Obstetrics Anaesthesia

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Magnesium used in the treatment of pre-eclampsia
a. Crosses the placenta and can result in fetal hypotonia
b. Potentiates non-depolarising neuromuscular blockers
c. Is completely eliminated in urine
d. Causes uterine stimulation
e. May be antagonized by IV calcium - Which of the following statements regarding the features of pre-eclampsia are true?
a. The incidence is approximately 2-3% in the UK population
b. Only diastolic pressure is important
c. Proteinuria is a recognized feature
d. Usually occurs 20 weeks post gestation
e. Abnormal liver function occurs in 15% of patients with preeclampsia - Regarding antihypertensive management in pre-eclampsia
a. Angiotensin converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) are fetotoxic
b. Antihypertensive treatment during pregnancy may include methyldopa
c. The first line antihypertensive post partum is methyldopa
d. Β-blockers play an important role in the management of intrapartum hypertension
e. Nifedipine is safe at any gestation - The following drugs are generally avoided in the management of hypertension during pregnancy
a. Atenolol
b. ACE inhibitors
c. ARBs
d. Hydralazine
e. Doxazosin - The following are symptoms or signs of magnesium toxicity
a. Loss of patellar reflex
b. Flushing
c. Double vision
d. Slurred speech
e. Cardiac arrest
INTRODUCTION
Hypertensive disorders of pregnancy are one of the most common obstetric medical problems and are associated with a high maternal and fetal morbidity. Maternal deaths from preeclampsia and eclampsia are on the rise and according to the UK Confidential Enquiry into Maternal Deaths, the mortality rate for 2006 – 2008 triennium was 0.83 per 100 000 maternities (22 deaths) compared with 0.66 (15 deaths) in the triennium 2003 – 2005.1 Cerebral haemorrhage remains the commonest cause of death in this group and hence rapid and effective treatment of hypertension to prevent haemorrhagic stroke is highlighted in this report.
As aetiology is largely unknown, preventative measures and screening tools are lacking and management is directed at the control of clinical manifestations. Delivery remains the only definitive treatment.
HISTORY
Ancient Greeks believed that preeclampsia was caused by the imbalance of the body fluids (blood, phlegm, yellow and black bile). Symptoms of the disease were later thought to be due to woman’s extremely porous skin and also the ‘wandering womb’, where the uterus wandered in the body and caused havoc upon the liver, spleen, brain and lungs. Early treatment was aimed at blood-letting and treating the woman to a warm bath in a calm and dark environment. However, from an early time the importance of hastening delivery was recognised.
PATHOPHYSIOLOGY
Much progress was made in understanding the pathophysiology of hypertensive disorders of pregnancy in the 20th century when poor invasion of the placental trophoblast cells of the maternal spiral arteries was identified as a major component of the disorder. This results in small muscular high resistance vessels instead of large low resistance vessels, leading to limited distensibility of spiral arteries restricting blood flow to the placenta and fetus. (Figure 1)
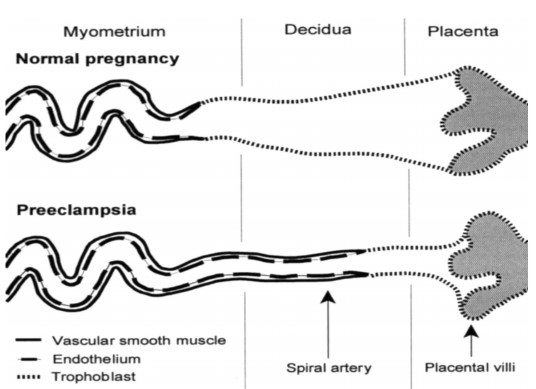
Figure 1. Spiral artery invasion by trophoblasts in normal and pre-eclamptic placenta. Reproduced with permission from Oxford University Press
PATHOGENESIS
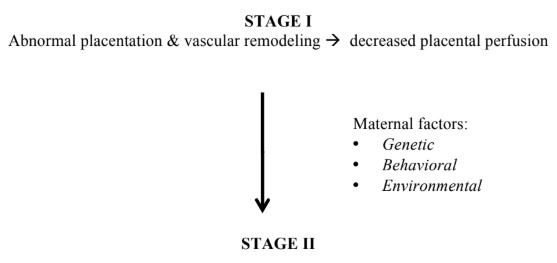
A two-stage process of pathogenesis has been described. Abnormal placentation along with endothelial dysfunction gives rise to the spectrum of the disease..
Maternal Syndrome of pre-eclampsia with endothelial dysfunction
The maternal syndrome of preeclampsia is characterised by decreased perfusion due to vasospasm and activation of coagulation cascade with microthrombi formation and end organ damage.2
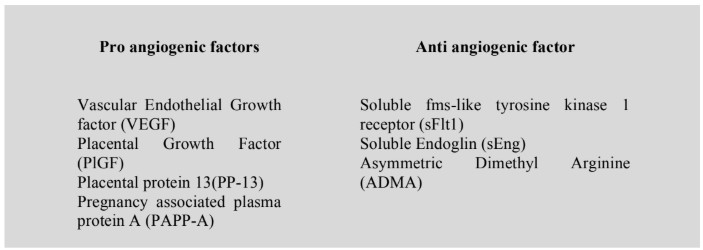
Resulting endothelial dysfunction produces an imbalance of pro and anti-angiogenic factors, with an increase in anti-angiogenic factors. It should be noted that these biomarkers do not have sufficiently high positive predictive value when used alone.3
DEFINITIONS AND TERMINOLOGY
Normally pregnancy causes a fall in mean arterial blood pressure (MAP) and systemic vascular resistance (SVR) in the first half of pregnancy as a result of vascular smooth muscle relaxationsecondary to progesterone. There is a gradual increase of MAP from 24 weeks until term when pre- pregnancy levels are reached.
The cardiovascular changes during pregnancy with relation to heart rate, cardiac output and stroke volume are shown in figure 2.
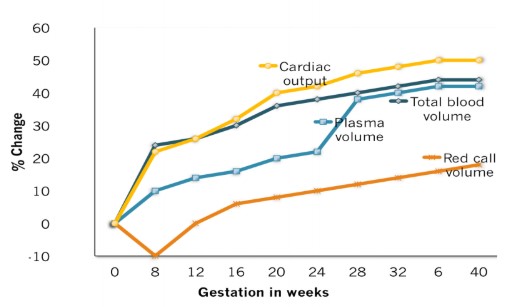
Figure 2. A graphical representation of normal cardiovascular changes in pregnancy.
Hypertensive disorders of pregnancy embrace a variety of definitions as shown below.4
Chronic Hypertension
Hypertension present at the time of pregnancy booking (before 20 weeks of gestation) or if the woman is already on antihypertensive treatment.
The physiological decrease in blood pressure in early pregnancy can mask the diagnosis of this condition and it may be apparent only in the post-partum period when the blood pressure fails to normalise. This condition complicates 3-5% of pregnancies and doubles the risk of preeclampsia.
Gestational Hypertension (Pregnancy Induced Hypertension)
New hypertension presenting after 20 weeks gestation without significant proteinuria* which usually resolves within 6 weeks of delivery.
It occurs in 6-7% of pregnancies and 15-25% of these women proceed to develop pre-eclampsia. It tends to recur in subsequent pregnancies.
Pre-eclampsia
New hypertension presenting after 20 weeks of gestation with significant proteinuria*. This condition complicates 5-6% of pregnancies and is responsible for an estimated 50000 deaths worldwide annually.
*Significant proteinuria – Urine protein creatinine ratio (PCR) > 30 mg/mmol (or) a total protein excretion ≥ 300 mg per 24 hr collection of urine (or) 2 specimens of urine collected ≥ 4 h apart with ≥2+ on the protein reagent strip.
Severe pre-eclampsia
Pre-eclampsia with severe hypertension (Table 1) with or without symptoms and associated biochemical and haematological impairment (Table 2).
The classical triad of hypertension, proteinuria and oedema in the diagnosis of pre-eclampsia is no longer used.
Eclampsia
Convulsive condition associated with pre-eclampsia.
In the UK, eclampsia occurs in 1-2% of pre-eclamptic pregnancies.
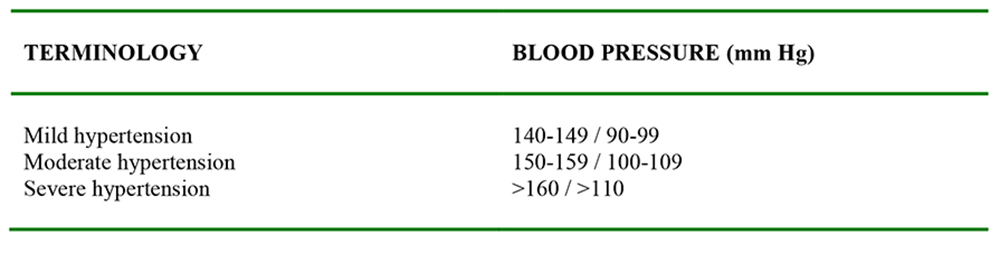
Table 1. Grades of hypertension according to severity.4
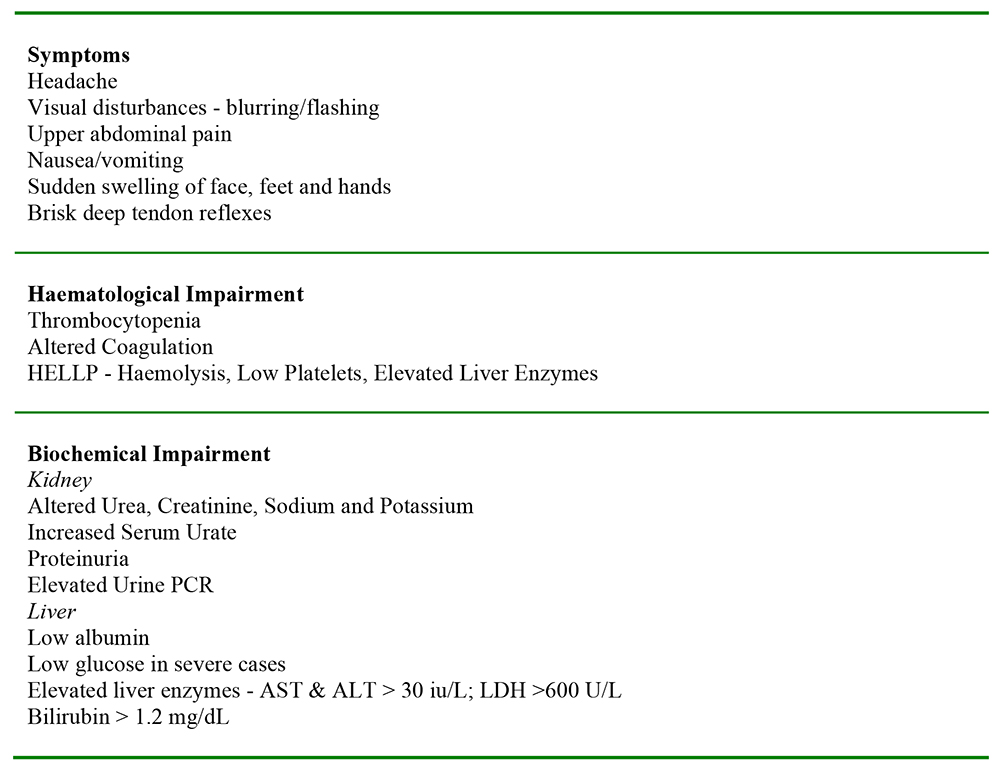
Table 2. Symptoms and Associated System Involvement in Severe Pre-Eclampsia
RISK FACTORS
The factors associated with the development of pre-eclampsia are classified in Table 3.4
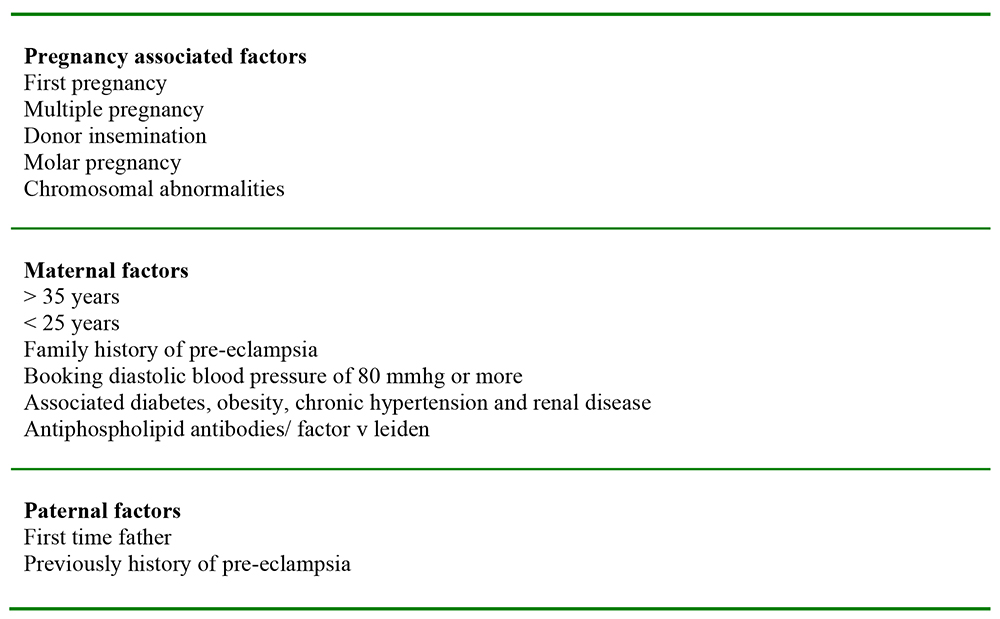
Table 3. Risk Factors
COMPLICATIONS
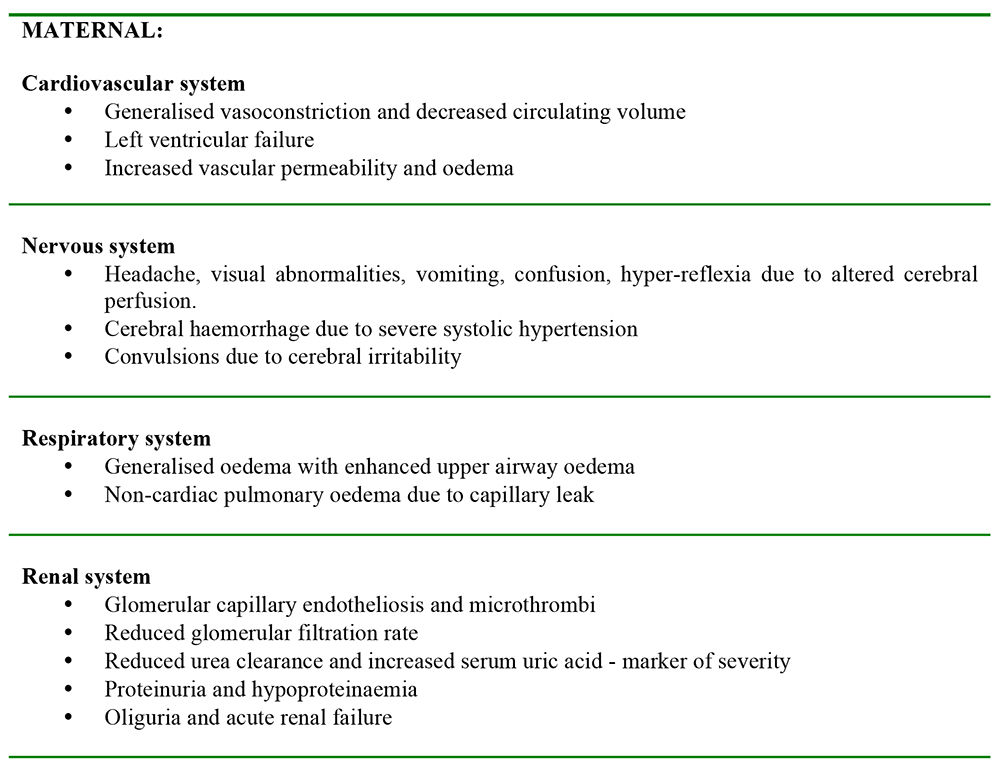
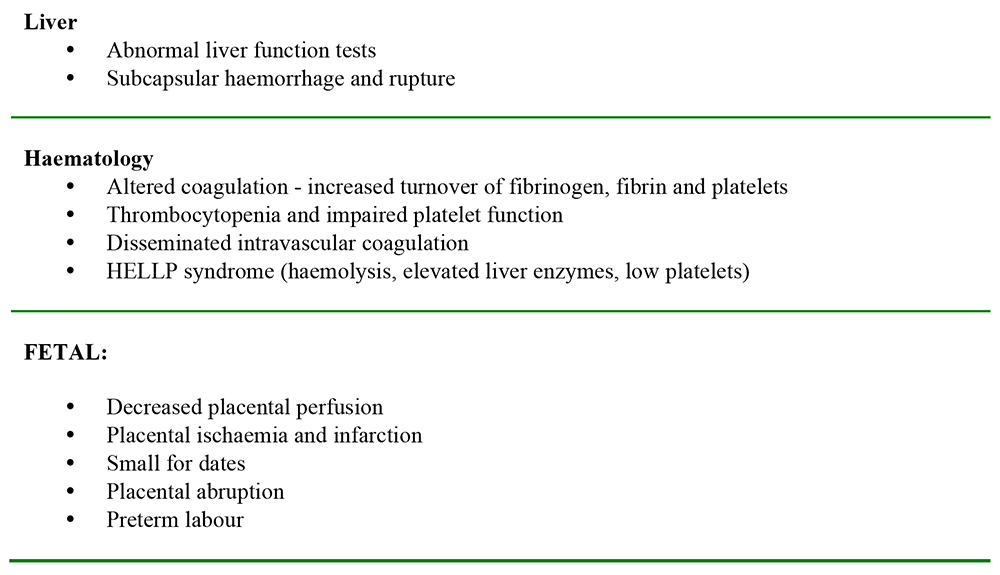
Table 4. Maternal & Fetal Complications
Preeclampsia as a Predictor of Future Cardiovascular Complications for Mother and Child
Offspring of pre-eclamptic mothers have been found to have an elevated risk of haemorrhagic or thrombotic stroke when compared to cardiovascular events, suggesting that pre-eclampsia is more closely related to blood vessel dysfunction in the brain than the heart.6
Preeclampsia is a risk factor for later cardiovascular disease in women. It has been shown to double the risk of ischaemic heart disease, stroke and venous thromboembolic events in the five to fifteen years following a pre-eclamptic pregnancy. It is notable that both pre-eclampsia and ischaemic heart disease are associated with dyslipidaemia, insulin resistance, and endothelial dysfunction.7
INVESTIGATIONS
Useful blood tests in preeclampsia include:
- Full blood count – with special emphasis on platelet count. Clotting screen is generally only required if platelets <100 × 10-9/L, liver function test (LFT) is abnormal or unexplained bleeding or bruising is present. Request a blood film if HELLP suspected.
- Urea & electrolytes – serum creatinine, serum urate.
- Liver function test – serum transaminases (AST or ALT). Check glucose if ALT >150, acute fatty liver of pregnancy or diabetic.
Use pregnancy-specific range, as there is a marked variation in the normal values during pregnancy and at different gestational periods.
Urine tests in pre-eclampsia include:
- Urine dipstick.
- Urinary protein creatinine ratio (PCR) from a random sample (< 30 mg/mmol excludes significant proteinuria; > 30 mg/mmol does not reliably confirm or quantify proteinuria).
- 24-hour urine collection (≥300 mg/24 hr both confirms and quantifies proteinuria).
- Midstream specimen of urine – to exclude infection.
- Urine output must be accurately monitored and recorded.
Further investigations are warranted according to clinical presentation.
MANAGEMENT
The management of patients with hypertensive disorders of pregnancy can be grouped into the following headings.
Pre-conception care
As the risks of pre-eclampsia and gestational hypertension are increased with raised BMI, weight loss should be encouraged in overweight women prior to conception.
Women with chronic hypertension should be assessed to exclude any secondary causes of hypertension, ensure optimal hypertensive control, discuss the increased risks of pre-eclampsia, and educate the need for drug alterations including withdrawal of angiotensin converting enzyme inhibitors (ACE inhibitors) and angiotensin receptor blockers (ARBs), due to the fetotoxic effects of these drugs. Women with previous poor obstetric outcomes because of severe pre-eclampsia should be counselled and offered prophylactic treatment with low dose aspirin.8
Due to the hypothesis that pre-eclampsia involves endothelial dysfunction and oxidative stress, supplementation with antioxidants Vitamin C and E is thought to improve the biochemical markers of endothelial activation. A multicentre trial of 10 000 nulliparous women showed that supplementation did not materially affect either maternal or perinatal outcomes.9
General antenatal care
Maternal
Pregnant women with hypertension require closer antenatal surveillance to aid early identification of pre-eclampsia with regular blood pressure measurement, blood and urine analysis. These women should have an early referral to an obstetric anaesthetic clinic. Not only are they at increased risk of obstetric intervention requiring anaesthetic input but also management of the condition itself may include regional blockade and this should be discussed in the antenatal period.
Admit all pregnant women with pre-eclampsia or gestational hypertension with severe hypertension (>160/110 mmHg) irrespective of gestation.
Fetal
Fetal monitoring in the form of fetal growth and biophysical profile with ultrasound scans to detect IUGR, amniotic fluid volume and umbilical artery doppler velocimetry should be performed every 4 weeks after 24-26 weeks’ gestation in women at high risk of pre-eclampsia. Abnormal umbilical artery Doppler thresholds include umbilical artery pulsatility index > 2 standard deviations and absent or reversed end diastolic flow.
Control of hypertension
Treatment of hypertension should be initiated to reduce the risk of maternal intracranial haemorrhage. Oral labetalol and methyldopa are the recommended first-line agents when the systolic blood pressure reaches 150-160 mmHg. If there is severe pre-eclampsia (with very high systolic pressures), treatment can be with either oral or intravenous labetalol, oral nifedipine, intravenous hydralazine or a combination of drugs to maintain a MAP of <125 mmHg. Overzealous hypertensive treatment may cause fetal compromise due to poor placental perfusion.10
Drugs
All antihypertensive drugs are assumed to cross the placenta and enter the fetal circulation. Most of the drugs commonly used have not been found to be teratogenic, although ACE inhibitors and ARBs are fetotoxic. The use of these drugs may result in IUGR, oligohydramnios, joint contractures, pulmonary hypoplasia, renal tubular dysplasia, neonatal anuric renal failure and hypocalvaria in the fetus. The mainstay of treating hypertension in pregnancy is to protect the woman from dangerously high blood pressure and to permit maximum fetal maturity by continuing pregnancy.5
Common drugs used in the management of hypertensive disorders of pregnancy and their side effects are summarised in Table 5.11
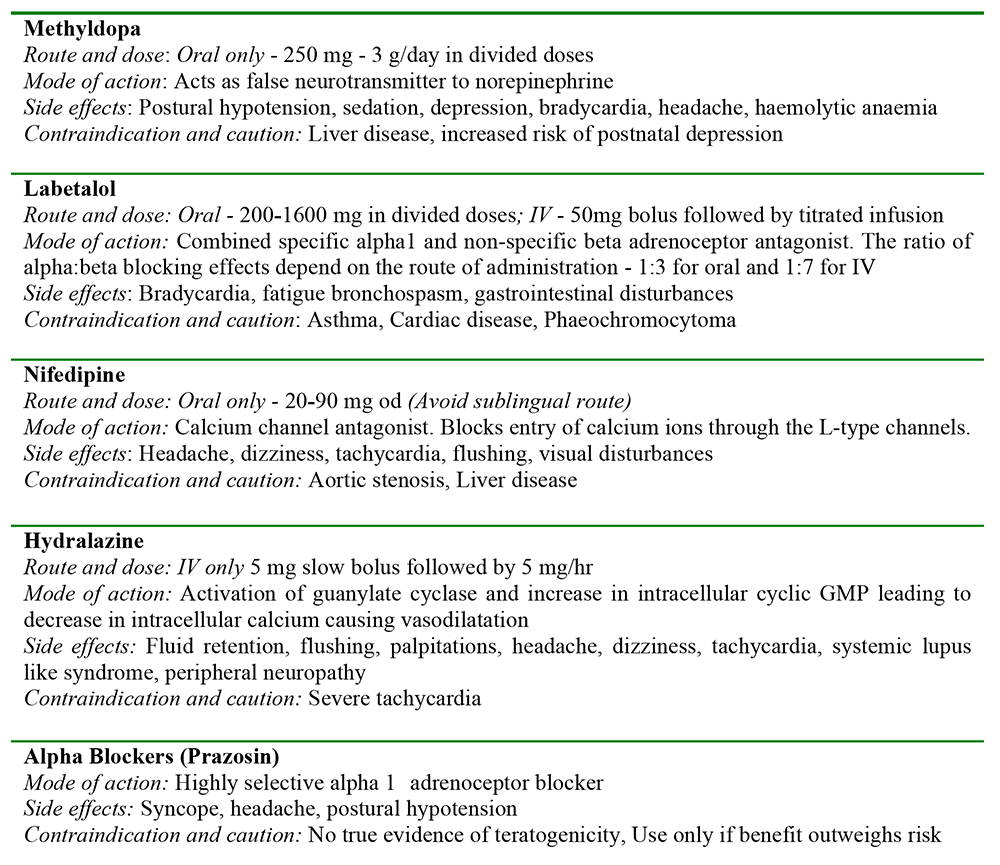
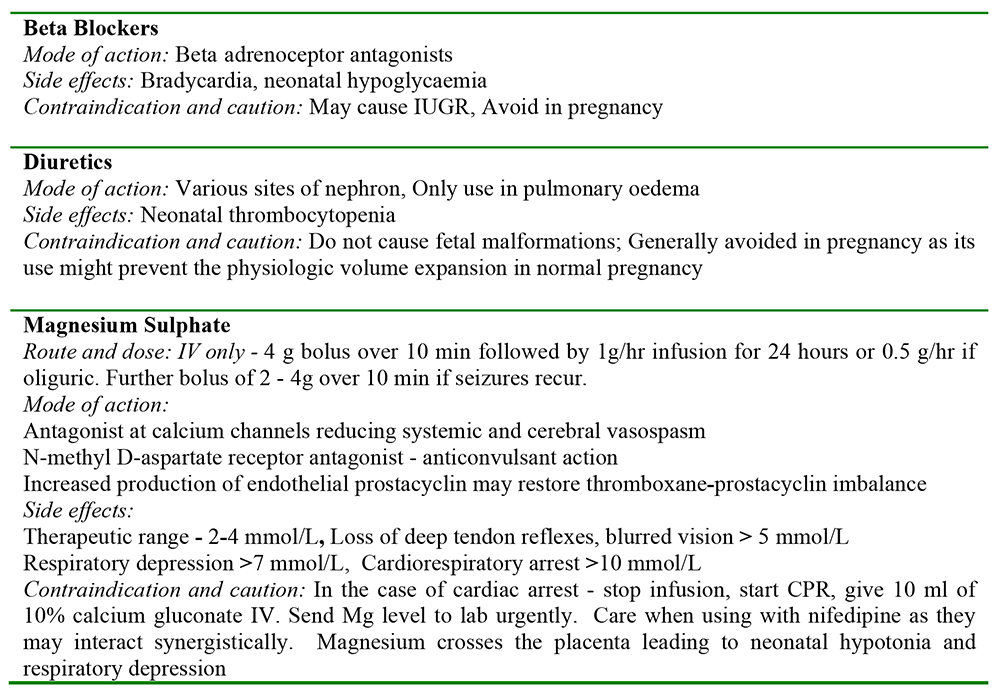
Table 5. Drugs used in the management of hypertension in pregnancy.
Prevention and control of seizures
Eclamptic seizures complicate 1-2% of pre-eclamptic pregnancies. Although uncommon, eclampsia is a debilitating condition that requires clear management guidelines to enable prompt and effective treatment. Rehearsal of its management using multidisciplinary simulation training or teaching drills may aid timely management.
Magnesium sulphate is now the drug of choice for reducing the risk of seizures in severe pre- eclampsia, controlling new onset seizures and reducing the risk of their recurrence. The vasodilator property of magnesium is thought to revert the cerebral vasospasm and increase cerebral blood flow, thus preventing convulsions.12
The dose of magnesium sulphate is derived from the Collaborative Eclampsia Trial regimen – 4g bolus over 10 min followed by 1g/hr infusion until 24 hours after delivery. This maintenance dose is stopped or decreased to 0.5g/hr if the patient is oliguric or if the serum magnesium levels are higher than the therapeutic range. In the event of recurrent seizures, a further bolus of 2-4g over 10 min is given.13
If further seizures occur despite the above, inform the Intensive Care Unit as additional seizure treatment may be required necessitating airway support and ventilation. 44% of eclamptic fits occur after delivery thus, post-natal vigilance is essential, although the disease will resolve spontaneously in all but a few cases.
Fluid management
Pre-eclampsia causes a contracted vascular system with increased capillary permeability. This influences fluid management in two main ways. Due to the generalised vasoconstriction, there may be a sudden drop in blood pressure following administration of certain antihypertensive agents. This may occur following hydralazine treatment and a fluid preload has been recommended. Secondly, due to increased capillary permeability there is a higher predisposition to pulmonary oedema. Studies and case reports have shown an extremely low incidence of permanent renal dysfunction though transient renal derangement is relatively common.
Fluid overload poses a much greater threat in this condition and hence it is common and safer to err on the side of less fluid intake. Invasive monitoring (invasive blood pressure and central venous pressure) may be indicated if there is uncertainty regarding fluid status and in severe cases where intensive care admission is planned. However, the benefits of central venous pressure monitoring in this group of patients remain unclear.
Maintenance fluid intake (including all IV infusions) should not exceed 1 ml/kg/hr. Urine output of 0.5 ml/kg/hr (2 mls/kg over 4 hours) is an accepted minimum. Fluid challenges to maintain this output should be given cautiously.
Labour analgesia
Epidural blockade is the preferred method of labour analgesia. It may obtund the sympathetic response to labour pain and thus limit blood pressure increases during labour. Severe pre-eclampsia is not a contraindication to epidural analgesia but should be avoided if there is a low and/or rapidly falling platelet count. Recommendations as to what is an acceptable platelet count for neuraxial blockade vary. In general, neuraxial blockade is likely to be safe at platelet counts greater than 100 x 10-9/L and is generally not recommended below platelet counts of 50 x 10-9/L. However individual maternal risk factors and local resource issues are important when deciding on the most appropriate method of providing analgesia.
In women with contraindications to regional blockade, analgesia should be provided by alternative means, such as patient controlled intravenous opioid analgesia.
Delivery management
Time and mode of delivery is dependent on the severity of the condition and the gestation of the fetus. In women <34 weeks gestation, unless the woman is very sick, measures should be aimed at stabilising and gaining time to obtain the maximum possible fetal lung maturity. The decision to deliver depends largely on maternal rather than fetal wellbeing as delivery improves the maternal disease.
Anaesthetic considerations for caesarean delivery
The choice of anaesthetic technique for caesarean delivery depends to a large extent on individual circumstances, though a regional technique is preferable in most cases.
A large multicentre trial showed that in severe pre-eclampsia, haemodynamic stability following a spinal anaesthetic was comparable to epidural blockade.14
Subarachnoid anaesthesia – In woman without an epidural in-situ, spinal or combined spinal-epidural anaesthesia is the technique of choice for caesarean delivery. When compared to general anaesthesia, advantages include better haemodynamic stability and avoidance of the complications associated with general anaesthesia (see below). Following spinal anaesthesia, women with pre-eclampsia may experience less hypotensive episodes and have lower vasoconstrictor requirements than those who do not have the condition.15 In addition, the response to the administration of vasopressor agents may be exaggerated and their administration should be carefully titrated.
Epidural analgesia – women with high blood pressure should be advised to have regional analgesia for labour, unless contraindicated, as it helps to control the hypertensive response to pain and may also improve placental blood flow in these patients. Epidural anaesthesia usually provides stable cardiovascular parameters and an effective ‘labour’ epidural may safely be extended for caesarean delivery. Both epidural and spinal anaesthesia are suitable for caesarean delivery but if the platelets are low or falling, a single shot spinal anaesthesia may be more appropriate because it may be associated with less risk of vertebral canal haematoma compared with an epidural.16
General anaesthesia – Intubation may be more difficult due to oedema of the upper airways and decreased pulmonary compliance may impair ventilation.
Indications for general anaesthesia:
- Contraindication to regional blockade e.g. low platelets, coagulopathy
- Post-ictal patient with obtunded level of consciousness or in patient with recurrent seizures
- Presence of pulmonary oedema associated with hypoxia
- Patient refusal of a regional anaesthetic technique
The pressor response to laryngoscopy can lead to a dangerously high surge in blood pressure that may lead to intracranial haemorrhage. It is essential that measures to attenuate this response are undertaken prior to induction and extubation. Magnesium (0.5-1g bolus), labetalol (25-50mg bolus), and potent parenteral opioids (e.g. alfentanil 1-2mg bolus) have all been successfully used.
Antacid and antiemetic premedication (ranitidine and metoclopramide) should be administered prior to caesarean delivery and antihypertensive and anticonvulsive drugs should be continued perioperatively. If the woman has received magnesium sulphate, muscle relaxation must be carefully monitored since magnesium may prolong the action of neuromuscular blocking agents. The routine use of ergometrine and syntometrine is avoided due to their hypertensive propensity and syntocinon is advised. Non-steroidal anti-inflammatory drugs should be withheld due to potential adverse effects on renal and platelet function. Paracetamol may need to be withheld if there is laboratory evidence of significant liver dysfunction.
Recovery
While many women will recover rapidly following delivery, close observation and monitoring is imperative since some may deteriorate and there is a risk of post-partum seizures in up to 44% of women with severe pre-eclampsia. Post-operative care should be provided on a maternity high dependency unit or intensive care unit as indicated. Careful attention to fluid balance, antihypertensive therapy and blood and biochemical status should be maintained. Magnesium sulphate is typically continued for 24 hours following delivery.
Post-partum review
Women with hypertensive disorders of pregnancy should be followed up. Antihypertensive medication may need stopping, changing or reducing in dose. Post-partum antihypertensive treatment may be required for 2-6 weeks after which it may be weaned off with careful review.
Women who experience hypertension in their first pregnancy are at increased recurrence risk of 19% for gestational hypertension, 32% for pre-eclampsia, and 46% for pre-eclampsia superimposed on pre- existing chronic hypertension.17
ANSWERS TO QUESTIONS
- TTFFT. 95% of magnesium filtered in urine is reabsorbed. The intestines also play a role in its excretion. Magnesium acts like a calcium-antagonist, and hence its toxicity is treated by intravenous calcium.
- TFTTF. Proteinuria is a feature, but oedema is not. The condition is called chronic hypertension if present before 20 weeks of pregnancy. The incidence of HELLP is low.
- TTFFT. ACE inhibitors and ARBs cause fetal renal agenesis. Postpartum use of methyl dopa is avoided as it causes post-natal depression. Beta blockers are also avoided due to the risk of IUGR
- TTTFF. As before
- TTTTT. See table 4.
REFERENCES and FURTHER READING
- Centre for Maternal and Child Enquiries (CMACE). Saving Mother’s Lives: reviewing maternal deaths to make motherhood safer: 2006-2008. The Eighth Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG 2011; 118: (Suppl.1): 1-203
- Bell MJ. A historical overview of preeclampsia-eclampsia. J Obstet Gynecol Neonatal Nurs 2010; 39: 510-518
- Alladin AA, Harrison M. Preeclampsia: Systemic Endothelial Damage Leading to Increased Activation of The Blood Coagulation Cascade. Journal of Biotech Research 2012; 4: 26-43
- The management of hypertensive disorders during pregnancy. NICE clinical guideline 107: August 2010
- Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol 2000; 183: S1 – 22
- Kajantie E et al. Pre-eclampsia is associated with increased risk of stroke in adult offspring: The Helsinki birth cohort study. Stroke 2009; 40: 1176-80
- New cardiovascular disease prevention. American Heart Association. March 2011
- Caritis S, Sibai BM, Hauth J, Lindheimer M, Klebanoff M, Thom E et al. Low-dose aspirin to prevent pre-eclampsia in women at risk. N England J Med 1998; 338: 701–5
- Kent A. Antioxidants and preeclampsia. Rev Obstet Gynecol 2010 Spring; 3920: 72-73
- James PR. Management of hypertension before, during and after pregnancy. Heart 2004; 90: 1499–1504
- Krishnachetty B, Plaat F. The treatment of hypertension in pregnancy. Anaesthesia & Intensive Care Medicine 2011; 12: 116-119
- Altman D, Carroli G, Duley L, Farrell B, Moodley J, Neilson J et al. Do women with preeclampsia, and their babies, benefit from magnesium sulphate? The Magpie trial: a randomised, placebo-controlled trial. Lancet 2002; 359: 1187-90
- The Eclampsia Trial Collaborative Group. Which anticonvulsant for women with eclampsia? Evidence from the Collaborative Eclampsia Trial. Lancet 1995; 345:1455–63
- Visalyaputra S, Rodanant O, Somboonviboon W, Tantivitayatan K, Thienthong S, Saengchote W. Spinal versus epidural anesthesia for cesarean delivery in severe preeclampsia: a prospective, randomised, multicenter study. Anesth Analg 2005; 101: 862-8
- Aya AG, Vialles N, Tanoubi I, Mangin R, Ferrer JM, Robert C et al. Spinal anesthesia-induced hypotension: a risk comparison between patients with severe preeclampsia and healthy women undergoing preterm cesarean delivery. Anesth Analg 2005; 101: 869-75
- O Sullivan G. Considerations when devising a protocol for pre-eclampsia. Acta Medica Lituanica 2012; 19: 115–22
- Zhang J, Troendle JF, Levine RJ. Risks of hypertensive disorders in the second pregnancy. Paediatr Perinat Epidemiol 2001; 15: 226–31
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/