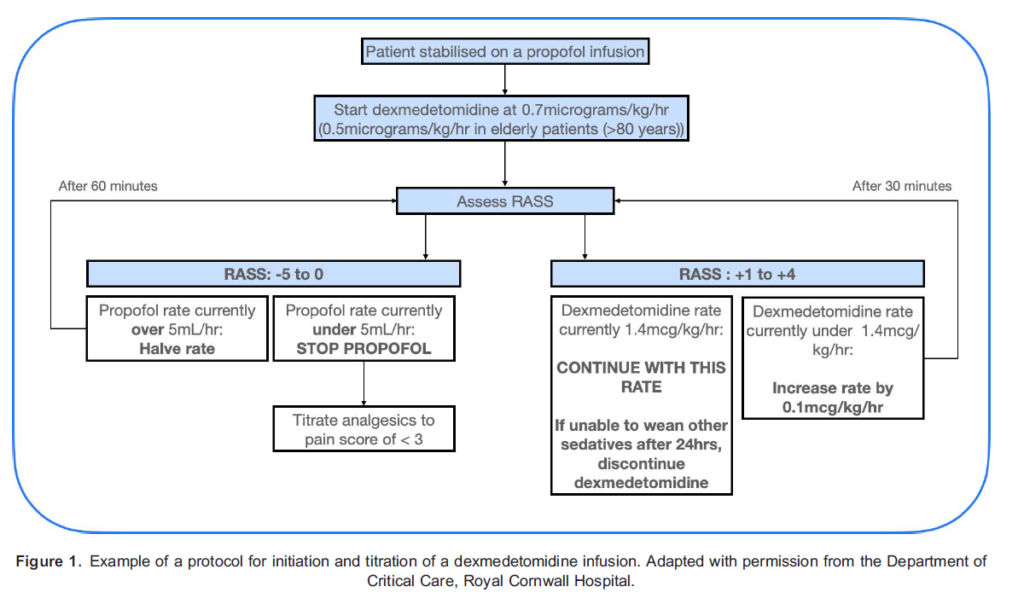
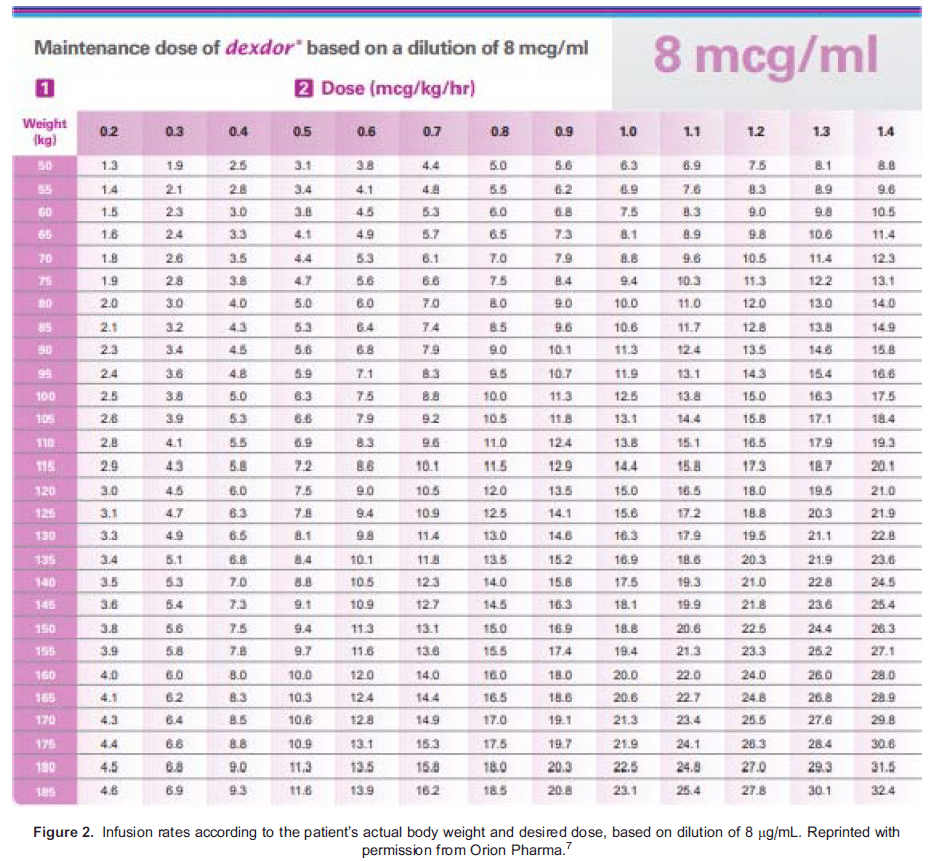
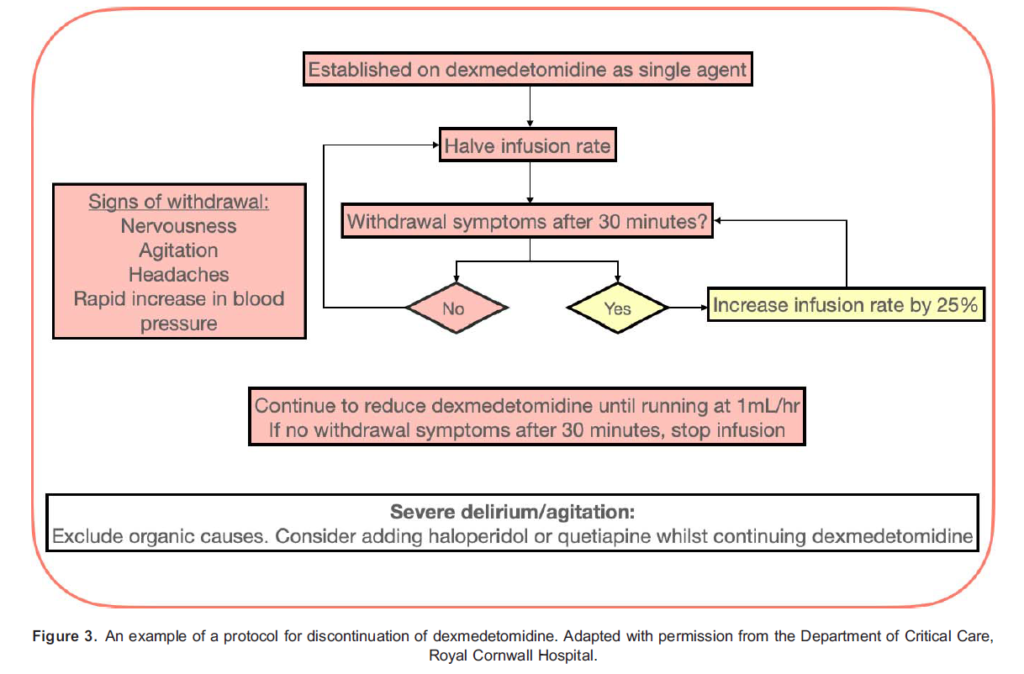
Dexmedetomidine is administered intravenously. When used as a second-line agent, it is started in patients who have already been established on sedative infusions and mechanical ventilation. Under these circumstances, dexmedetomidine should be commenced at an infusion rate of 0.7 lg/kg/h, using actual body weight. It should then be titrated gradually to the desired level of sedation within the range of 0.2 to 1.4 lg/kg/h.7 UK licensing information does not recommend the use of a loading bolus, and steady state is achieved in 1 hour.1 Notably, the unique properties of dexmedetomidine permit it to be continued at a lower dose during and immediately after extubation. Figures 1, 2, and 3, respectively, provide further information on initiation, dosing and discontinuation of dexmedetomidine.
Pharmacokinetics
Dexmedetomidine exhibits a 2-compartment model, with a distribution half-life of 6 minutes. It exhibits linear pharmacokinetics and it has been shown, within the recommended range given above, not to accumulate in treatments lasting up to 14 days. It is 94% protein bound, binding primarily to serum albumin, with a constant degree of binding over a wide range of serum albumin levels. Volume of distribution at steady state is estimated at between 1.1 and 2.1 l/kg.
Dexmedetomidine is extensively hepatically metabolised, including via the CYP450 system. All metabolites have negligible pharmacological activity. Ninety-five percent of an administered dose is renally excreted, with the remainder excreted via the gut.
There is no requirement for dose adjustment in severe renal failure, but those with significantly impaired hepatic synthetic function may be exposed to increased free drug fractions, leading to prolonged elimination half-life, from approximately 1.9 to 2.5 hours in the healthy subject to up to 7.4 hours in those with severe hepatic impairment.1 For this reason, it is suggested that despite dexmedetomidine being titrated to effect, it may still be prudent to reduce maintenance doses in patients with hepatic impairment.
Monitoring Requirements
Patients receiving a dexmedetomidine infusion require continuous electrocardiogram, respiration and blood pressure monitoring. If noninvasive blood pressure monitoring is used, the minimum cycle time should be 5 minutes. Two-hourly sedation scores should be performed to aid titration, and the Confusion Assessment Method for the Intensive Care Unit (ICU) delirium scoring should be performed at least every 12 hours.1 There is no requirement to measure serum drug levels.
REVIEW OF CURRENT LITERATURE
Many critical care patients require a period of sedation, often to facilitate mechanical ventilation via an oral endotracheal tube. Traditional sedation regimens, such as propofol with an opioid, are associated with a high incidence of side effects, including prolonged mechanical ventilation,8 coma,9 delirium,9 posttraumatic stress,10 and increased economic costs.11 It has been suggested that dexmedetomidine, because of its different mechanisms of action and properties, may have an improved side effect profile. Available studies comparing dexmedetomidine to alternative regimens for a number of different variables are appraised.
Reduced Critical Care Length of Stay, Duration of Mechanical Ventilation and Time to Extubation
In a parallel-design trial by Jakob et al,12 patients were randomised to either dexmedetomidine versus propofol (PRODEX trial) or dexmedetomidine versus midazolam (MIDEX trial). Pooled analysis was used to determine whether dexmedetomidine was noninferior at maintaining patients within the target sedation range.12
Patients projected to require mechanical ventilation for more than 24 hours were randomly assigned to a sedative agent within 72 hours of ICU admission. Sedative infusions were titrated to maintain light-to-moderate sedation (RASS, 0 to -3). Dexmedetomidine was found to be noninferior to midazolam and propofol in maintaining this degree of sedation. The study reported that time at target RASS without rescue medication was as follows: midazolam 56.6% versus dexmedetomidine 60.7%, and propofol 64.7% versus dexmedetomidine 64.6%. Drug discontinuation rates were similar in all groups, but discontinuation due to a lack of efficacy was more frequent in the dexmedetomidine group (midazolam 4% versus dexmedetomidine 9%, P =.02 and propofol 5% versus dexmedetomidine 14%, P <.01). One explanation for this may be the unfamiliarity amongst participating clinicians in titrating dexmedetomidine compared with either propofol or midazolam; however, an increased incidence of bradycardia and hypotension was also observed in the dexmedetomidine groups in both studies. Bradycardia was reported in 14.2% of the dexmedetomidine group versus 5.2% of the midazolam group (P < .001). Similar results for the incidence of bradycardia and hypotension were observed in the PRODEX trial. There was also a significant increase in the incidence of first-degree atrioventricular block amongst patients receiving dexmedetomidine (3.7%) versus propofol (0.8%) in the PRODEX trial (P = .04).
The median length of ICU stay was not significantly different in the 2 studies. However, there were conflicting results relating to duration of mechanical ventilation. MIDEX reported that in comparison with midazolam, dexmedetomidine was associated with a statistically significant reduction in the median duration of mechanical ventilation (123 hours [interquartile range [IQR] 67-337 versus 164 hours [IQR 93-380], P=.03). PRODEX reported a reduction in the median duration of mechanical ventilation in the dexmedetomidine group that did not reach statistical significance (97 hours [IQR 45-257] versus 118 hours [IQR 48-327], P = .24; Figure 3). Turunen et al13 conducted an economic evaluation of the MIDEX and PRODEX trials. They evaluated total sedative cost by consumption as well the number of days intubated and the number of critical care days without mechanical ventilation. Pooled results from both studies reported a statistically significant reduction in median duration of critical care stay in the dexmedetomidine group (dexmedetomidine 166.5 hours [IQR 98.5-315] versus standard care 196 hours [IQR 116-361], P = .02). They also reported statistically significant reductions in the dexmedetomidine group for median duration of mechanical ventilation (103 hours [IQR 51-215] versus 139 hours [IQR 70-265], P=.005) and median time to extubation (89 hours [IQR 46-188] versus 118 hours [53-231], P = .00003).
Pooled data from both trials demonstrated that sedation with dexmedetomidine resulted in lower total critical care costs, with a median cost reduction of E2656 as compared with standard regimens using either midazolam or propofol.
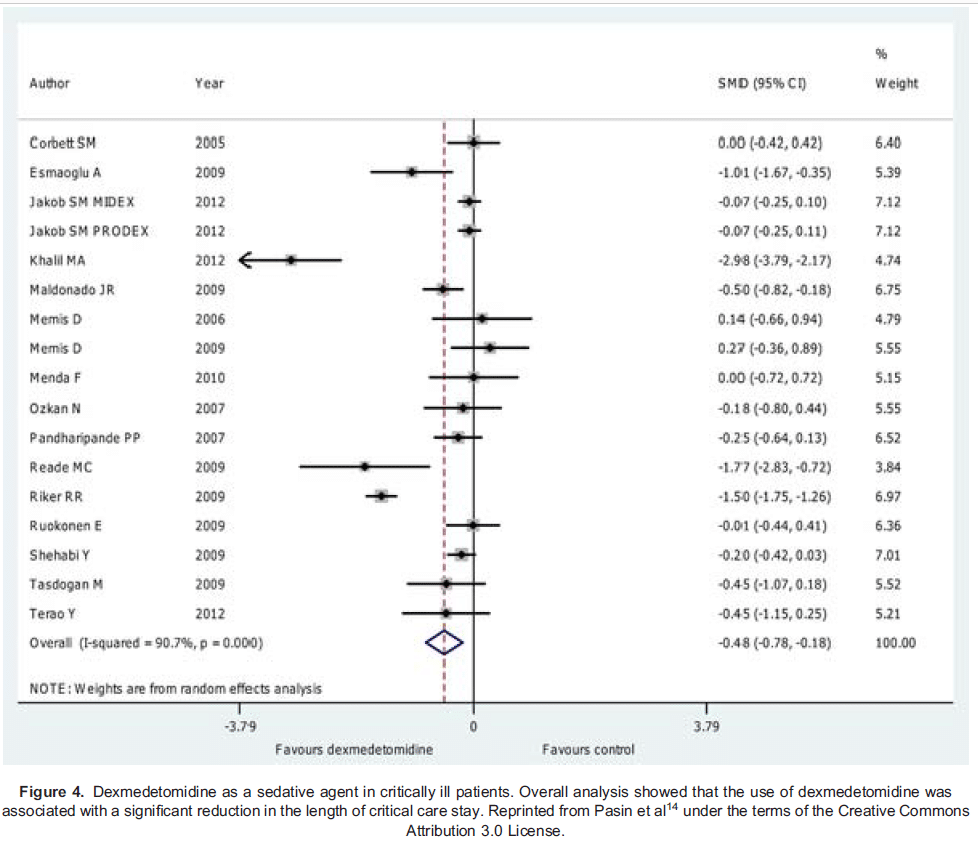
A meta-analysis by Pasin and colleagues14 provided further evidence of the economic and clinical benefits of a dexmedetomidine-based sedative regimen. Their overall analysis was that dexmedetomidine was associated with a significant reduction in both length of critical care stay (illustrated in Figure 4; weighted mean difference -0.79 days [-1.17 to -0.4], P < .001) and time to extubation (weighted mean difference- 2.74 hours [-3.8 to-1.65], P < .001; 21.65 vs 23.8 hours, P=.005).
A pilot, phase 3 multicentre, prospective, randomised, double-blinded, double-dummy active comparator study by Ruokonen et al15 compared dexmedetomidine to propofol or midazolam for long-term sedation on critical care. Their primary aim was to assess whether sedation with dexmedetomidine is as effective as standard regimens with propofol or midazolam in patients admitted within 72 hours and expected to require sedation for >24 hours with a length of stay >48 hours. Outcome measures included time maintained at target sedation level and length of critical care stay.
The results demonstrated a similar length of critical care stay between the groups and a nonsignificant trend toward a shorter median duration of mechanical ventilation in the dexmedetomidine group compared with the standard of care group (77.2 hours [17.5-338.8 hours] vs 110.6 hours [20.1-675 hours], P=.109).15 Overall, there was no statistically significant difference in time spent at target RASS (median time at target RASS 64% dexmedetomidine versus 63% standard care). There was, however, a significant reduction in median time at target RASS in the dexmedetomidine group for those patients with a target RASS of -4 (median time 42% [range 4%-64%] vs median of 62% [range 0%-85%]). The authors concluded that dexmedetomidine is not suitable for patients requiring deep sedation (RASS -4 or less).
A study by Riker et al16 reported similar findings to the study by Jakob et al,12 in which the use of dexmedetomidine was associated with reduced time to extubation compared with midazolam. Riker et al compared the efficacy and safety of prolonged sedation using dexmedetomidine versus midazolam for mechanically ventilated patients. They reported that the median time to extubation was 1.9 days less in dexmedetomidine-treated patients compared with those who received midazolam (3.7 days [95% confidence interval [CI], 3.1 to 4.0] vs 5.6 days [95% CI, 4.6 to 5.9]; P = .01).
Nunes et al17 conducted a retrospective study that explored whether different sedation regimens influenced the course and duration of the weaning process in patients on critical care. This was a noninterventional study conducted in 15 Swedish critical care units. Patients were treated according to the judgment of their attending physician, and the choice of sedation regimen followed normal clinical practice at each centre. A total of 152 intubated adults were enrolled. Having already been assessed as ‘fit for weaning,’ they were divided into 3 groups according to the sedative(s) received prior to their enrolment in the study. The 3 groups were dexmedetomidine alone (DEX group, n = 32), standard of care (SOC) with midazolam and/or propofol (SOC group, n = 67), and SOC plus dexmedetomidine (SOCDEX group, n = 53).
The median durations of intubation of patients in the SOC (37 hours [IQR 24-64]) and SOCDEX (48.5 hours [IQR 30.6-77.8]) groups before the start of the weaning period were significantly shorter than that in the DEX group (79.1 hours [43.4-122.3], P < .001). Despite this, the median time for weaning was significantly shorter for patients in the DEX group (5.4 hours [IQR 1.6- 20.3]) versus both the SOC group (17.8 hours [IQR 5-31.8]; P= .006) and the SOCDEX group (26.3 hours [IQR 16.8-38.1; P < .001). It has been suggested that as there was not a statistically significant difference in median time to weaning between the SOC and SOCDEX groups (P = .213) that the potential benefit of dexmedetomidine with respect to faster weaning from mechanical ventilation may be lost if dexmedetomidine is not used as a single sedative agent. Important limitations of this study include the small number of patients included and its retrospective, nonblinded design.
Use as a Sole Agent
A recent multinational, open-label randomised controlled trial by Shehabi et al18 with almost 4000 subjects examined the utility of dexmedetomidine as a sole, early sedative agent, comparing it with usual care. Study participants were adult patients, ventilated in the ICU for less than 12 hours, anticipated to require ventilation for at least a further calendar day and receiving sedatives. Dexmedetomidine was avoided in the usual care group and used where possible as a primary or sole agent in the intervention group. The primary outcome measure was 90-day all-cause mortality. Secondary outcome measures included number of days free of coma or delirium and number of days free of mechanical ventilation.
The trial reported no difference in 90-day all-cause mortality between the 2 groups (29.1% in both groups). As measured at day 28, the number of days free of coma or delirium and mechanical ventilation were both 1 day higher in the dexmedetomidine group. The authors concluded that despite the fact that patients in the dexmedetomidine group spent a greater proportion of time within target RASS (56.1% vs 51.8%), dexmedetomidine alone is insufficient to provide adequate sedation in this population. A total of 74.5% of patients in the dexmedetomidine group required supplemental sedatives. More adverse events, such as hypotension, bradycardia, and prolonged sinus asystole were also reported in the dexmedetomidine group. The rate for prolonged sinus asystole was 0.7% in the dexmedetomidine group versus 0.1% in the usual care group.
Improvement in Pain Control
Dexmedetomidine is a potent alpha-2 agonist that has effects at various sites in the pain pathway. The main site of action is in the spinal cord, in which stimulation of alpha-2 receptors in the substantia gelatinosa of the dorsal horn reduces the release of nociceptive neurotransmitters. Patients receiving dexmedetomidine have also been observed to have improved oral endotracheal tube tolerance. As a result, patients are more often able to effectively communicate symptoms, such as pain, to the staff looking after them. Jakob et al12 reported a 40% improvement in the ability of patients to communicate pain, allowing better titration of analgesia. Further evidence to support the role of dexmedetomidine as an analgesic comes from its use in anaesthesia and perioperative care. Aho et al19 demonstrated that dexmedetomidine reduced opioid requirements for female patients undergoing laparoscopic tube ligation. Similar results were established by Gurbet et al20 for patients undergoing abdominal surgery.
Reduction in Agitation and Delirium
Delirium is very common amongst patients admitted to critical care. It is associated with prolonged hospital length of stay and time requiring mechanical ventilation, both of which may increase health care expense.21,22
A number of studies have reported reduced delirium in patients receiving dexmedetomidine. Riker et al16 reported a significant reduction in delirium in the dexmedetomidine group versus the midazolam group in a large multicentre, prospective, double-blind, randomised trial. The reported prevalence of delirium was 54% in dexmedetomidine-treated patients versus 76.6% in midazolam-treated patients (95% CI, 14% to 33%; P<.001).16
Maldonado et al23 investigated the effects of postoperative sedation on the development of delirium in patients undergoing cardiac valve procedures. The incidence of delirium for the entire study population was 34%. The incidence of delirium for patients receiving different sedative agents was as follows: dexmedetomidine, 3%; propofol, 50%; and midazolam, 50%. The absolute risk reduction in the incidence of delirium associated with dexmedetomidine was therefore 47%(95%CI, 28%-66%), corresponding to a number needed to treat of just more than 2 patients to prevent 1 patient suffering from delirium (95% CI, 1.5-3.6).23
There are a number of potential explanations to account for these observations. First, unlike propofol and benzodiazepines, dexmedetomidine does not potentiate GABAA receptor activity. Second, dexmedetomidine is thought to provide a more natural sleep/wake pattern.
SUMMARY
Dexmedetomidine is an alternative sedative agent for use in critical care. It has a different mechanism of action compared with other more standard sedation agents. Both patient-specific and organisational benefits have been described in the literature. Most important amongst these are reductions in duration of mechanical ventilation, duration of critical care admission and incidence of delirium, in addition to important analgesic properties. Despite these recognised benefits, dexmedetomidine has not been universally adopted as a first-line sedative agent in critical care, and its effectiveness as a single-agent sedative has been called into question by a recent trial.
REFERENCES
- EMC. Summary of product characteristics. Accessed Aug 1st 2018 https://www.medicines.org.uk/emc/product/4783/smpc
- EU Medicines Agency. Initial marketing authorisation. Accessed Aug 1st 2018 https://www.ema.europa.eu/en/documents/assessment-report/dexdor-epar-public-assessment-report_en.pdf
- EU Medicines Agency. Extension of indication variation assessment report. Accessed Aug 1st 2018. https://www.ema.europa.eu/en/documents/variation-report/dexdor-h-c-2268-ii-0026-epar-assessment-report-variation_en.pdf
- Scott-Warren VL, Sebastian J. Dexmedetomidine: its use in intensive care medicine and anaesthesia. BJA Educ. 2016;16:242-246.
- Tobias J. Dexmedetomidine to control agitation and delirium from toxic ingestions in adolescents. J Pediatr Pharmacol Ther. 2010;15:43-48.
- Scarth E, Smith S. Drugs in Anaesthesia and Intensive Care. 5th ed. Oxford, UK: Oxford University Press; 2016.
- Orion Pharma. Dexdor dosing information. Accessed Aug 1st 2018. https://www.dexdor.eu/contentassets/396cbd4029c54d0fadb0712f1baf1ca9/dexdor_dosing-poster-a4-2017_8mcg-low.pdf
- Kollef MH, Levy NT, Ahrens TS, Schaiff R, Prentice D, Sherman G. The use of continuous i.v. sedation is associated with prolongation of mechanical ventilation. Chest. 1998;114(2):541-548.
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342(20):1471-1477.
- Jones C, Backman C, Capuzzo M, Flaatten H, Rylander C, Griffiths RD. Precipitants of post-traumatic stress disorder following intensive care: a hypothesis generating study of diversity in care. Intensive Care Med. 2007;33(6):978-985.
- Brook AD, Ahrens TS, Schaiff R, et al. Effect of a nursing-implemented sedation protocol on the duration of mechanical ventilation. Crit Care Med. 1999;27(12):2609-2615.
- Jakob SM, Ruokonen E, Grounds RM, et al. Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA. 2012;307(11):1151-1160.
- Turunen H, Jakob SM, Ruokonen E, et al. Dexmedetomidine versus standard care sedation with propofol or midazolam in intensive care: an economic evaluation. Crit Care. 2015;19:67.
- Pasin L, Greco T, Feltracco P, et al. Dexmedetomidine as a sedative agent in critically ill patients: a meta-analysis of randomized controlled trials. PLoS One. 2013;8(12):e82913. https://doi.org/10.1371/journal.pone.0082913
- Ruokonen E, Parviainen I, Jakob SM, et al. Dexmedetomidine versus propofol/midazolam for long-term sedation during mechanical ventilation. Intensive Care Med. 2009;35(2):282-290.
- Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA. 2009;301(5):489-499.
- Nunes SL, Forsberg S, Blomqvist H, et al. Effect of sedation regimen on weaning from mechanical ventilation in the intensive care unit. Clin Drug Investig. 2018;38(6):535-543. doi:10.1007/s40261-018-0636-2
- Shehabi Y, Howe B, Bellomo R, et al. Early sedation with dexmedetomidine in critically ill patients. N Engl J Med. 2019;380:2506-2517.
- Aho MS, Erkola OA, Scheinin H, Lehtinen AM, Korttila KT. Effect of intravenously administered dexmedetomidine on pain after laparoscopic tubal ligation. Anesth Analg. 1991;73(2):112-118.
- Gurbet A, Basagan-Mogol E, Tu¨ rker G, Ugun F, Nur Kaya F, Ozcan B. Intraoperative infusion of dexmedetomidine reduces preoperative analgesic requirements. Can J Anaesth. 2006;53(7):646-652.
- Reade MC, Eastwood GM, Bellomo R, et al. Effect of dexmedetomidine added to standard care on ventilator-free time in patients with agitated delirium: a randomized clinical trial. JAMA. 2016;315(14):1460-1468.
- Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291(14):1753-1762. doi:10.1001/jama.291.14.1753
- Maldonado JR, Wysong A, van der Starre PJ, Block T, Miller C, Reitz BA. Dexmedetomidine and the reduction of postoperative delirium after cardiac surgery. Psychosomatics. 2009;50(3):206-217.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/