Obstetrics Anaesthesia

KEY POINTS
- Myopathies are muscular disorders with multisystem involvement that have the potential to affect the anaesthetic and obstetric care of pregnant patients.
- Myopathies are associated with increased obstetric complications.
- A multidisciplinary team approach and a comprehensive care plan for delivery are important to ensure safe anaesthetic, obstetric and neonatal care.
INTRODUCTION
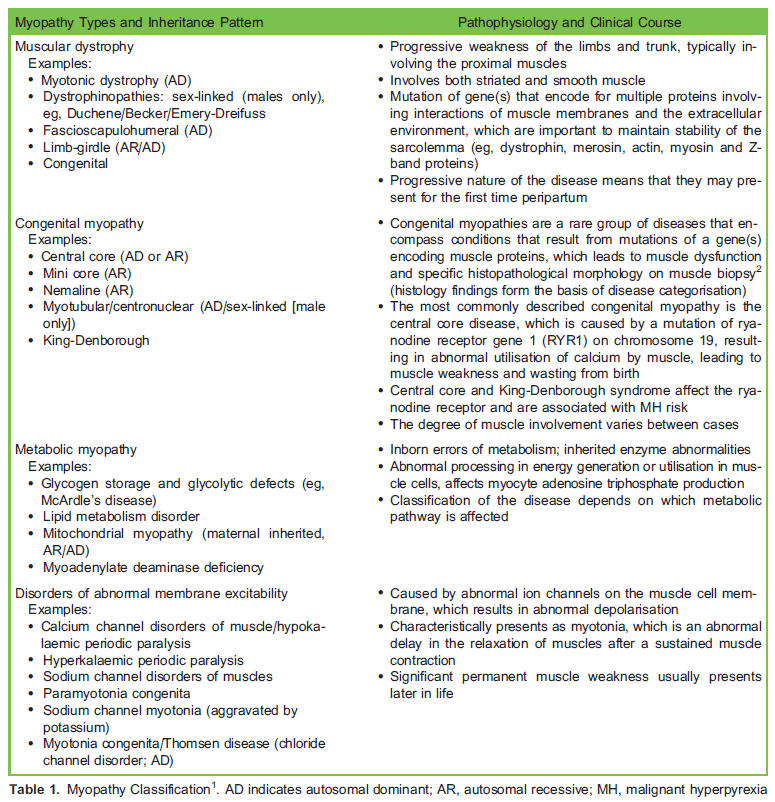
Myopathy refers to disorders caused by abnormal skeletal muscle function with intact nervous innervation. Abnormalities of muscle structure and cellular metabolism result in a variety of clinical syndromes with differing degrees of weakness and dysfunction (Table 1)1. Myopathies can be inherited in an autosomal dominant or recessive manner. There is a spectrum of presentation, from asymptomatic to progressive disease involving multiple organ systems that poses significant challenges to anaesthesia and obstetric care. Symptoms can be exacerbated by the normal physiological changes of
pregnancy.
MYOPATHY
Features of Myopathy During Pregnancy
Subclinical Myopathy
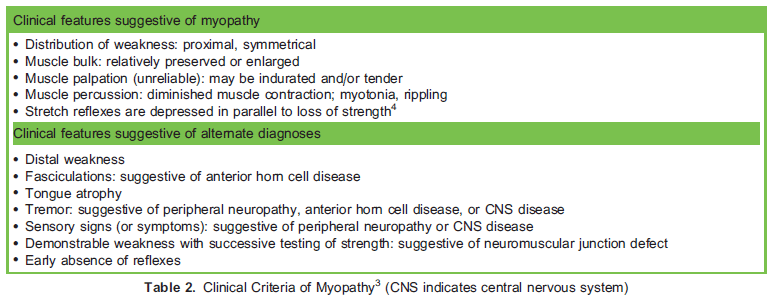
Myopathies consist of a spectrum of muscular diseases; symptoms can be subclinical depending on the genetic defect and mode of inheritance, or they can be clinically evident (Table 2). A history of recurrent pneumonia, previous intensive care admissions following minor illnesses or abnormal muscle weakness or tone should raise concern and warrant appropriate investigation, review and counselling before pregnancy. Maternal diagnosis of neuromuscular disease may occur retrospectively following delivery of a neonate with signs of myopathy. Unexplained elevation of creatinine kinase greater than 4-fold is suggestive of myopathy.
Increased Incidence of Obstetric Complications
Myopathy can result in global muscular dysfunction (striated and smooth muscle), which is further complicated by abnormal cellular pathways in energy generation and utilisation in muscle cells, and can lead to an increased incidence of obstetric complications5, including the following:
- Spontaneous abortion
- Polyhydramnios
- Premature labour and preterm delivery
- Abnormal presentation
- Prolonged first stage of labour
- Uterine atony
- Retained placenta
- Placenta accreta and previa
- Increased incidence of neonatal death
Exacerbation of Myotonia and Muscle Weakness During Pregnancy
Elevated progesterone levels during the third trimester may cause temporary exacerbation of muscle weakness. The mechanism of this is unclear, but it may be caused by effects of progesterone on the intracellular/extracellular potassium ratio6. Progesterone levels fall, and weakness usually improves rapidly following delivery. Regular monitoring of maternal oxygen saturation and respiratory strength is mandatory postpartum for all patients with significant myopathy.
Systemic and Anaesthetic Complications of Myopathies
Myopathies can have multisystem involvement, which has an impact on anaesthetic and obstetric care. Below are general considerations, and there may be specific considerations associated with that specific myopathy that require review.
Airway
- Associated dysmorphia
- Temporomandibular joint dislocation
- Oropharyngeal muscle involvement
- Central sleep apnoea
Anaesthetic considerations
- Careful positioning and preparation for a potentially difficult airway (difficult bag mask ventilation, intubation and pulmonary aspiration)
- Postoperative monitoring for exacerbation of sleep apnoea
Respiratory
- Functional diaphragmatic and intercostal muscle weakness
- Reduced vital capacity (VC), total lung capacity (TLC) and peak expiratory pressure
- VC of ,1 L is predictive of increased morbidity during pregnancy
- Recurrent aspiration pneumonia may lead to chronic lung disease
- Reduced sensitivity to pCO2 in the respiratory centre for those who are chronically hypoxic
Anaesthetic Considerations
- Suxamethonium should be avoided as it may cause unpredictable release of potassium from muscles, leading to potentially life-threatening hyperkalaemia.
- Suxamethonium can induce masseter spasm and/or generalised muscle rigidity, making intubation and ventilation more difficult.
- Nondepolarising muscle relaxants produce longer-lasting paralysis with normal doses in patients with myopathy; a reduced dose should be administered with neuromuscular blockade monitoring.
- Rocuronium and vecuronium have potential advantages for muscle relaxation, as they can be readily reversed with sugammadex.
- Consider the use of high-flow nasal oxygen therapy (HFNOT) via a transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) device for preoxygenation7 (postoperative use of HFNOT can reduce postextubation respiratory failure, but there are no data specific to its use in myopathic patients).
- Magnesium sulphate (eg, for preeclampsia or neonatal neuroprotection) exacerbates muscle weakness and should be used cautiously in myopathic patients.
- Even small doses of respiratory depressants such as opioids affect ventilatory effort: opioid-sparing techniques are indicated when possible, and short- or ultra-short-acting opioids are preferable. The use of regional block techniques (eg, transversus abdominis plane [TAP] block) or neuraxial techniques to provide analgesia can reduce systemic opioid requirements.
Cardiac
- Conduction defects: atrioventricular block, bundle branch block, intraventricular conduction block
- Dysrhythmia(s)
- Dilated cardiomyopathy
- Exaggerated cardiac decompensation with anaesthetic induction agents
Anaesthetic Considerations
- Antenatal workup should include an electrocardiogram (ECG) and echocardiography if indicated
- Telemetry may be indicated during labour and the postpartum period
Gastrointestinal
- Abnormal swallowing due to reduced coordination of oesophageal muscles
- Decreased lower oesophageal sphincter tone
- Delayed gastric emptying and gastric dilation
Anaesthetic Considerations
- Neuraxial anaesthetic techniques (spinal, combined spinal-epidural [CSE] or epidural) avoid exposing the patient to the risk of pulmonary aspiration that exists with general anaesthesia (GA) and avoids muscle relaxants.
- If GA is indicated, premedication with oral sodium citrate and a rapid sequence induction with cricoid pressure are recommended.
Metabolic
Myopathy can be associated with abnormal cellular glucose and fat metabolism, which can be exacerbated by the stress response to surgery or labour.
Anaesthetic Considerations
- Frequent blood glucose and lactate monitoring is advisable (an arterial line for perioperative blood sampling may be useful).
Central Nervous System
- Association with learning difficulties; consent implications
Musculoskeletal System
- Association with skeletal muscle weakness and dystrophic changes
- Association with scoliosis
- Risk of rhabdomyolysis
Anaesthetic Considerations
- Scoliosis can be associated with restrictive lung disease and associated respiratory failure; a titrated catheter-based neuraxial technique may have advantages over a single-shot spinal (eg, an epidural or CSE), and peripartum respiratory support may be required.
- Scoliosis and/or corrective spinal surgery (eg, Harrington rods) can make placement of epidurals difficult and is associated with increased risk of failure and complications.
- Consider total intravenous anaesthesia (TIVA) if GA is required.
- Monitor creatinine kinase, potassium and renal function (myoglobulinuria secondary to rhabdomyolysis) perioperatively.
Other Anaesthetic Considerations
- Attention to temperature control during the perioperative period helps prevent myotonic crisis.
- Prolonged fasting may trigger myotonic crisis and avoid excessive preoperative fasting.
Medical Emergencies Associated With Myopathies
Myotonic Crisis
Myotonic crisis is a unique complication associated with myotonic dystrophy12 in which patients develop localised or generalised sustained muscular contraction, which are unresponsive to neuromuscular blockade with regional, neuraxial or general anaesthesia. It may make bag-mask ventilation and intubation difficult, presenting as an anaesthetic emergency.
Prevention is important; temperature should be controlled with active warming perioperatively, and precipitants (eg, suxamethonium, excessive shivering) should be avoided. If a generalised crisis occurs, a supportive approach is advocated with intubation and ventilation as required. Pharmacologic treatments such as procainamide, melixetine, dantrolene and phenytoin have been suggested; however, these pharmacologic treatments should be guided by neurologists and/or intensive care physicians with relevant expertise 1,8.
Rhabdomyolysis and Malignant Hyperpyrexia
Myopathic patients are prone to develop rhabdomyolysis upon surgical stress insults due to unstable muscle membrane integrity. This might lead to hyperkalaemia and the release of excessive creatinine kinases, resulting in acute renal failure. Optimisation of intravenous fluid replacement and pre- and postoperative monitoring of renal functions are recommended.
Some patients with rare forms of myopathy, such as central core myopathy, are specifically at risk of developing malignant hyperpyrexia (MH) when exposed to anaesthetic drugs. Precautions and appropriate steps to avoid exposure to known MH-triggering agents (eg, volatile anaesthetic agents and suxamethonium) should be taken in cases with high suspicion of MH. A thorough family history and appropriate referral for investigations (eg, muscle biopsy) should be consider antenatally. Neuraxial anaesthesia and TIVA techniques are considered safe in MH.
Neuraxial Anaesthesia and Myopathies
Neuraxial anaesthesia is preferable for caesarean delivery (CD) as compared with GA. The advantages of neuraxial anaesthesia in patients with myopathy are the following:
- Neuraxial anaesthesia avoids exposure to GA and muscle relaxants.
- Small incremental doses allow for titration to effect a reduction in the risk of a high block and cardiovascular instability.
- Neuraxial anaesthesia provides superior postoperative analgesia, reducing systemic opioid requirements.
The disadvantage of neuraxial anaesthesia in patients with myopathy is as follows:
- Associated scoliosis may make neuraxial block placement more difficult and is associated with a higher incidence of block failure and complications.
Spinal Anaesthesia and CSE Techniques
Spinal anaesthesia can be considered for emergency CD in women with normal cardiac function (if time permits). To prevent spinal-induced hypotension, a continuous vasopressor infusion (eg, phenylephrine) and IV fluid co-loading with frequent blood pressure monitoring (eg, 1-minute intervals prior to delivery) are recommended.
An epidural or CSE technique with a low-dose spinal component13,14,15 can be considered as an alternative to GA in myopathic patients with cardiac dysfunction, which allows titrated dosing to effect.
Summary of Anaesthetic Management
Preoperative
- ECG: to assess baseline rhythm
- Holter monitor: to investigate for cardiac dysrhythmia(s)
- Echocardiography: to assess cardiac function and exclude cardiomyopathy
- Chest X-ray
- Pulmonary function test: to assess VC, TLC and peak expiratory flow rate
- Arterial blood gas analysis
Early discussion and referral to tertiary obstetric care unit for support and advice, involving a multidisciplinary team including obstetricians, midwives, anaesthetists, neonatologists, geneticists, neurologists and/or rheumatologists (cardiology and respiratory teams should be involved where indicated). 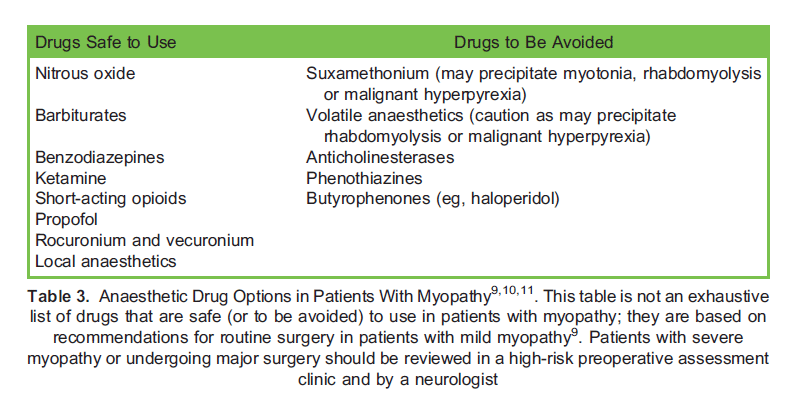
Intraoperative
- Neuraxial anaesthesia: consider titratable technique (eg, low-dose CSE technique or epidural) if evidence of cardiac dysfunction.
- Maintain normothermia
- Frequent blood glucose and lactate monitoring
- If GA performed (eg, for an emergency CD): minimal dose of muscle relaxation (eg, rocuronium) to achieve optimal conditions for laryngoscopy; neuromuscular monitoring; and use sugammadex as a reversal agent where available.
- Use short- or ultra-short-acting opioids
Postoperative
- If respiratory impairment, consider HFNOT (THRIVE device)
- High-dependency care for respiratory monitoring
- Consider opioid-sparing techniques (eg, TAP blocks/postoperative epidural analgesia)
Anaesthetic Drugs and Myopathies
Patients with myopathies have a higher risk of developing postoperative complications following GA. Table 3 highlights common anaesthetic drugs that are considered relatively safe for administration in patients with myopathy and drugs that should be avoided9,10,11.
SUMMARY
Myopathies are multisystem disorders that can affect women of childbearing age. Understanding the pathology and potential anaesthetic complications of myopathies is crucial to safely manage these patients. A multidisciplinary team approach with an agreed delivery plan is essential to ensure safe anaesthetic and obstetric care.
REFERENCES
- Gambling DR, Douglas MJ, McKay RSF. Obstetric Anesthesia and Uncommon Disorders. 2nd ed. Cambridge, UK: Cambridge University Press; 2008.
- Cassandrini D, Trovato R, Rubegni A, et al. Congenital myopathies: clinical phenotypes and new diagnostic tools. Ital J Pediatr. 2017;43(1):101.
- Chinnery PF, Ciafaloni E, Griggs R. Evaluation and Treatment of Myopathies. 2nd ed. Oxford, UK: Oxford University Press; 2014.
- Reeves AG, Swenson RS. Dartmouth Medical School. Disorders of the nervous system. Accessed January 31, 2019. https://www.dartmouth.edu/~dons/part_1/chapter_8.html#chpt_8_reflex_evaluation
- Rudnik-Scho¨ neborn S, Zerres K. Outcome in pregnancies complicated by myotonic dystrophy: a study of 31 patients and review of the literature. Eur J Obstet Gynecol Reprod Biol. 2004;114(1):44-53.
- Russell SH, Hirsch NP. Anaesthesia and myotonia. Br J Anaesth. 1994;72:210-216.
- Ng I, Krieser R, Mezzavia P, et al. The use of Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) for pre-oxygenation in neurosurgical patients: a randomised controlled trial. Anaesth Intensive Care. 2018;46(4):360-367.
- Trip J, Drost GG, van Engelen BGM, Faber CG. Drug treatment for myotonia. Cochrane Database Syst Rev. 2006;(1):CD004762. doi:10.1002/14651858.CD004762.pub2
- Trevisan CP, Accorsi A, Morandi LO, et al. Undiagnosed myopathy before surgery and safe anaesthesia table. Acta Myol. 2013;32(2):100-105.
- Klingler W, Lehmann-Horn F, Jurkat-Rott K. Complications of anaesthesia in neuromuscular disorders. Neuromuscul Disord. 2005;15:195-206.
- Racca F, Mongini T, Wolfler A, et al. Recommendations for anesthesia and perioperative management of patients with neuromuscular disorders. Minerva Anestesiol. 2013;79:419-433.
- Benito-Leo´ n J, Aguilar-Gala´ n EV. Recurrent myotonic crisis in a pregnant woman with myotonic dystrophy. Eur J Obstet Gynecol Reprod Biol. 2001;95(2):181.
- Roofthooft E, Van de Velde M. Low-dose spinal anaesthesia for caesarean section to prevent spinal-induced hypotension. Curr Opin Anaesthesiol. 2008;21(3):259-262. doi:10.1097/ACO.0b013e3282ff5e41
- Teoh WH, Thomas E, Tan HM. Ultra-low dose combined spinal-epidural anesthesia with intrathecal bupivacaine 3.75 mg for cesarean delivery: a randomized controlled trial. Int J Obstet Anesth. 2006;15(4):273-278.
- Van de Velde M. Low-dose spinal anesthesia for cesarean section to prevent spinal-induced hypotension. Curr Opin Anaesthesiol. 2019;32(3):268-270.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/