Obstetrics Anaesthesia

QUESTIONS
Before continuing, try to answer the following questions. The answers and a short explanation can be found at the end of the article.
- Regarding the causes of maternal death, the following statements are true:
- Thromboembolism is the most common direct cause of maternal death in the UK.
- Haemorrhage, obstructed labour, sepsis, eclampsia, illegal abortion account for the majority of maternal deaths in the UK.
- The UK maternal mortality rate is 13.95 per 100,000 maternities.
- Causes of maternal death in the UK are similar to those in the rest of the world.
- Regarding maternal deaths in the most recent CEMACH report, the following statements are true:
- Obesity was uncommon in those women whose deaths were directly related to anaesthesia.
- The third most common cause of death was directly as a result of anaesthesia.
- Senior anaesthetic staff should be involved early in the care of sick women.
- Consultants should be involved in the treatment of women with a BMI > 45.
- The following statements are either true or false.
- Epidural analgesia during labour is not recommended in women with raised BMI
- Obesity is a serious and increasing problem
- Obese women should be reviewed early in labour by an anaesthetist
- The incidences of cardiovascular disease and obesity are decreasing in the UK
- The following statements are either true or false.
- Maternal mortality is decreasing in the UK
- Intralipid should not be used for the treatment of severe local anaesthetic toxicity in the obstetric population
- Syntocinon should be given as a 10u bolus.
- Maternal tachycardia is not a useful sign as it is usually due to anxiety
WHAT IS CEMACH?
The Confidential Enquiry into Maternal and Child Health (CEMACH) identifies deaths of women in the UK during pregnancy and within 42 days of giving birth that are directly or indirectly related to the pregnancy. The circumstances surrounding these deaths are then examined and guidance provided to help improve the care of women presenting with similar conditions in the future. The report considers deaths over a three-year period and the most recent report, ‘Saving Mothers’ Lives’, examined the period 2003-5. Prior to CEMACH, the ‘Confidential Enquiry into Maternal Deaths’ (CEMD) reported triennially on deaths in pregnancy or following delivery in England and Wales and provided 54 years of valuable continuous data in this area.
The current report identifies 295 deaths, with 132 directly and 163 indirectly related to pregnancy. For the population examined, this represents a maternal mortality rate of 13.95 per 100,000 maternities. This is an increase from the previous report, but is not statistically significant. Six women died as a direct result of anaesthesia and poor perioperative anaesthetic management was considered to have contributed to the fatal outcome in a further 31cases.
WHY DO MOTHERS DIE?
Most deaths worldwide occur due to haemorrhage, obstructed labour, infection, eclampsia and complications of abortion. In the UK, these problems combined accounted for only 14% of deaths.
CAUSES OF MATERNAL DEATH IN THE UK
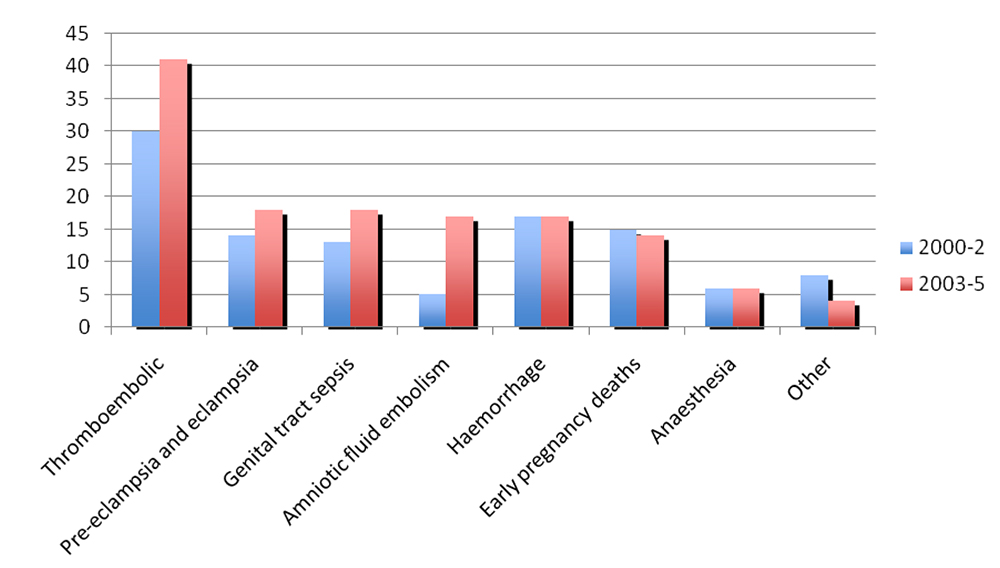
Figure 1. Direct causes of maternal death
1. Thromboembolic – 41 deaths
- 33 deaths due to pulmonary embolism, 8 due to cerebral vein thrombosis.
- Incidence largely unchanged since 1990s when thromboprophlaxis became routine.
- 27 of the women who died had risk factors for thromboembolism.
- Treatment was considered substandard in the majority of cases of pulmonary embolism (22 of the 33). The main reasons were inadequate risk assessment, failure to recognise symptoms or act on risk factors and failure to commence appropriate treatment.
- Incidence may increase in the future as a result of the increasing rate of obesity.
2. Pre-eclampsia and eclampsia – 18 deaths
- 6 women had eclampsia and eight developed HELLP syndrome (Haemolysis, Elevated Liver enzymes, Low Platelets).
- Intracranial haemorrhage was the most common cause of death.
- In 8 cases there was major substandard care of which failure to commence effective anti-hypertensive therapy was the most recurring theme.
3. Genital tract sepsis – 18 deaths
- Similar to previous years.
- The most common organisms responsible for sepsis were Group A β-haemolytic Strep and E.Coli.
- In some cases there were delays in diagnosis, failure to recognise severity of illness, delays in admission and commencing appropriate treatment and late involvement of senior staff.
4. Amniotic fluid embolism – 17 deaths
- Significant increase compared to previous years.
- In 7 cases, care was deemed substandard. Reasons for this included failure to recognise serious illness and delays in resuscitation.
5. Haemorrhage – 17 deaths
- Similar to previous years.
- 10 women received substandard care including poor management of a morbidly adherent placenta and failure to recognise intra-abdominal haemorrhage.
- 2 women refused blood transfusion for religious reasons.
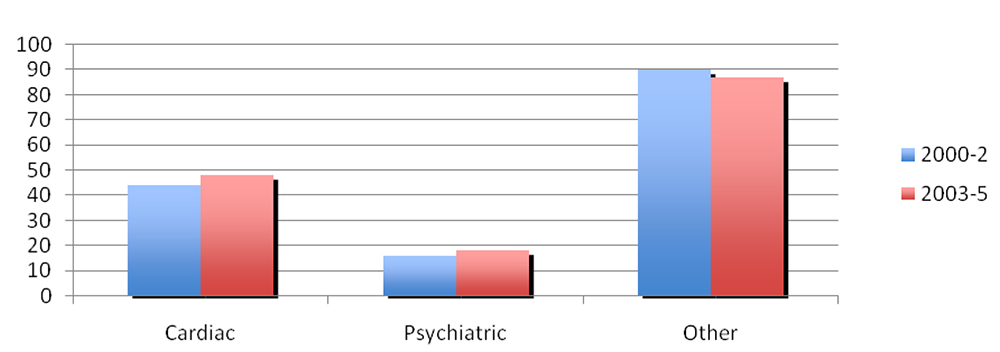
Figure 2. Indirect Causes
1. Cardiac disease – 48 deaths
- This is increasing and may reflect a greater incidence of ischaemic heart disease due to obesity, smoking, increased maternal age, alcohol and poor overall health.
- The main causes of death were myocardial infarction and thoracic aortic dissection.
- Almost half of the women who died received substandard care including inadequate assessment/monitoring throughout pregnancy and a failure to recognise the signs of cardiac disease and initiate appropriate treatment.
2. Psychiatric – 18 deaths
- 12 committed suicide and 6 died from drug overdose.
- The majority of mental health problems encountered are depressive in nature. The risk of developing a serious mental illness is reduced during pregnancy, but markedly elevated in the first three months following childbirth.
- It is important to identify women with psychiatric disease or pre-existing substance misuse so that appropriate management can be planned.
- Substance misuse presents a number of problems for the anaesthetist including difficult IV access and problems providing effective analgesia.
3. Other – 87 deaths
- This category includes deaths due to pre-existing conditions or those that develop and are exacerbated by pregnancy and includes deaths due to cerebral haemorrhage, epilepsy and diabetes.
Women that died were more likely to have experienced social deprivation with mortality rates up to 7 times higher in certain groups including the unemployed or migrants. A third of children who lost their mother were already in care at the time of the maternal death. Obesity was also an important factor. The majority of women who died from thromboembolic disease, sepsis and cardiac disease were overweight or obese.
WHY IS MORTALITY NOT DECREASING?
A number of factors may be responsible:
- Increasing maternal age
- Increasing migrant population
- Obesity
- Cardiovascular disease
- Smoking
- Poor overall health
The final 4 factors were common in many maternal deaths.
DEATHS DIRECTLY RELATED TO ANAESTHESIA
Of the 6 women that died, 4 were obese (2 morbidly obese (BMI > 35)) and the mean age was 30. Two of the women died in early pregnancy.
Postoperative respiratory failure – 3 deaths
- One woman died following laparoscopic surgery for ectopic pregnancy. She was asthmatic and obese. She developed severe bronchospasm following extubation. A trainee anaesthetist failed to re-intubate her trachea and by the time senior help arrived she had suffered a cardiac arrest.
- A second woman who died was also obese and anaesthetised in early pregnancy by a trainee anaesthetist. She was given a relatively large dose of fentanyl prior to transfer to recovery at the end of a procedure. She developed respiratory failure in recovery and suffered a fatal cardiac arrest.
- A third woman who was morbidly obese had an elective caesarean section under spinal anaesthetic performed by a consultant anaesthetist. She became agitated and short of breath postoperatively and a few hours later was transferred to the postnatal ward where her symptoms continued. She was reviewed by an anaesthetist, but had a cardiac arrest some time later. During resuscitation there were problems with availability of equipment.
Drug administration error – 1 death
A woman received an epidural and low dose infusion of local anaesthetic for labour. Following instrumental delivery, syntocinon and IV fluids were administered due to post-partum bleeding. Shortly afterward she suffered a seizure and fatal VF arrest and it became apparent that 150 ml of 0.1% bupivacaine solution had been given intravenously in error.
Anatomical abnormality – 1 death
One woman died following the insertion of a central line. She had pectus excavatum and presented in mid pregnancy with pre-eclampsia and HELLP syndrome. Invasive monitoring was inserted prior to an urgent caesarean section. She suffered a fatal cardiac arrest and at post mortem was found to have a right-sided haemothorax secondary to trauma caused by attempts to insert a central line.
Miscellaneous – 1 death
The final death that was directly attributed to anaesthesia occurred in a woman with multiple medical problems and obesity who was admitted a few weeks following delivery for drainage of a renal collection. She did not want the procedure performed under local anaesthetic. During the general anaesthetic she had a cardiac arrest and died. It was thought her death was due to electrolyte disturbances.
DEATHS TO WHICH POOR ANAESTHETIC MANAGEMENT CONTRIBUTED
Poor anaesthetic management was thought to have contributed to 31 deaths. There were a number of areas into which these deaths can be grouped:
Failure to recognise serious illness.
- Often compounded by rarity of presentation and interpretation of normal/abnormal physiological changes during pregnancy/childbirth. The report highlighted the importance of modified early warning scoring systems (MEWS). An early warning score (EWS) is used in most hospitals in the UK. Points are given for abnormal BP, pulse rate, respiratory rate and oxygen saturation. The points are added together and used to help identify sick patients. Modified early warning scores are being introduced into maternity units and take into account the normal physiological changes of pregnancy.
- A maternal death where failure to recognise serious illness, is illustrated by the following case: A woman who had undergone a medical termination developed an infection due to retained products of conception. She continued to bleed, but delayed seeking medical attention. Shortly after she presented to the hospital she deteriorated due to severe anaemia and sepsis. She was given a large volume of intravenous fluids by trainee medical staff and developed pulmonary oedema. It was felt that earlier recognition of the seriousness of her condition along with careful resuscitation with appropriate blood products and fluids guided by invasive monitoring and inotropes should have been implemented.
Poor management of Haemorrhage including:
- Poor recognition of concealed bleeding.
- Misinterpretation of clinical signs and mistrust of non-invasive blood pressure readings.
- Inconsistent use of invasive monitoring.
- Use of large volumes of cold fluids/blood products.
- Poor post-operative care/observation.
- Poor management of placenta accreta.
Inappropriate use of uterotonics to prevent and manage maternal haemorrhage.
Established guidelines were not always followed. A slow bolus of 5 units syntocinon rather than 10 units should be administered. A rapid bolus of 10 units syntocinon has been associated with cardiovascular collapse and death. A low dose infusion of syntocinon with subsequent IM/IV ergometrine or IM carboprost should be administered to help maintain uterine tone while limiting haemodynamic instability.
Sepsis
The lack of appreciation and management of sepsis was considered to have contributed to the deaths of 15 of the 21 women who died of sepsis related problems.
Pre-eclampsia and eclampsia.
Of the 18 women who died as a result of pre-eclampsia or eclampsia, inadequate anaesthetic management was considered to have contributed to the deaths of four. Problems identified related to poor control of hypertension during and after caesarean section.
Obesity.
The incidence of obesity is increasing and is likely to become more of a problem in future years. Obesity increases the risk of cardiac disease, pre-eclampsia, gestational diabetes, thromboembolism, infection and post-partum haemorrhage. Obesity also makes monitoring and practical procedures more difficult to perform.
The quality of in-house serious incident reporting.
This is vital in helping to reduce maternal deaths. When an untoward incident occurs, a review should be undertaken. A panel of clinicians that is not directly involved in the incident should carry out the review. The panel should investigate the incident so that lessons can be learnt in order to prevent such events occurring in the future. The report highlighted a number of cases where a review was not carried out properly or not carried out at all.
LESSONS FOR THE ANAESTHETIST
Service provision.
- Hospitals should strive for the highest standards of anaesthetic care for pregnant women before, during and after delivery.
- There should be access to senior (consultant) anaesthetic assistance at all times.
General measures.
- Local guidelines are a useful way of improving the care of women with high-risk pregnancies and the effective management of obstetric emergencies.
- Appropriate prevention of thromboembolic disease. Thromboembolic disease accounts for the second most common cause of death in pregnant women. With increasing levels of obesity in some parts of the world, it is likely to become more of a problem in the future.
- Multidisciplinary approach to high-risk patients. For example, obese women can be counselled regarding weight loss prior to becoming pregnant. Once pregnant they should be seen by a dietician to try and reduce weight gain. Morbidly obese women should also be reviewed by an anaesthetist during pregnancy so that potential problems can be identified and appropriate management plans made and discussed.
- Recognition of the implications of substance misuse. Smoking and ischaemic heart/respiratory disease; alcohol and liver disease; intravenous drug use and difficult venous access, risk of endocarditis and challenging post operative analgesia.
- Recognition of the increased incidence of rheumatic heart disease due to the increasing migrant population in certain parts of the world.
Recognition and management of the sick mother.
- It is essential to recognise important clinical signs, including maternal tachycardia to aid early recognition of serious illness. The normal physiological changes of pregnancy may be misinterpreted when managing sick pregnant women. During late pregnancy and labour, cardiac output is increased and a woman may be seriously ill before she becomes hypotensive. At this point she will have little physiological reserve and may deteriorate rapidly if action is not taken.
- Use of modified early warning scores. (See above)
- Seeking senior help early and the training of medical staff in identifying and treating sick mothers. Delays in recognising, treating and calling for senior help in the management of sick women are a recurring theme throughout previous reports. Training staff to deal with emergencies on the delivery suite should be regularly practised through simulation of emergencies with either actors or high fidelity simulators.
- Availability of devices to measure haemoglobin at the point of care. This will provide a rapid result and guide transfusion. Modern equipment is accurate, easy to use and portable.
- Warming of large volume IV infusions. Obstetric blood loss can be rapid and life threatening. Large volumes of cold fluids can lead to hypothermia with the associated problems of coagulopathy and increased blood loss, increased wound infection, myocardial ischaemia/arrhythmias and prolonged action of neuromuscular blocking agents. It is also unpleasant and can lead to slower recovery and increased duration of hospital stay.
- Use of invasive monitoring where appropriate. Invasive arterial blood pressure monitoring may be especially beneficial in certain cases including management of severe pre-eclampsia. Central Venous Pressure monitoring however is not without risk (see above: ‘deaths directly attributed to anaesthesia’) and may confer limited clinical benefit.
- Importance of reducing hypertensive response to laryngoscopy and avoiding syntometrine and ergometrine in severe pre-eclampsia. Laryngoscopy can lead to a dangerous rise in the blood pressure of hypertensive women. This can be reduced by the use of a short acting opioid (e.g. alfentanyl 1-2mg IV) or a beta blocker (e.g. labetalol 10-20mg IV). If opioids are given prior to delivery then the paediatrician should be informed of the risk of neonatal respiratory depression.
- High-risk cases should be managed by consultant anaesthetist/obstetrician in appropriate setting such as high dependency/intensive care.
- Guidelines for the treatment of women who refuse blood transfusion. Groups such as Jehovah’s witnesses may refuse blood and blood product transfusion. Some groups will accept autologous blood transfusion. Autologous blood can be safely ‘salvaged’ intraoperatively, however equipment to do this is expensive.
Prevention of and treatment of local anaesthetic toxicity.
- Inadvertent intravenous administration of local anaesthetic intended for epidural use is potentially fatal (see above: ‘deaths directly attributed to anaesthesia’). Unfortunately it is easy to connect local anaesthetic infusions to intravenous lines as the connectors are the same. Risk can be limited by ensuring equipment (syringes and infusion lines) for administering epidural local anaesthetic solutions are coloured differently to equipment for intravenous infusion.
- Availability of intralipid to treat cardiovascular collapse due to local anaesthetic toxicity. 20% Intralipid may be effective in the management of cardiac arrest following local anaesthetic toxicity. Treatment consists of 1.5 ml/kg as an initial bolus, followed by an infusion of 0.25 ml/kg/min. For further information see www.lipidrescue.squarespace.com
Obesity.
Obesity causes multiple problems for the anaesthetist. Obese women are more likely to need obstetric interventions which will often require some form of anaesthesia. Other problems include:
- Obese women are more at risk of gestational diabetes and hypertension/pre-eclampsia
- Airway and breathing- intubation may be more difficult and the incidence of failed intubationis higher in the obese than non-obese population. Obese patients are more difficult to ventilate and are more prone to oxygen desaturation.
- Circulation- venous access is more difficult, blood pressure monitoring is more difficult and they are more prone to venous thromboembolism.
- Anaesthesia- regional anaesthesia is more difficult and more likely to fail. General anaesthesia is more challenging in the obese patient.
- Special equipment may be required- know the weight limit of your beds/operating tables.
The following simple points should be considered:
- Local protocols for management of obese women. Referral for anaesthetic review prior to labour.
- Regional anaesthesia where possible.
- Consultant led management.
- Availability of lifting assists/appropriate manpower.
- Consideration of invasive arterial blood pressure monitoring.
- All morbidly obese women to receive LMW heparins/TED stockings.
- Early administration of antacid prophylaxis in labour.
ANSWERS TO QUESTIONS
-
- T
- F
- T
- F
The maternal mortality rate in the UK is 13.95 per 100,000 maternities. Thromboembolism is the most common direct cause of death in the UK. However worldwide, haemorrhage, obstructed labour, sepsis, eclampsia and illegal abortion account for the majority of maternal deaths.
-
- F
- F
- T
- T
Of the women whose deaths were directly related toanaesthesia, 4 were obese. In the UK, anaesthesia is the 6th most common direct cause of death. Senior anaesthetists should be involved early in the care of sick women and in those women whose BMI is greater than 35.
-
- F
- T
- T
- F
Obesity and cardiovascular disease are serious and increasing problems. Obese women should be reviewed early in labour and regional anaesthesia encouraged.
-
- F
- F
- F
- F
Maternal mortality is not decreasing in the developed world. Intralipid is not contraindicated in the obstetric population. Syntocinon should be given as a slow bolus of 5 units to limit haemodynamic disturbance. Maternal tachycardia is a cause for concern and should be investigated.
WEBLINKS
- The CEMACH report can be downloaded from www.cemach.org.uk/
- Further information on the use of intralipid for treatment of local anaesthetic toxicity is available at http://lipidrescue.squarespace.com
REFERENCES
- Lewis, G (ed) 2007. The Confidential Enquiry into Maternal and Child Health (CEMACH). Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer – 2003-2005. The Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London: CEMACH.
- Cooper, G. and McClure, J. Anaesthesia chapter from Saving Mothers’ Lives; reviewing maternal deaths to make pregnancy safer: BJA 2008; 100: 17-22.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/