Regional Anaesthesia

Key Points
- Pericapsular Nerve (PENG) Block is a novel regional anaesthesia technique which has been suggested as an alternative to existing blocks to reduce pain following hip fractures and hip surgery.
- It involves blocking, with one ultrasound-guided injection, the articular branches of the femoral nerve, the obturator nerve and, where present, the accessory obturator nerve to the hip.
- Case series have suggested that PENG block has the potential to provide comparable or greater analgesic benefit than existing techniques such as femoral nerve or fascia iliaca blocks.
- PENG block is a motor sparing block, targeting only the sensory innervation of the hip, potentially allowing for earlier mobilisation and recovery postoperatively.
Introduction
Hip fracture is the most common serious injury in the elderly population, and is also the most common cause for older people to need emergency surgery. Age-standardised annual rates of hip fracture are 260-349/100,000 in women and 122-140/100,000 in men in the USA and UK 1. Surgical reduction and fixation is the definitive treatment in the majority of cases 2. Meanwhile, total hip arthroplasty is the international standard of care for degenerative hip joint disease. The average rate of total hip replacement among the 38 countries of the Organisation for Economic Co-operation and Development (OECD) is 182 procedures per 100,000 members of the population 3.
A number of regional analgesia techniques to alleviate pain following hip fracture and hip arthroplasty surgery exist, though many may have undesirable side effects. Regional techniques, including femoral nerve (FN) block, fascia iliaca compartment block (FICB) and femoral 3-in-1 block, are used regularly due to their ability to reduce postoperative pain, as well as reducing opioid consumption and related adverse effects of opioids 2. However, recent anatomical studies have shown that the articular branches of both the femoral and obturator nerve, those which innervate the anterior hip capsule, may not be optimally blocked by these techniques 4. These blocks also generally cause a degree of motor blockade, which can delay post-operative mobilisation.
The Pericapsular Nerve Group (PENG) block is a novel regional anaesthesia technique, first described in 2018, which can be used as an alternative to femoral nerve block or fascia iliaca compartment block to reduce pain postoperatively after hip surgeries. It targets, with one injection, the nerves supplying the anterior capsule of the hip, namely the obturator nerve, the accessory obturator nerve (where present) and the articular branches of the femoral nerve.
Though still in its infancy, multiple case reports have shown the potential of the PENG block to successfully reduce post-operative pain following hip surgery, as well as reducing opioid consumption and minimising opioid-induced side effects, essential in this elderly patient cohort. It has also been found to be a motor sparing block, with the potential of enabling earlier postoperative mobilisation for patients 2.
This tutorial will examine the literature available on the clinical application of the PENG block. We will discuss the anatomical basis for the block’s success and describe the technique itself, before looking ahead to examine what the future may hold for the PENG block.
What is the PENG Block?
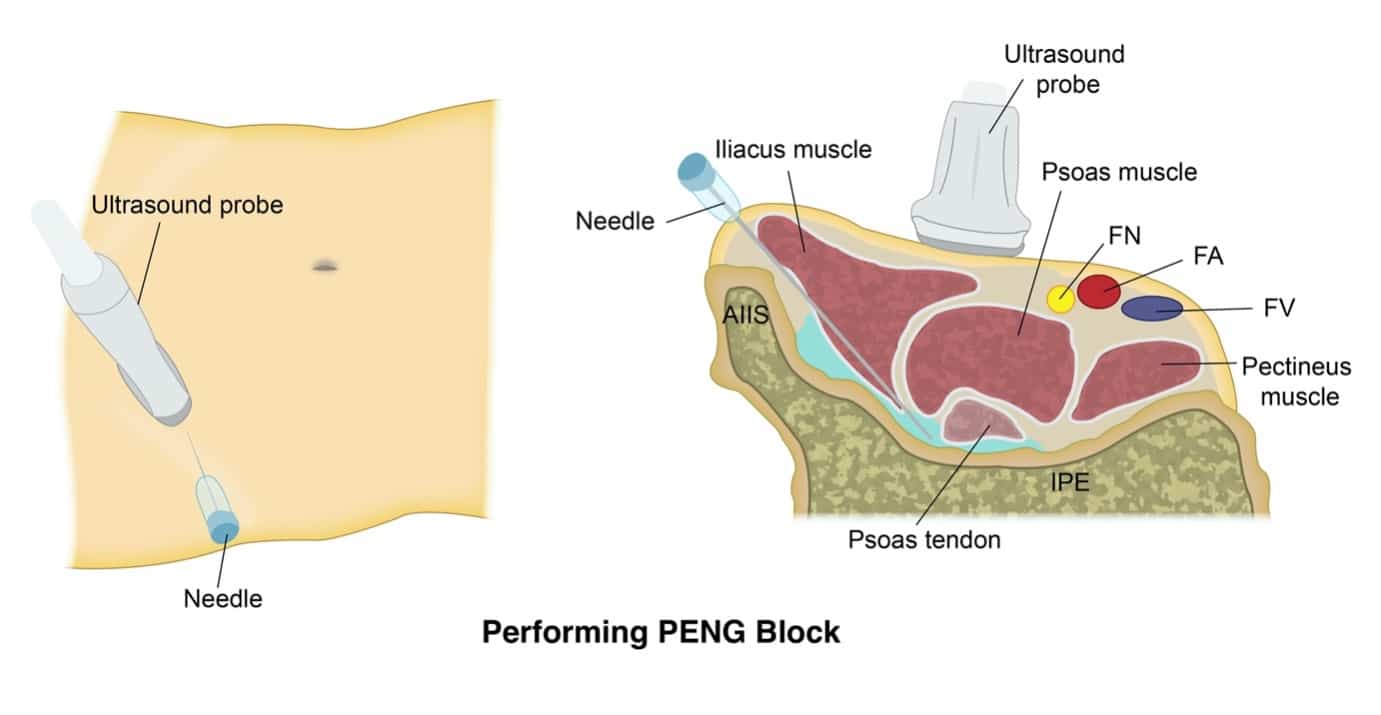
Figure 1. Diagrammatic representation of the Pericapsular Nerve Group block being performed. AIIS = Anterior inferior iliac spine, IPE = iliopectineal eminence. FN = femoral nerve, FA = femoral artery, FV = femoral vein.
The PENG Block is a regional analgesia technique, first described in 2018 by Giron-Arango et al. as a novel approach to reducing postoperative pain and opioid consumption in patients following hip fracture surgery. It is a plane block involving one injection, performed under ultrasound guidance, of a high volume of local anaesthetic into the musculofascial plane between the psoas tendon anteriorly and the pubic ramus posteriorly 2 (See Figure 1).
This first study by Giron et al. described the technique and its successful application in five patients with hip fracture. The PENG block showed a clinically relevant reduction in pain scores, comparable to alternative regional techniques. The technique was also found to have a potential motor-sparing effect when compared with the FN block and FICB, with no quadriceps weakness reported in any of the five patients post-operatively 2.
Anatomical Basis for the PENG Block’s Success
One of the principal challenges of effective regional analgesia for hip pain is the complex innervation of the hip joint by multiple nerves. Recent anatomical studies of the hip joint have clarified this anatomy. The anterior hip capsule has been shown to be supplied by articular branches of the femoral, obturator and accessory obturator nerves, where present 4. The posterior capsule is innervated most commonly by the nerve to the quadratus femoris, while small articular branches from the sciatic nerve and superior gluteal nerves may also be seen 5. The anterior capsule, which contains the majority of the sensory innervation of the joint and has been identified as the main source of the majority of postoperative hip pain, is the target for the PENG block 3,4.
Short et al further demonstrated that “high” sensory articular branches of the femoral nerve, originating cranially to the inguinal ligament, play a greater role in the innervation of the anterior hip capsule than previously thought. These articular branches enter the iliacus muscle at the L4-L5 level, travel deep to the psoas muscle between the anterior inferior iliac spine and iliopubic eminence before innervating the hip capsule 4. The accessory obturator nerve is present in 10-30% of cases. It courses deep to the psoas muscle from the L5 level before innervating the medial aspect of the hip joint capsule 4.
The spread of local anaesthetic after infrainguinal regional analgesia techniques targeting the hip capsule, such as infrainguinal FICB and femoral 3-in-1 block have been studied in separate studies using magnetic resonance. It has been shown that the cephalad spread of local anaesthetic after these blocks is unlikely to extend above L5 6. Therefore, neither the infrainguinal FICB nor the femoral 3-in-1 block are likely to consistently block the articular branches of the femoral nerve or the accessory obturator nerve. Further studies have also shown that these regional techniques also frequently fail to adequately block the obturator nerve 7. These anatomical findings explain why it is difficult to achieve optimum analgesia for the hip joint using infrainguinal regional techniques such as the FN block, FICB or femoral 3-in-1 block. More recently, a suprainguinal approach to the FICB has been proposed, and was shown to provide a more consistent spread of local anaesthetic in a cranial direction under the fascia iliaca. This suprainguinal FICB provided a more reliable spread to the anatomical location of the three target nerves on MRI than an infrainguinal approach 8.
The PENG block is also a suprainguinal approach to targeting pain arising from the hip capsule. The high articular branches of the femoral nerve and the accessory obturator nerve have been consistently found between the anterior inferior iliac spine and the iliopubic eminence, while the obturator nerve runs close by, in close proximity to the inferomedial acetabulum 7. Using these anatomical details, the PENG block can be applied to block all three nerves which innervate the anterior capsule of the hip with one injection of local anaesthetic.
Mechanism of Action
The PENG block is an interfascial plane block, targeting the plane between the psoas tendon anteriorly and the pubic ramus posteriorly. Deep fascial planes are potential spaces and can act as ‘transmission belts’ for the spread of local anaesthetic within the body. The efficacy of interfascial plane blocks relies on the local anaesthetic agent passively distributing with the plane to reach the target nerves. To date, there has been one study investigating the spread of local anaesthetic following PENG block 9. Tran et al. performed the PENG block in a cadaveric specimen, injecting methylene blue and observing the staining pattern within the hip joint. The dye spread in the bursal space between the iliopsoas and anterior hip joint and stained the entire anterior hip joint capsule. Though further research is required to verify these results and determine the optimal volume of local anaesthetic for the block, this study provides support that the block successfully captures the articular branches of the femoral, obturator and accessory obturator nerves, as originally described 9.
One limitation of the PENG block is that the lateral femoral cutaneous nerve (LFCN) is not routinely blocked by the technique. Due to skin incision and subcutaneous dissection, postoperative pain after posterior and direct lateral approach hip surgery will usually include dermatomal pain for the lateral thigh supplied by the LFCN. A combination of PENG block with LFCN block (or incision site infiltration with local anaesthetic) may provide better analgesia than PENG block alone for this reason 10.
Technical Performance of the PENG Block

Figure 2. Sonographic anatomy of the Pericapsular Nerve Group Block.
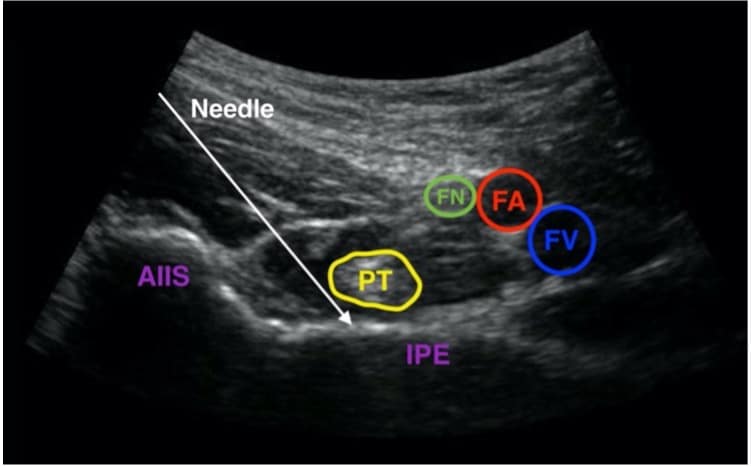
Figure 3. Same image as figure 2, labelled and with intended needle course.
AIIS = Anterior inferior iliac spine, PT = psoas tendon, IPE = iliopectineal eminence. FN = femoral nerve, FA = femoral artery, FV = femoral vein.
The PENG block is performed with the patient in the supine position and the operator standing on the ipsilateral side of the affected limb. The ultrasound machine should be positioned with the screen in a direct line of sight. A low-frequency (curvilinear) ultrasound probe (2-5MHz) is initially placed in a transverse plane over the anterior inferior iliac spine, before being aligned with the pubic ramus by rotating the probe 45 degrees counter clockwise (See Figure 1). It should be possible to observe the iliopubic eminence, the iliopsoas muscle tendon, the femoral artery and pectineus muscle in this view. The femoral nerve should be identified during scanning prior to needle insertion. An 80mm sonographic needle should be inserted from lateral to medial in an in-plane approach, with the aim of placing the tip in the musculofascial plane between the psoas tendon anteriorly and the pubic ramus posteriorly (see Figures 2 and 3). Negative aspiration should be observed before injection of local anaesthetic into the plane and observation of fluid spread in the desired plane 2.
There are no studies published to date examining the effect of varying the specific local anaesthetic used or the volume used. In their original case series, Giron et al performed the majority of their PENG blocks with 20mls of 0.25% bupivacaine and epinephrine 1:400,000. In general, a high volume of local anaesthetic has been used in the majority of published case reports and case series describing PENG blocks, with 20-30mls of 0.25%-0.5% bupivacaine or levobupivacaine commonly used, with or without epinephrine. Dexamethasone has been used as an additive by some authors to extend the duration of the block 11.
PENG Block in the Literature
Since the first publication in Regional Anaesthesia and Acute Pain in late 2018 of the paper by Giron-Arango et al, the PENG block has generated a wide level of interest. Due to the relative infancy of the PENG block, the available literature on the technique is largely limited to case reports and cohort studies, with a scarcity of randomised control trials completed on the efficacy of the procedure to date. A wide range of published case studies indicate the potential of the PENG block to significantly improve hip joint analgesia, however, and multiple larger clinical trials investigating the technique are currently ongoing.
Successful Analgesic Outcomes
The PENG block has many potential advantages over traditional regional analgesia techniques used for pain originating in the hip capsule. Principally, the block has the potential to achieve a wider coverage of sensory nerves innervating the hip, improving analgesia and reducing postoperative pain. This may lead to reduced postoperative opioid consumption, resulting in less opioid-related side effects and less long-term opioid dependency 11.
As expected, the majority of the available literature regarding the PENG block involves its use in hip fracture patients or those undergoing hip surgery. A 2020 review of the available literature on PENG blocks performed for hip fractures and hip surgeries highlighted twenty case reports and case series, encompassing a combined total of 74 patients. In all twenty studies, the PENG block was shown to provide sufficient analgesia or anaesthesia 11. In Giron-Arango’s first study, PENG block in patients with hip fractures reduced pain scores by a median of 7 points on a 10 point Numerical Rating Scale 2. A recent single-centre randomised control trial comparing PENG block to ‘no block’ in patients undergoing total hip arthroplasty also showed that pain scores of patients who received PENG block were significantly reduced when compared to patients in the ‘no block’ group. The PENG block patients also showed a significant reduction in opioid consumption, better range of hip motion and shorter time to ambulation after surgery 12.
Other Benefits
The PENG block targets only the sensory innervation of the hip, and case studies have reported a potential motor-sparing effect when compared with the FN block and FI block 2. In a larger, randomised comparison between PENG block and suprainguinal fascia iliaca block for patients undergoing primary total hip arthroplasty, PENG block resulted in a lower incidence of quadriceps motor block and an increased preservation of hip adduction than suprainguinal fascia iliaca block, with no significant difference between the groups in postoperative pain scores, opioid consumption or length of hospital stay 13. Absence of motor blockade after PENG block may allow earlier patient mobilisation postoperatively and earlier participation in rehabilitation, contributing to an early recovery 11. Motor sparing lower limb blocks can also lead to a reduction in postoperative falls risk when compared to non-motor sparing alternatives, though it must be noted that quadriceps weakness can still occur if inadvertent FN block or FICB occurs following PENG block (see Adverse Effects, below). Further investigation is required to ascertain the optimum local anaesthetic volume to reliably provide motor-sparing PENG block, while research comparing PENG block with other motor-sparing strategies such as periarticular local anaesthetic infiltration would also be helpful 13.
The easily identifiable sonographic structures involved in PENG block – including the anterior inferior iliac spine, the iliopubic eminence and the psoas tendon – make the technical performance of the block comparable to existing nerve blocks in terms of difficulty. This is supported by a lack of any serious adverse events after PENG block such as permanent nerve injury, vascular damage or local anaesthetic systemic toxicity reported in the literature to date, though it must be considered that the current literature is as yet too limited to make definitive assumptions regarding the safety of the technique.
Adverse Effects and Risks
To date, two cases of motor weakness of the quadriceps following PENG block have been reported 14. In each case, the block was performed postoperatively and was reported to be technically challenging. The weakness was transient in both cases, and has been attributed to inadvertent femoral nerve or fascia iliaca blockade. Yu et al. hypothesised that injection of local anaesthetic more superficially than intended, or needle placement medial to rather than posterior to the psoas tendon, may result in superficial spread of a proportion of the local anaesthetic and cause inadvertent FN or FI block. They also cautioned that postoperative performance of the block may allow spread of local anaesthetic to unanticipated locations due to normal tissue planes being disrupted by surgery 14.
When performing the PENG block, there is potential for the needle path to traverse both the femoral nerve or the LFCN of the thigh. It is vital to identify the femoral nerve in the scanning phase of the block, prior to needle insertion, to minimise risk of injury. The LFCN has a smaller calibre and follows a more variable course as it passes into the anterior thigh below the inguinal ligament, making it more challenging to locate on ultrasound 10. Any complaints of lateral thigh pain after needle insertion requires a prompt re-assessment of the anatomy. The pelvic part of the ureter must also be considered. It lies on the pelvic wall in close proximity to the obturator nerve, where it has the potential to be injured by a more medial needle advancement or a medial to lateral needling technique 15. Despite these concerns, no injuries to femoral nerve, lateral femoral cutaneous nerve or ureter have been described following PENG block in the literature to date.
Limitations of the Literature
The PENG block remains in its infancy with most data in the literature arising from case reports or case series. There are limitations inherent to these types of study, including publication bias and danger of overinterpretation. There is also no consensus on optimum injectate and volume, making comparisons between studies difficult.
A number of larger trials regarding the efficacy of the PENG block are ongoing as per the U.S National Library of Medicine’s clinicaltrials.gov, though these are unpublished works at the time of writing. Ongoing research of interest includes randomised trials comparing PENG block to ‘no block’ for primary hip arthroplasty, PENG block vs. wound infiltration for hip replacement and PENG block vs. FICB block in hip fracture patients. Studies comparing the efficacy of PENG block after different types of hip surgery (hemiarthroplasty vs. DHS, for example) and after procedures involving different surgical approaches to the hip (anterior vs. posterior) may be areas of interest for the future. Anatomic studies may also be useful to confirm the extent and reliability of spread of local anaesthetic to the targeted nerves, as may a large cohort study to definitively investigate the safety of the technique.
Summary
The PENG block is a novel regional anaesthesia technique which can be viewed as an alternative to FN block or FICB in the treatment of pain originating from the hip. Though the literature published to date is largely limited to case reports and case series, it has been shown to have the potential to provide greater analgesic benefit than existing regional analgesia techniques for patients with hip fractures or undergoing hip surgery. There has been no major adverse events reported arising from the technique, while it also has the potential to spare the motor innervation of the lower limb. Larger studies are required to determine its true efficacy when compared with other regional techniques and its safety, as well as optimum injectate volume.
References
- Kanis, JA, Oden A, McCloskey, EV, Johansson, H, Wahl DA, Cooper C, 2012. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporosis international. 2012; 23(9):2239-2256.
- Girón-Arango L, Peng PW, Chin KJ, Brull R, Perlas A. Pericapsular nerve group (PENG) block for hip fracture. Regional Anesthesia & Pain Medicine. 2018; 1;43(8):859-63.
- McPherson K, Gon G, Scott M. International variations in a selected number of surgical procedures. OECD Health Working Papers, No. 61. 2013.
- Short AJ, Barnett JJ, Gofeld M, Baig E, Lam K, Agur AM, Peng PW. Anatomic study of innervation of the anterior hip capsule: implication for image-guided intervention. Regional Anesthesia & Pain Medicine. 2018; 1;43(2):186-92.
- Nagpal AS, Brennick C, Occhialini AP, Leet JG, Clark TS, Rahimi OB, Hulk K, Bickelhaupt B, Eckmann MS. Innervation of the Posterior Hip Capsule: A Cadaveric Study. Pain Med. 2021; 22(5):1072-1079.
- Marhofer P, Našel C, Sitzwohl C, Kapral S. Magnetic resonance imaging of the distribution of local anesthetic during the three-in-one block. Anesthesia & Analgesia. 2000; 1;90(1):119-24.
- Swenson JD, Davis JJ, Stream JO, Crim JR, Burks RT, Greis PE. Local anesthetic injection deep to the fascia iliaca at the level of the inguinal ligament: the pattern of distribution and effects on the obturator nerve. Journal of Clinical Anesthesia. 2015; 1;27(8):652-7.
- Vermeylen K, Desmet M, Leunen I, Soetens F, Neyrinck A, Carens D, Caerts B, Seynaeve P, Hadzic A, Van de Velde M. Supra-inguinal injection for fascia iliaca compartment block results in more consistent spread towards the lumbar plexus than an infra-inguinal injection: a volunteer study. Regional Anesthesia & Pain Medicine. 2019; 44(4):483-491.
- Tran J, Agur A, Peng P. Is pericapsular nerve group (PENG) block a true pericapsular block?. Regional Anesthesia & Pain Medicine. 2019; 1;44(2):257.
- Roy R, Agarwal G, Pradhan C, Kuanar, D. Total postoperative analgesia for hip surgeries, PENG block with LFCN block. Regional Anesthesia & Pain Medicine. 2019; 0:1.
- Morrison C, Brown B, Lin DY, Jaarsma R, Kroon H. Analgesia and anesthesia using the pericapsular nerve group block in hip surgery and hip fracture: a scoping review. Regional Anesthesia & Pain Medicine. 2021; 1;46(2):169-75.
- Pascarella, G., Costa, F., Del Buono, R., Pulitanò, R., Strumia, A., Piliego, C., De Quattro, E., Cataldo, R., Agrò, F.E., Carassiti, M. and collaborators, 2021. Impact of the pericapsular nerve group (PENG) block on postoperative analgesia and functional recovery following total hip arthroplasty: a randomised, observer‐masked, controlled trial. Anaesthesia. 2021; 76:1492-1498.
- Aliste J, Layera S, Bravo D, Jara Á, Muñoz G, Barrientos C, Wulf R, Brañez J, Finlayson RJ, Tran Q. Randomized comparison between pericapsular nerve group (PENG) block and suprainguinal fascia iliaca block for total hip arthroplasty. Regional Anesthesia & Pain Medicine. 2021; Oct;46(10):874-878.
- Yu HC, Moser JJ, Chu AY, Montgomery SH, Brown N, Endersby RV. Inadvertent quadriceps weakness following the pericapsular nerve group (PENG) block. Regional Anesthesia & Pain Medicine. 2019; 1;44(5):611-3.
- Mistry T, Sonawane KB, Kuppusamy E. PENG block: points to ponder. Regional Anesthesia & Pain Medicine. 2019; 1;44(3):423-4.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/