General Topics

KEY POINTS
- Thyroid storm is a life-threatening condition characterised by overt thyrotoxicosis in the setting of longstanding untreated or undertreated hyperthyroidism.
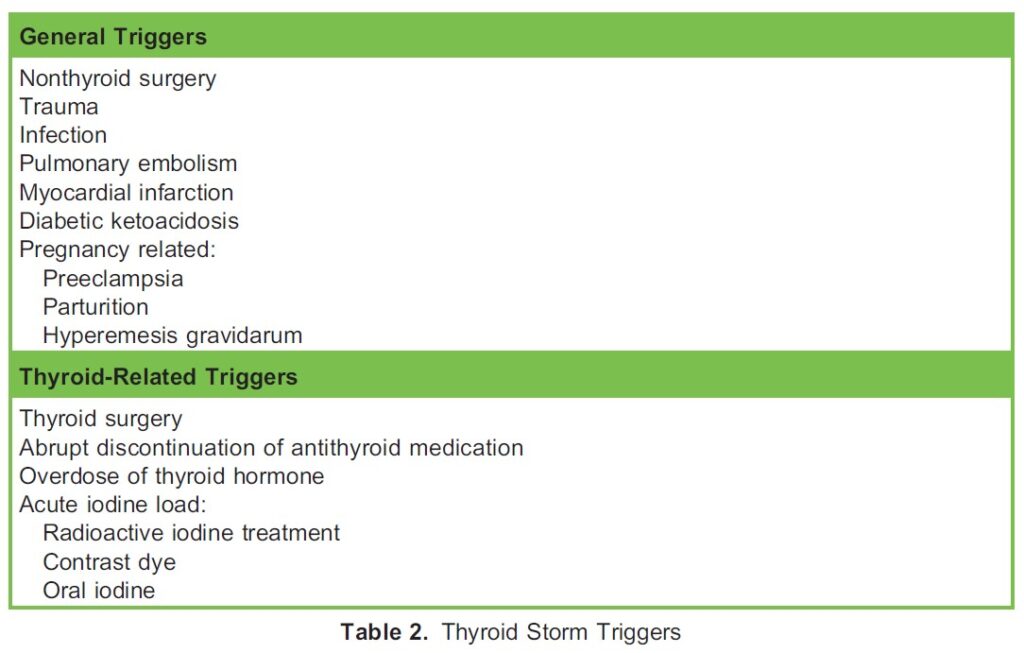
- It may be triggered by an acute stress event such as abrupt discontinuation of antithyroid medication, infection, or surgery.
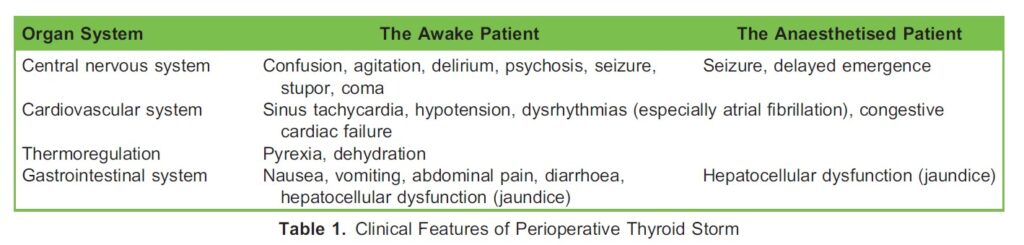
- In the awake patient, neurological, cardiovascular, thermoregulatory, and gastrointestinal dysfunction characterise the predominant clinical abnormalities.
- In the anaesthetised patient, intraoperative signs may be limited to pyrexia, tachycardia, and atrial fibrillation, making the diagnosis more difficult.
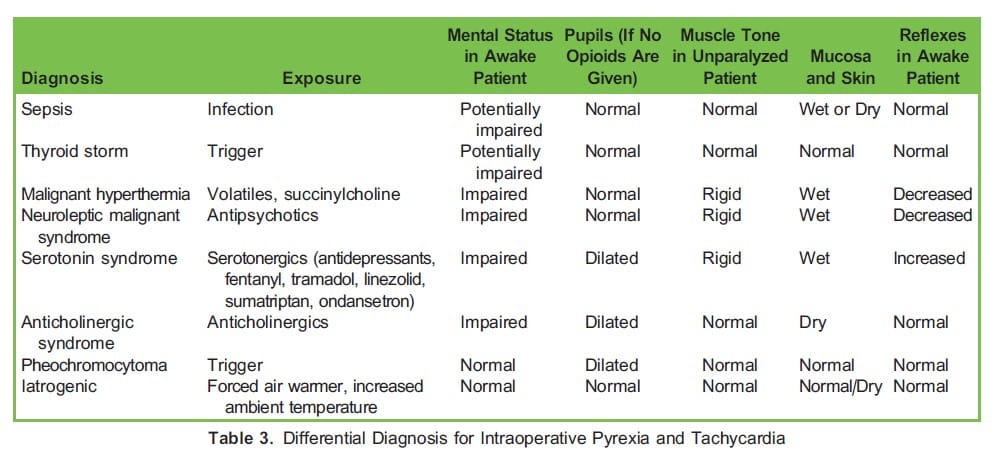
- The differential diagnosis for an intraoperative thyroid storm should include sepsis, malignant hyperthermia, neuroleptic malignant syndrome, serotonin syndrome, pheochromocytoma, and anticholinergic syndrome.
- Perioperative management should include general supportive measures (airway, breathing, circulation, and temperature management) as well as specific pharmacological interventions (beta-blockade, thionamide, iodine, and glucocorticosteroids).
INTRODUCTION
A paucity of literature exists regarding the intraoperative recognition and management of a thyrotoxic crisis, more commonly known as a thyroid storm. Due to the rarity of this condition1-3 and the various nonspecific clinical manifestations of a thyroid storm under anaesthesia,4 prompt diagnosis and initiation of treatment remain a challenge but are very important.5 This tutorial will focus on this rare but life-threatening complication of thyrotoxicosis, provide a stepwise approach to supportive and pharmacological management, and provide guidance on the optimisation of patients in the perioperative period.
Definition
Hyperthyroidism, thyrotoxicosis, and thyroid storm are 3 separate clinical conditions that should not be confused with one another.
- Hyperthyroidism is a biochemical diagnosis that is defined by an increase in circulating thyroid hormone levels.6
- Thyrotoxicosis refers to a group of signs and symptoms induced by the thyroid hormones’ inappropriate activation in the tissue and should be seen as the clinical manifestation of hyperthyroidism.6
- A thyroid storm is an acute life-threatening endocrine emergency resembling an exaggerated presentation of thyrotoxicosis.7
Basic Thyroid Physiology
The thyroid’s main function is to convert iodine into thyroid hormones: the prohormone thyroxine (T4) and the bioactive hormone triiodothyronine (T3). Thyroid cells combine iodine and tyrosine to form T3 and T4. The normal thyroid gland produces about 80% T4 and 20% T3. The majority of T3 is produced by enzymatic deiodination of T4 in peripheral tissues by iodothyronine deiodinases. The thyroid gland is under the control of the anterior pituitary gland, which secretes thyroidstimulating hormone (TSH) and stimulates the production of T3 and T4. TSH is produced and released from the anterior pituitary gland in response to thyrotropin-releasing hormone (TRH) released from the hypothalamus and carried to the pituitary via the hypothalamohypophyseal portal system. The hypothalamus can also inhibit TSH secretion via the effects of released somatostatin, in the same way that growth hormone inhibition occurs. Free T3 and free T4 in the plasma exert a negative feedback effect on the hypothalamus and the pituitary to regulate the circulating levels.8
Incidence and Mortality
The majority of epidemiological data on thyroid storm are from national surveys in Japan and the United States. Thyroid storm incidence ranges from 0.20 to 0.76 per 100 000 people per year.9,10 Intraoperative and postoperative thyroid storm following nonthyroid surgery has rarely been reported, with 24 cases identified in the literature between 1930 and 2018.5 The rarity of this intraoperative emergency is due to the widespread use of antithyroid medication to achieve a euthyroid state prior to surgery. Mortality rates of thyroid storm range between 10% and 30% despite early diagnosis.1,7,9
Clinical Features
Symptoms of thyrotoxicosis include heat intolerance, palpitations, anxiety, fatigue, weight loss, muscle weakness, and, in women, irregular menses. Clinical findings may include tremors, tachycardia, lid lag, and warm moist skin. The clinical picture of thyroid storm is characterised Cby nonspecific signs ranging from thermoregulatory dysfunction to thyrotoxic heart disease
(cardiothyreosis)1 (Table 1).
CLINICAL MANIFESTATION
The exact mechanisms underlying the development of a thyroid storm are poorly understood. Thyroid storm occurs in undiagnosed or uncontrolled hyperthyroidism or thyrotoxicosis in the presence of a trigger.11 A heightened cellular response to thyroid hormone is implicated, as seen during acute stress. The increased or abrupt availability of free hormones results in enhanced responsiveness to catecholamines. It is postulated that a rapid increase in thyroid hormone, rather than the actual hormone level, leads to the development of a thyroid storm. A thyroid storm must be triggered regardless of the aetiology of hyperthyroidism and thyrotoxicosis; however, in up to 30% of patients no trigger can be identified.
Triggers
Thyroid storm can develop in untreated or poorly controlled hyperthyroidism but it is more commonly precipitated by an acute event. The literature describes several precipitating factors, or triggers, including abrupt discontinuation of antithyroid medication, infection, surgery (thyroid and nonthyroid), trauma, preeclampsia, parturition, hyperemesis gravidarum, diabetic ketoacidosis, and acute iodine overload (radioactive iodine treatment, iodine in contrast studies, and oral iodine) (Table 2).2,3
Diagnosis
The diagnosis of thyroid storm is challenging due to the nonspecific clinical features and rarity. The diagnosis is further hampered due to the continuum of severity ranging from thyrotoxicosis to thyroid storm. No laboratory abnormalities are specific to thyroid storm. Hyperthermia, mental state changes (irritability, delirium, psychosis, lethargy, coma), hypotension, tachycardia, dysrhythmias, and gastrointestinal and hepatocellular dysfunction characterise the clinical scenario in an awake patient with thyroid storm (Table 1).9
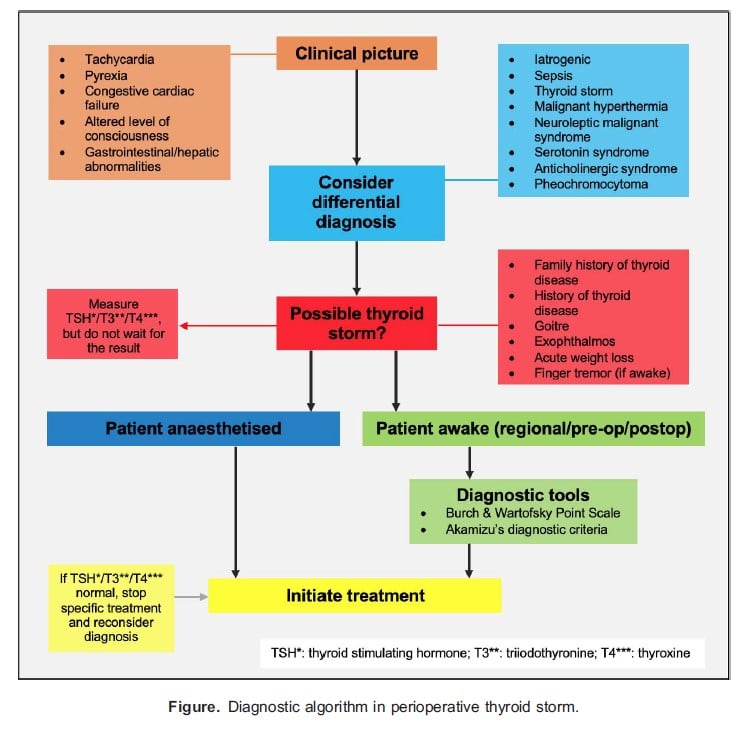
The diagnosis of intraoperative storm is a difficult task as the only clues may be intraoperative pyrexia and tachycardia. Mental state changes and gastrointestinal dysfunction will not be detected in a patient under general anaesthesia. Tachycardia has numerous causes and may indicate pain, awareness, hypovolemia, haemorrhage, medication side effects, or bladder distension. A rise in temperature and end-tidal carbon dioxide may be a sign of sepsis, malignant hyperthermia, neuroleptic malignant syndrome, serotonin syndrome, pheochromocytoma, or anticholinergic syndrome.12 Atypical presentations have been described under general anaesthesia in which the patient does not develop a fever. In the setting of a caesarean section under neuraxial anaesthesia, haemorrhage and hormonal changes can obscure the symptoms of thyrotoxicosis, making the intraoperative diagnosis even more challenging.
A stepwise diagnostic approach should be followed when a patient under general anaesthesia develops intraoperative tachycardia or pyrexia (Figure).13,14 The differential diagnosis for pyrexia and tachycardia should be considered initially (Table 3).12
Diagnostic Tools
Certain diagnostic tools can aid in diagnosing a thyroid storm in the awake patient in the preoperative and postoperative periods. The Burch and Wartofsky point scale (BWPS) described in 1993 uses nonspecific features to predict the likelihood of a thyroid storm (Table 4).3
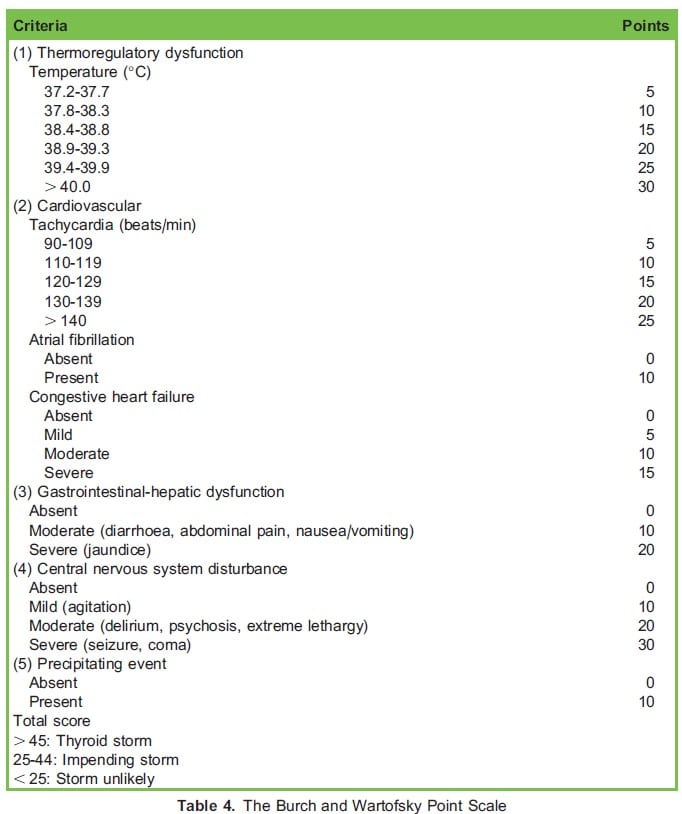
The BWPS has been widely applied for the diagnosis of thyroid storm for more than 2 decades. Central nervous system disturbances are heavily weighted in the BWPS; however, in the anaesthetised patient these disturbances will not be detected. In 2012, the Japanese Thyroid Association proposed diagnostic criteria (the Akamizu diagnostic criteria) that include thyrotoxicosis as a prerequisite condition (Table 5).13
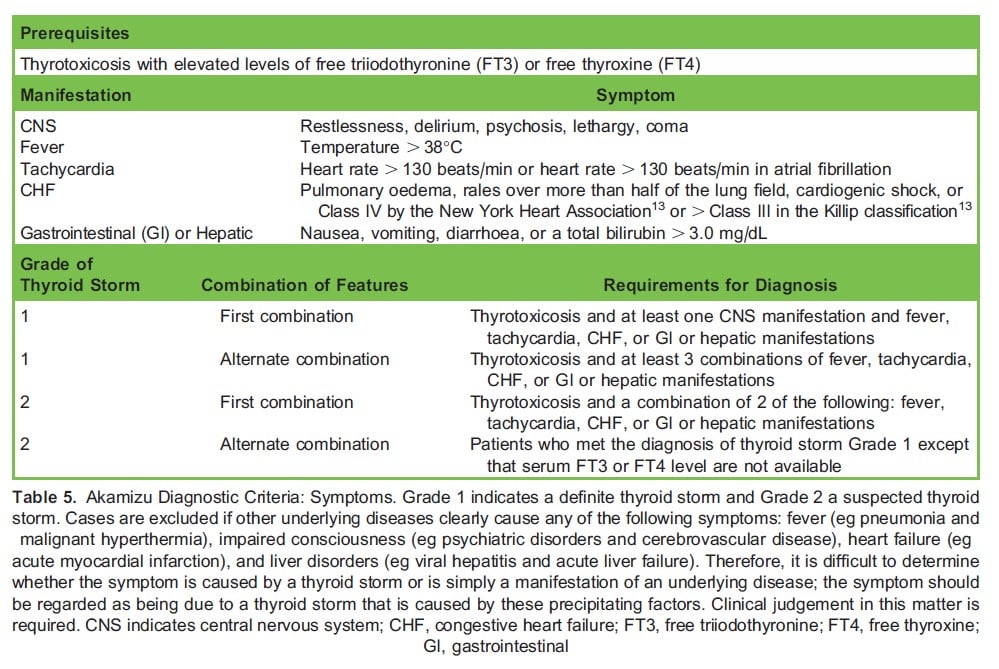
Using both scores to evaluate an awake patient’s condition is recommended to increase diagnostic accuracy. These diagnostic criteria are helpful because they provide a systematic framework to think about the diagnosis. However, we are not forced to rigidly adhere to these criteria for 2 reasons. Firstly, the diagnosis of thyroid storm is partially a diagnosis of exclusion. For example, sepsis with multi-organ failure could easily score .45 on the BWPS. Therefore, a score .45 does not prove a diagnosis of thyroid storm. Secondly, treatment for thyroid storm is reasonable in any patient with severe hyperthyroidism causing organ failure (especially heart failure). Therefore, even if the patient does not have a score .45 on the BWPS, it may be prudent to initiate therapy for thyroid storm.
MANAGEMENT OF INTRAOPERATIVE THYROID STORM
Once the preliminary diagnosis of a thyroid storm has been made, prompt initiation of treatment is of utmost importance. The treatment options for thyroid storm are expanded from those used for uncomplicated hyperthyroidism. The principles of treatment outlined below are based on clinical experience, case studies, the 2016 Japan Thyroid Association Guideline,13 and the 2016 American Thyroid Association Guideline.14
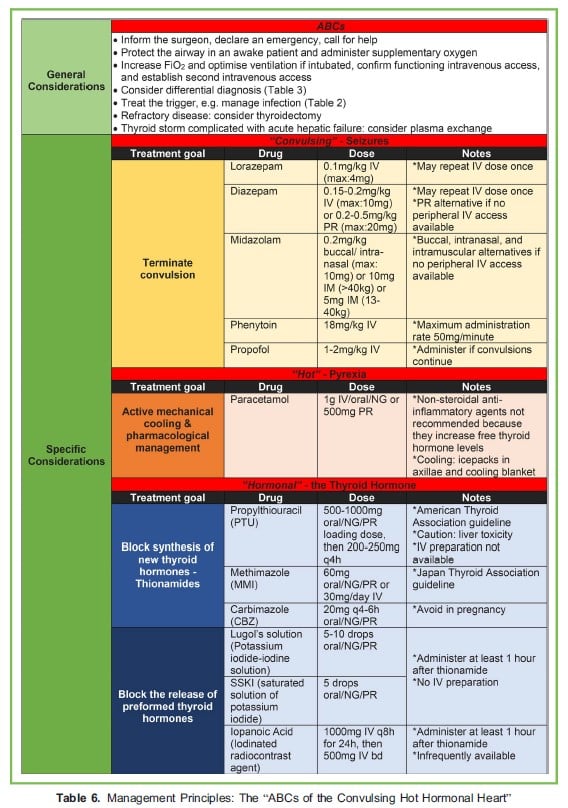
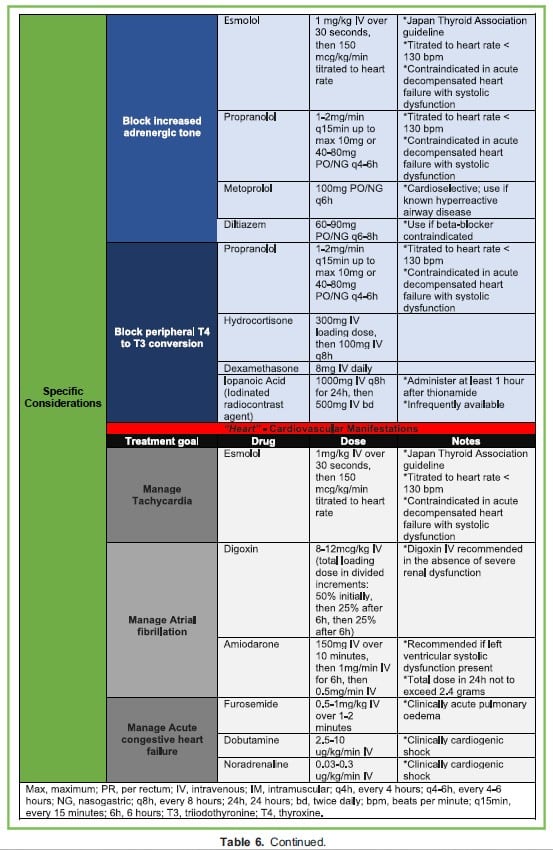
Management principles can be divided into general considerations and specific considerations (Table 6),13,14 and encompass the following:
- Consideration and exclusion of the differential diagnoses,12
- If thyroid storm is likely, implementation of the “ABCs of the Convulsing Hot Hormonal heart” (Table 6), and
- Consideration of thyroidectomy in refractory cases and plasma exchange in thyroid storm complicated with acute hepatic failure.13
OPTIMISATION PRIOR TO SURGERY
If hyperthyroidism or thyrotoxicosis is diagnosed in the preoperative period in a patient scheduled for elective surgery, it is recommended that surgery and anaesthesia be postponed until the patient is clinically and biochemically euthyroid. Achieving a euthyroid state can take anything from 6 weeks up to 18 months. In consultation with an endocrinologist the patient should be followed up initially after 4 to 6 weeks, then at month 3, month 6, and then at yearly intervals. In the setting of emergency surgery where optimisation might not be an option, a perioperative thyroid storm should be anticipated and adequately prepared for. Premedication in the form of a beta-blocker (propranolol 0.1-0.15 mg/kg intravenously [IV]), antithyroid drug (propylthiouracil 200- 400 mg orally), and a corticosteroid (hydrocortisone 300 mg IV) should be administered. Where possible, regional anaesthesia and peripheral nerve block are preferable to general anaesthesia. If the surgical procedure does not allow for a regional anaesthetic technique, proceed with general anaesthesia ensuring that the intubation response is blunted, analgesia and depth of anaesthesia are adequate, and a smooth emergence and extubation are performed.15 Vigilance regarding thyroid storm should extend into the postoperative care period; therefore it is recommended that the patient be monitored in a high-dependency unit.
SUMMARY
Thyroid storm in an awake patient remains an elusive diagnosis. In an anaesthetised patient, the diagnosis is even more challenging, and the pharmacological treatment options are limited to a few intravenous medications. In the awake patient, the BWPS and the Akamizu’s diagnostic criteria should form part of the anaesthetist’s assessment. When tachycardia and pyrexia are noted in the patient receiving general anaesthesia, the differential diagnosis including thyroid storm should be considered.
And the waters leapt,
And the wild winds swept,
And blew out the moon in the sky,
And I laughed with glee,
It was joy to me
As the storm went raging by!
The rising of the storm, by Paul Laurence Dunbar
REFERENCES
1. Bourcier S, Coutrot M, Kimmoun A, et al. Thyroid storm in the ICU: a retrospective multicenter study. Crit Care Med. 2020;48:83-90.
2. Goodier CG. Endocrine emergencies in obstetrics. Clin Obstet Gynecol. 2019;62:339-346.
3. Burch HB, Wartofsky L. Life-threatening thyrotoxicosis: thyroid storm. Endocrinol Metab Clin North Am. 1993;22:263-277.
4. Schaefer AW, Solorzano PJ, Mavarez AC, et al. Diagnosis and management of intraoperative thyroid storm in a child with undiagnosed Graves’ disease: a case report. JA Clin Rep. 2022;8:52.
5. Shoja MM, Lopez ON, Okereke I. Acute thyroid storm following thymectomy: a surprising result of undiagnosed Graves’ disease. Cureus. 2018;10:e3239.
6. Fitzgerald PA. Hyperthyroidism (thyrotoxicosis). In: Papadakis MA, McPhee SJ, Rabow MW, McQuaid KR, eds. Current Medical Diagnosis & Treatment 2023. 62nd ed. New York: McGraw Hill; 2023; p2609.
7. Sarlis NJ, Gourgiotis L. Thyroid emergencies. Rev Endocr Metab Disord. 2003;4:129-136.
8. Ortiga-Carvalho TM, Chiamolera MI, Pazos-Moura CC, et al. Hypothalamus-pituitary-thyroid axis. Compr Physiol. 2016;6:1387-1428.
9. Akamizu T. Thyroid storm: a Japanese perspective. Thyroid. 2018;28(1):32-40.
10. Galindo RJ, Hurtado CR, Pasquel FJ, et al. National trends in incidence, mortality, and clinical outcomes of patients hospitalized for thyrotoxicosis with and without thyroid storm in the United States, 2004-2013. Thyroid. 2019;29:36-43.
11. Basida B, Zalavadiya N, Ismail R, et al. Weathering the storm: thyroid storm precipitated by radioiodine contrast in metastatic thyroid carcinoma. Cureus. 2021;13:e14219.
12. Laliberte BD, Goldenberg E, Reece-Stremtan SJ. Intraoperative diagnosis and treatment of thyroid storm in a 15-year-old male. A A Case Rep. 2014;3:107-109.
13. Satoh T, Isozaki O, Suzuki A, et al. 2016 Guidelines for the management of thyroid storm from the Japan Thyroid Association and Japan Endocrine Society (First edition). Endocr J. 2016;63:1025-1064.
14. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26:1343-1421.
15. Terefe M, Belay BY, BY, Addisu NY, et al. Perioperative management of the thyrotoxic patients: a systematic review. Ann Med Surg. 2022;81:104487.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/