Covid-19

KEY POINTS
- Posttraumatic stress symptoms have been reported in health care workers after pandemics, including SARS, MERS and Ebola.
- The extent of the psychological impact of COVID-19 on health care workers is not yet known.
- Stress, resilience and burnout need to be considered and addressed separately when considering wellbeing.
- Identifying those at risk can be difficult in large workforces, so a multimodal approach is most effective.
- A wellbeing task force focusing resources on psychological support and key stressors for staff helps to improve wellbeing and morale.
FOREWORD
Professor Rob Bor, Consultant Clinical Psychologist
There is no health without mental health.
Brock Chisholm1
Understanding and supporting the psychological wellbeing of health care professionals working with COVID-19 patients has become increasingly important and a main focus of resilience and prevention strategies within many health care settings. The emerging published literature, which has studied health care professionals’ psychological wellbeing, points to a number of recurring themes, although researchers are keen to stress that it is not yet possible to report on the long-term psychological effects and whether these worsen or improve over time.
Stress and burnout among health care staff working with these patients is most intense when staff become chronically fatigued, emotionally exhausted, feel depersonalized, experience moral (dis)stress, question the extent of management support for their efforts and feel a low sense of accomplishment for their vital work. There are, however, proven psychological and coaching methods and interventions, as well as informal ‘coffee and chat’ spaces by which staff can improve or protect their mental wellbeing, reduce the risk of burnout or suffering posttraumatic stress, develop resilience, cope better with the tasks confronting them and remain in their job. There are no published data yet on staff attrition following the initial COVID-19 outbreak and associated surge, but anecdotally, it has already added to staff costs as well as the additional costs associated with the loss of clinicians with vast clinical experience. There is a compelling case for placing the emotional wellbeing for staff high on health care managers’ list of priorities, which will inevitably benefit not only COVID-19 patients but also others attending health care settings.
INTRODUCTION
COVID-19, the disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is the defining global health crisis of our time, with more than 106 million cases worldwide as of February 2021.2
In the aftermath of the Severe Acute Respiratory Syndrome (SARS) pandemic in China, 10% of health care workers experienced some form of posttraumatic stress (PTS) symptoms, in some cases lasting between 1 and 3 years.3 A review has shown that PTS symptoms after outbreaks occur in 11% to 74% of health care workers. Depression, insomnia, anxiety and general psychiatric symptoms were all highlighted as being the most prevalent symptoms.4
Experiencing high levels of unfamiliarity and uncontrollability increase the likelihood of developing PTS symptoms, in addition to prolonged exposure of the pandemic itself.5–7 In this now 13-month-long unprecedented COVID-19 pandemic, unfamiliarity and uncontrollability are key emotions. The incidence of PTS symptoms as a result of COVID-19 is yet to be ascertained, but historical data coupled with the scale of the current pandemic suggests that the psychological impact of COVID-19 on our health care workers needs to be battled in parallel with the disease itself.
Before the COVID-19 pandemic, the physical and mental impact of high-stress specialties, such as anaesthesia and intensive care, were already being recognised and addressed.8 It is vital that the psychological burden of the COVID-19 pandemic, occurring on a baseline high prevalence of burnout, depression and stress within these specialties, is understood and that measures are taken to preserve the wellbeing of these health care workers.
In this article, we aim to help departments and organisations identify those at risk, understand the tools that already exist to facilitate improved wellbeing and how to go about setting up a wellbeing response to COVID-19 to help frontline health care workers.
WELLBEING IN ANAESTHESIA AND COVID-19
Wellbeing in anaesthesia has been a topic of increasing interest in recent years. In the United Kingdom in 2017, the Royal College of Anaesthetists’ (RCoA) survey of morale and welfare identified that 85% of anaesthetists in training were at a higher risk of burnout. A national survey in 2018 looking at fatigue in consultants in anaesthesia and paediatric intensive care showed that 91% reported work-related fatigue and more than 50% felt this led to a moderate or significant negative impact on health, wellbeing and home life.9 As a result of these surveys, changes have been made to tackle fatigue and improve mental health within the anaesthetic and intensive care community.
From a 2020 survey regarding the view from the frontline of anaesthesia during COVID-19 noted that 43.9% of workers felt mentally unwell, with more than two-thirds under a high degree of pressure and 13.7% currently at risk of burnout as a direct result of COVID-19 stress. In the same survey, nearly half (45.4%) perceived morale within their team as high or very high.10 This may represent our ability to support each other in a team environment and improved awareness of mental health within departments.
STRESS, BURNOUT AND RESILIENCE
Burnout, stress and resilience are often discussed together when considering wellbeing. Although interlinked, it is important to recognise that they are not the same. To improve wellbeing, each needs to be considered and addressed separately.
Stress
Stress is defined as ‘‘when the pressure placed on an individual exceeds their perceived capacity to cope.’’ Stress can improve the performance of the individual while leading to overengagement and hyperactivity. The negative impacts are that it can result in anxiety disorders and loss of energy with primarily physical damage, although this can also be behavioural and emotional.11
Signs and responses to stress may include the following:
- Insomnia
- Fatigue
- Irritability
- Anxiety
- Depression
- Burnout
- Feelings of guilt
- Anger
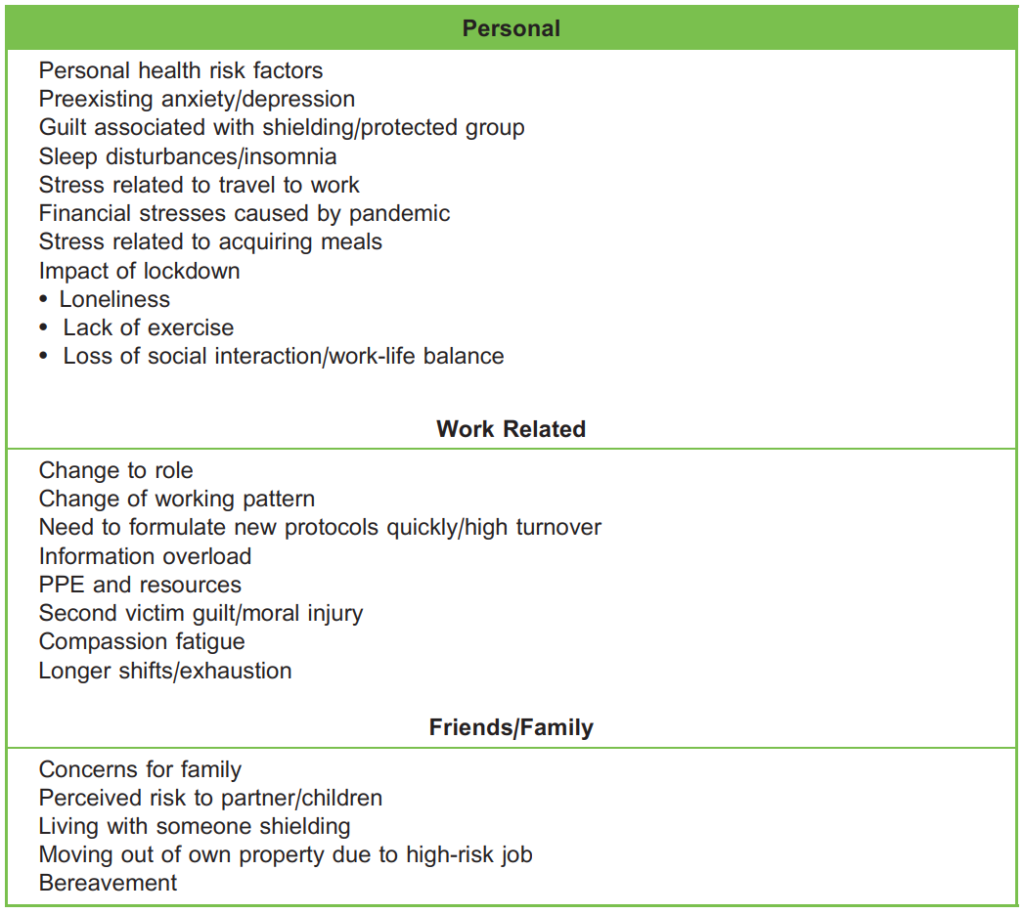
Table 1. Factors Leading to Increased Stress During COVID-19: Personal, Work Related and Family
Burnout
Prolonged periods of stress can lead to burnout.
The World Health Organisation defines burnout as ‘‘a syndrome resulting from chronic workplace stress that has not been successfully managed.’’ Although burnout can present with a collection of physical and psychological signs and symptoms, it is characterised by a triad of (1) emotional exhaustion, (2) depersonalization and (3) a sense of low personal accomplishment.12
The cause of burnout is multifactorial, with both personal and organisational factors contributing. During COVID-19, moral distress resulting from a perceived inability to provide adequate care for patients due to an overwhelmed health care service is an additional contributory factor.
Resilience
Resilience is the capacity to recover from work-related challenges and the ability to adapt well in the face of adversity, trauma, tragedy or significant sources of stress.
Akin to burnout and stress, an individual’s resilience will be shaped by both personal and organisational/environmental factors.12 Resilience is often an inherent trait, but it can also be taught. Improving resilience can be used as a tool to reduce the risk of burnout.
FACTORS LEADING TO INCREASED STRESS
The factors leading to increased stress amongst anaesthetists and intensivists during COVID-19 are shown in Table 1.
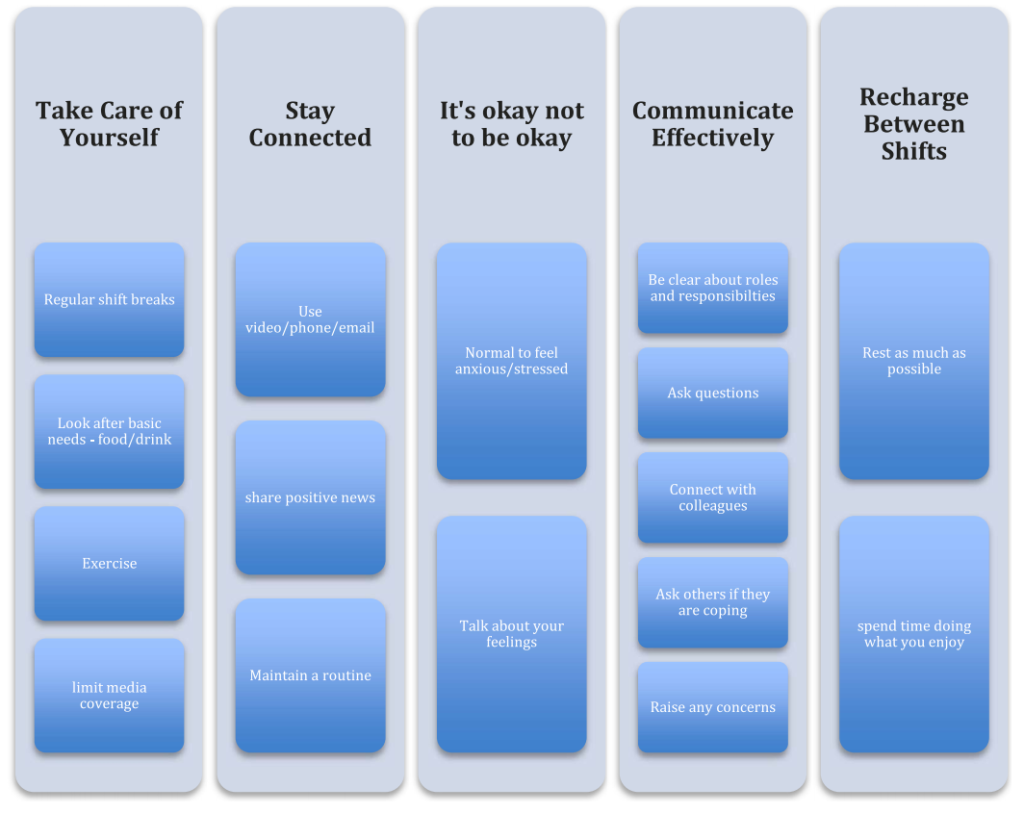
Figure 1. General advice and tools to help cope during the pandemic.
Identifying Staff Who Need Psychological Support
Being able to recognise workforce vulnerability and the anxiety this might trigger can make work more rewarding and promote empathy and compassion.13
Identifying those individuals who need support can be challenging in hospitals with a large workforce, especially in a lowresource setting. Professional wellbeing is multifactorial and fits poorly into current measuring tools14; therefore, an approach using varying tools to broaden the catchment of staff is most effective. These tools include the following:
- Nominated trust wellbeing guardian, in charge of coordinating staff wellbeing
- Departmental wellbeing team with a member dedicated to checking in on staff about whom they are concerned.
- Identify nonclinical staff dedicated to checking in on staff who are off sick and self-isolating with COVID-19.
- Burnout questionnaire (Maslach Burnout Inventory [MBI] is most commonly used)15
- Anonymous help lines (local or national)
Wellbeing self-assessment tools to help staff manage their physical and mental health and identify when they need to seek more support16
- Regular post-shift debrief sessions with in-house psychologists or on-call team following the management of distressing patient cases (e.g., cardiac arrests, deaths, etc.)
- In-house psychological support from local psychologists, counselors and coaches (eg, in our institution, a Resilience and Emotional Support Team [REST] was launched that could be accessed any staff member from 8 AM to 10 PM)
IMPROVING STAFF WELLBEING DURING A PANDEMIC
The development of PTS symptoms by health care workers can be related to individual characteristics, the level of exposure to affected patients and organisational support. Characteristics such as anxiety or insecurity may increase the risk of burnout and PTS symptoms.12 To support the wellbeing of health care workers, the following are recommended:
- Assessment and promotion of coping strategies (Figure 1) and personal resilience
- Provision of adequate protective equipment supplies
- Organisation of support services

Figure 2. Core aspects of wellbeing.
Establishing a COVID-19 wellbeing team is vital for coordinating the above recommendations. The team should identify the potential core aspects of wellbeing during this crisis and implement strategies to support their staff (Figure 2). Improving resilience, reducing stress and avoiding burnout are core objectives. In addition to psychological support and basic personal requirements such as food and rest, areas of potential stress for staff should be identified and targeted in greater detail. Examples of areas for potential stress include the inability to park at work because of restrictions, yet staff are met with a need to avoid public transport; new unfamiliar standard operating practices and guidelines relating to COVID-19; and childcare issues.
The Intensive Care Society UK has developed an outline regarding how to approach the wellbeing of staff in the ICU depending on the COVID caseload (Table 2),17 a readily available resource that can be adapted and applied to both anaesthetic and medical workforces.
The section below outlines the resources and changes that have been implemented in some areas of the United Kingdom to support staff, including national-, organisational- and individual-level changes (Tables 3–5). These can be adapted and applied to varied resource settings.
National Changes
National-level changes to support frontline worker wellbeing in the United Kingdom has being varied and helped to boost morale (Table 3). During the initial surge of COVID-19 cases in early 2020, the two main issues causing severe anxiety and stress were the availability of personal protective equipment (PPE), especially for those performing aerosol-generating procedures, and the difficulty accessing groceries because of long working hours and low supplies in supermarkets. These were addressed at a national level by ensuring PPE supplies were not an issue for further surges and that all hospital workers had protected supermarket access times.
Organisational/Departmental Changes
The changes that occurred at the organisational and departmental level in the United Kingdom to support staff were the most significant (Table 4). In a number of trusts, wellbeing teams were created or expanded to ensure that all key areas of wellbeing were being addressed and that there were significant rest facilities and supplies of food. However, the biggest impact for staff struggling with their wellbeing was the availability of psychological support services. Most hospitals offered in-house psychological support, and others also teamed up with professional coaches to create programs such as Coaching Through Covid and Compassion at Work programs, which were available at our institution. These programs were pro bono and offered interested members of staff both one-to-one and group sessions with professional coaches to support them through the pandemic.
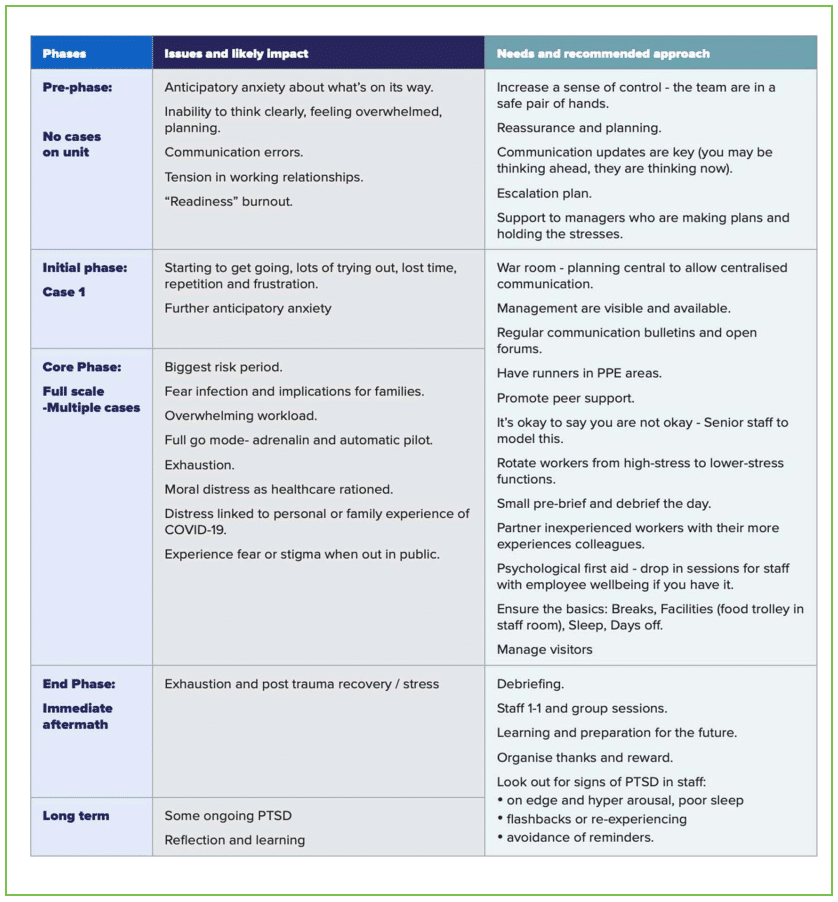
Table 2. Intensive Care Society: How to Approach Wellbeing for Staff in Intensive Care. Approval to use image granted by the Intensive Care Society17
Individual Changes
General advice and resources on mindfulness and resilience can help individuals to focus on their wellbeing (Figure 1; Table 5). Resources were made available to staff, and digital applications focusing of mindfulness and resilience, such as headspace, also offered free access for National Health Service workers.
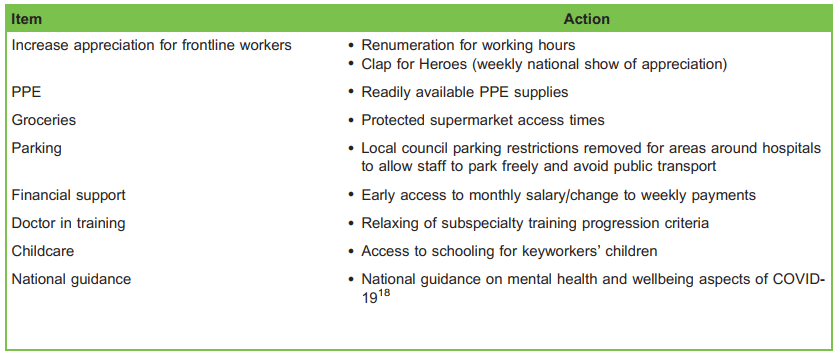
Table 3. National Changes Made in the United Kingdom to Support Staff Wellbeing
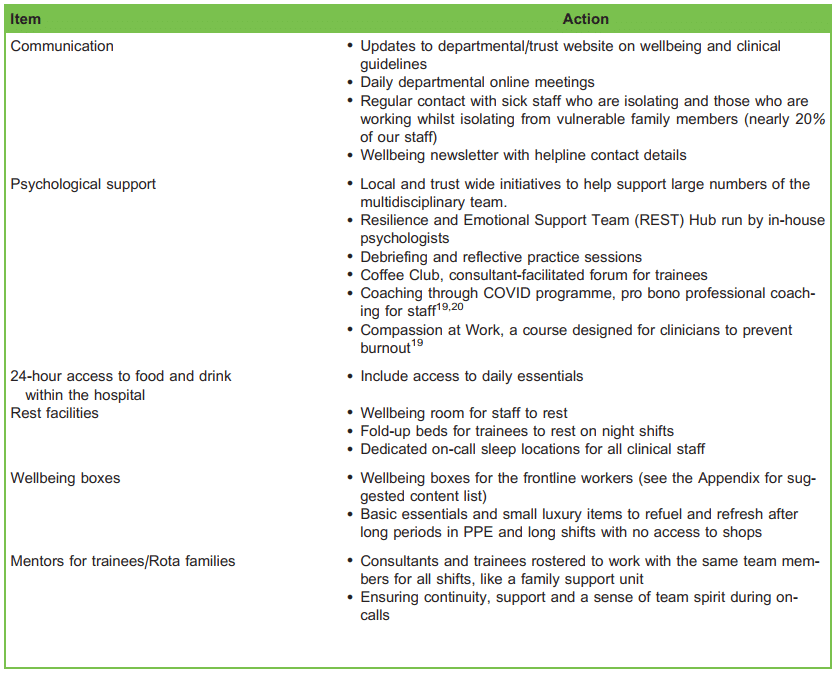
Table 4. Organisational-/Departmental-Level Changes Made in the United Kingdom to Support Staff Wellbeing
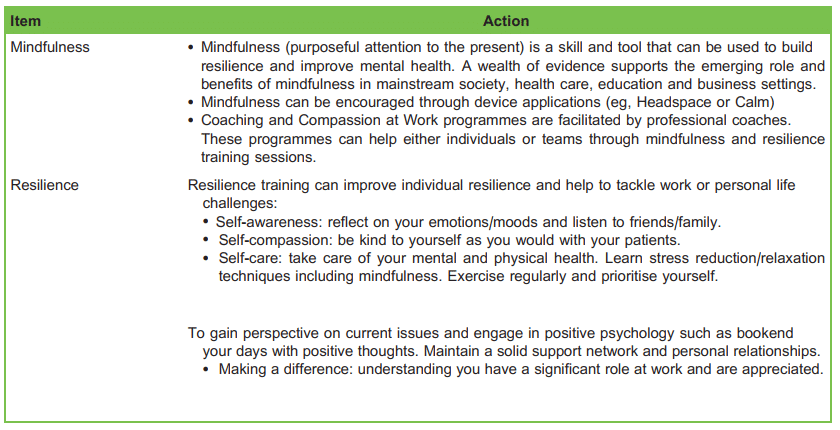
Table 5. Individual Changes Recommended to Staff in the United Kingdom to Support Their Wellbeing
SUMMARY
COVID-19 has drawn a line in the sand, not only for health care workers but for the population worldwide. What came before is no longer, and we must now face a new normal, in which struggles with stress, anxiety, burnout and psychological distress in our colleagues must be tackled to preserve the wellbeing of our workforce fighting this disease.
REFERENCES
1. Outline for a Study Group on World Health and the Survival of the Human Race. Material Drawn From Articles and Speeches by Brock Chisholm. Geneva, Switzerland: World Health Organization; 1954.
2. World Health Organisation. Timeline of WHO’s response to COVID-19. https://covid19.who.int. Accessed 28 July 2020.
3. Wu P, Fang Y, Guan Z, et al. The psychological impact of the SARS epidemic on hospital employees in China: exposure, risk perception, and altruistic acceptance of risk. Can J Psychiatry. 2009;54(5):302-311.
4. Preti E, Di Mattei V, Perego G, et al. The psychological impact of epidemic and pandemic outbreaks on healthcare workers: rapid review of the evidence. Curr Psychiatry Rep. 2020;22(8):43.
5. Marshall RD, Bryant R, Amsel L, et al. The psychology of ongoing threat: relative risk appraisal, September 11, 2001, attacks and terrorism-related fears. Am Psychol. 2007;62(4):304-316.
6. Slovic P. Perception of risk. Science. 1987;236:280-285.
7. Marshall RD, Galea S, Kilpatrick D. Psychological reactions to terrorist attacks. Findings from the National Study of Americans’ reactions to September 11: comment. JAMA. 2002;288(21):2683-2684.
8. Looseley A, Wainwright E, Cook T, et al. Stress, burnout, depression and work satisfaction among UK anaesthetic trainees; a quantitative analysis of the Satisfaction and Wellbeing in Anaesthetic Training study. Anaesthesia. 2019;74:1231-1239.
9. Royal College of Anaesthetists. A report on the welfare, morale and experiences of anaesthetists in training: the need to listen. https://www.rcoa.ac.uk/sites/default/files/documents/2019-08/Welfare-Morale2017.pdf. Accessed 28 July 2020.
10. Royal College of Anaesthetists. View from the frontline of anaesthesia during COVID-19. https://rcoa.ac.uk/sites/default/ files/documents/2020-04/View-from-the-frontline-anaesthesia-during-COVID-19.pdf. Accessed28 July 2020.
11. NHS Employers. Stress management. https://www.nhsemployers.org/~/media/Employers/Publications/Stress%20management.pdf. Accessed 29 July 2020.
12. Wong AV-K, Olusanya O. Burnout and resilience in anaesthesia and intensive care medicine. BJA Educ. 2017;17(10):334-340
13. NHS, National Workforce Skills Development Unit. Workforce stress and the supportive organisation: A framework for improvement through reflection, curiosity and change. https://www.hee.nhs.uk/sites/default/files/documents/Workforce%20Stress%20and%20the%20Supportive%20Organisation_0.pdf. Accessed 29 July 2020.
14. World Federation of Societies of Anaesthesiologists. Anaesthesiologists’ professional health and well-being. https://resources.wfsahq.org/atotw/anaesthesiologists-professional-health-and-well-being/. Accessed 4 February 2021.
15. Maslach C, Jackson S, Leiter MP, eds. Maslach Burnout Inventory Manual. 3rd ed. Palo Alto, CA: ConsultingPsychologists Press; 1996.
16. https://www.exeter.ac.uk/staff/wellbeing/self-care/ Accessed 4 February 2021.
17. Intensive Care Society. Wellbeing hub. https://ics.ac.uk/ICS/ICS/Wellbeing.aspx. Accessed 28 July 2020.
18. Public Health England. Guidance for the public on the mental health and wellbeing aspects of coronavirus (COVID-19). https://www.gov.uk/government/publications/covid-19-guidance-for-the-public-on-mental-health-and-wellbeing/guidancefor-the-public-on-the-mental-health-and-wellbeing-aspects-of-coronavirus-covid-19. Accessed 30 January 2021.
19. Royal College of Anaesthetists. https://rcoa.ac.uk/sites/default/files/documents/2020-08/Bulletin123.pdf. Accessed 1 September 2020.
20. https://coachingthroughcovid.org. Accessed 26th February 2021.
21. https://www.headspace.com. Accessed 26th February 2021.
22. https://www.calm.com. Accessed 26th February 2021.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/