
QUESTIONS
- Regarding rheumatoid arthritis (RA):
a. It only affects bones and connective tissue
b. It mainly affects the axial skeleton
c. It is associated with the HLA-DR4 subtype
d. Over 95% of rheumatoid patients are positive for rheumatoid factor
e. Environmental factors may play a role in it’s aetiopathogenesis - The following features are seen in patients with RA:
a. Dry eyes
b. Obstructive lung disease
c. Anaemia
d. Weight gain
e. Increased susceptibility to infections - The drugs that can be used to treat the symptoms of RA are:
a. Paracetamol
b. Infliximab
c. Indomethacin
d. Prednisolone
e. Ciclosporin
INTRODUCTION
Rheumatoid arthritis (RA) is an autoimmune, chronic systemic inflammatory disorder characterised by deforming symmetrical polyarthritis of varying extent and severity, associated with synovitis of joint and tendon sheaths, loss of articular cartilage and erosion of juxta-articular bone. It is a multi-system disorder that may affect the function of other organ systems.
INCIDENCE
The incidence of rheumatoid arthritis is low, with 1.5 men and 3.6 women developing RA per 10,000 people per year. The prevalence of RA is estimated at between 0.5-1.5% worldwide, but tends to be higher in the Northern European and North American populations. It is three times more common in women than men, and has a peak incidence of onset between 30 and 55 years.
AETIOPATHOGENESIS
The aetiology of RA is still unclear, and is believed to be similar to that of other autoimmune diseases i.e. an abnormal immune response to an infectious agent or a component of the agent, in a genetically susceptible individual. Approximately 70% of cases are associated with the HLA-DR4 subtype, and 80% of patients are sero-positive for rheumatoid factor (compared to 5-10% of the general population). Environmental factors may also play a role, including as yet, unidentified viral or bacterial agents. Other risk factors associated with the development of RA include female gender, a family history of RA, food allergies and intolerances, altered gut flora, psychological stress, exposure to heavy metals and cigarette smoking.
CLINICAL FEATURES
These can be divided into musculoskeletal involvement and effects on other organ systems.
Musculoskeletal
- Patients typically present with persistent, painful joint swelling with morning stiffness. Joint involvement is often symmetrical.
- Commonly affected joints include the wrists, fingers, neck, shoulders, elbows, hips, knees, ankles and feet. The main signs are soft tissue swelling, raised temperature, tenderness on pressure or movement, limitation of movement and later, deformities and nodules.
- The phase of acute inflammation may be preceded by a prodrome of fatigue and generalised weakness. Exacerbations of RA may be associated with fever and lymphadenopathy. They tend to occur in episodes lasting weeks or months, between which patients may be relatively asymptomatic. Repeated exacerbations lead to progressive joint damage and severe disability in 10% of patients.
Axial skeleton involvement
Axial skeleton involvement is common and often asymptomatic. This can have major consequences for airway management and should be looked for in all long term RA patients.
Cervical spine
The atlanto-axial joint is commonly affected in RA because of attenuation of the transverse ligament and erosion of the odontoid peg (also known as the dens). This may cause atlanto-axial instability in about 25% of patients suffering from RA. The risk of instability increases over time, and is greater in patients with severe disease and in those who are seropositive. Acute atlanto-axial subluxation may cause spinal cord compression or compression of the vertebral arteries leading to quadriparesis or sudden death. Patients may be asymptomatic or present with neck or occipital pain and radicular symptoms, which are difficult to differentiate from other rheumatoid complications. Patients who have symptoms suggestive of cervical spine involvement should be referred to a rheumatologist or spinal surgeon to monitor symptoms and radiographic progression of disease and to consider early spinal fixation. There are two main categories of cervical spine instability: subaxial subluxation and atlantoaxial subluxation (AAS).
- Subaxial subluxation: This is uncommon and occurs below C2. It leads to early symptoms of nerve compression.
- Atlanto-axial subluxation (4 subtypes):
- Anterior (affecting up to 80% of patients). The C1 vertebra moves forward on the C2 vertebra as a result of destruction of the transverse ligament. There is then a risk of spinal cord compression by the odontoid peg. A lateral cervical spine X-ray in flexion is useful in diagnosis. Subluxation is diagnosed if the distance between the atlas and the odontoid peg exceeds 4 mm in patients older than 44 yr and 3 mm in younger patients. Anterior atlanto-axial subluxation is worsened by neck flexion. See Figure 1.
- Posterior (affecting about 5% of patients). Destruction of the odontoid peg may cause backward movement of the C1 vertebra on C2, which may be seen on lateral cervical spine X-ray in extension. Posterior atlanto-axial subluxation is worsened by neck extension.
- Vertical (accounts for about 10–20%). Destruction of the lateral mass of C1 can lead to subluxation of the odontoid peg through the foramen magnum and compression of the cervico-medullary junction.
- Lateral or rotatory subluxation results from degenerative changes in the C1/C2 facet joints. It can lead to spinal nerve and vertebral artery compression.
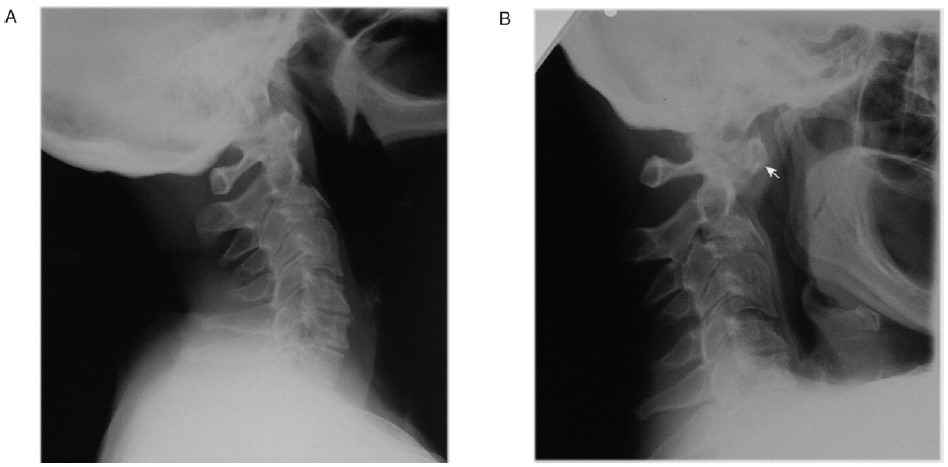
Figure 1. Cervical spine X-rays in a patient with severe rheumatoid arthritis on long term steroids showing anterior atlanto-axial subluxation (with permission from Oxford University Press). A – Neck extension. B – Neck flexion: Demonstrates severe anterior atlanto-axial subluxation. Note the position of odontoid peg axis (arrows). There is a 13 mm dislocation between the odontoid peg and the main body of the axis. C3 shows degenerative changes.
Ankylosis
Ankylosis of the cervical spine may lead to fixed flexion deformity of the neck
Laryngeal involvement:
Involvement of the cricoarytenoid joint may cause dyspnoea, stridor, hoarseness and rarely upper airway obstruction. Laryngeal amyloidosis and rheumatoid nodules may also cause obstruction of the larynx. Assessment is by laryngoscopy combined with computed tomography (CT) imaging. Difficulties have been reported following tracheal extubation, and patients require close observation during recovery for signs of airway obstruction secondary to oedema.
The Temporomandibular joint (TMJ):
The TMJ may be involved causing limitation of mouth opening, which may render direct laryngoscopy impossible.
Organ system involvement
Extra-articular manifestations occur in >50% of patients.
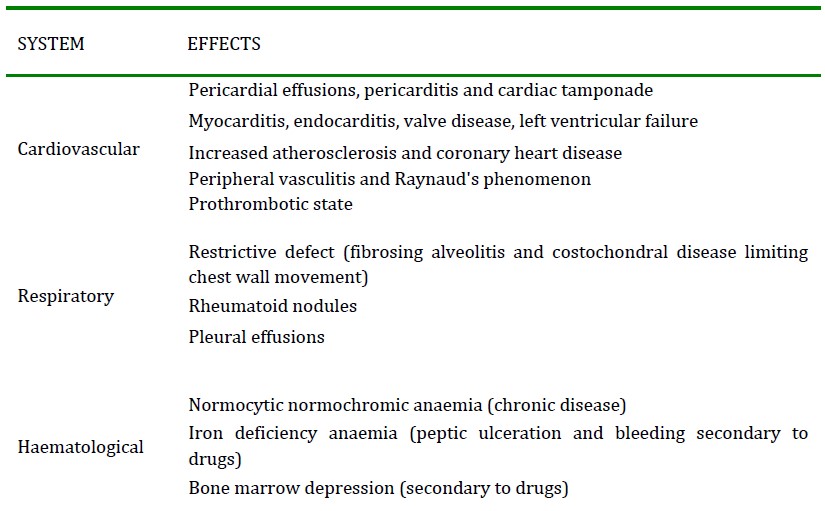
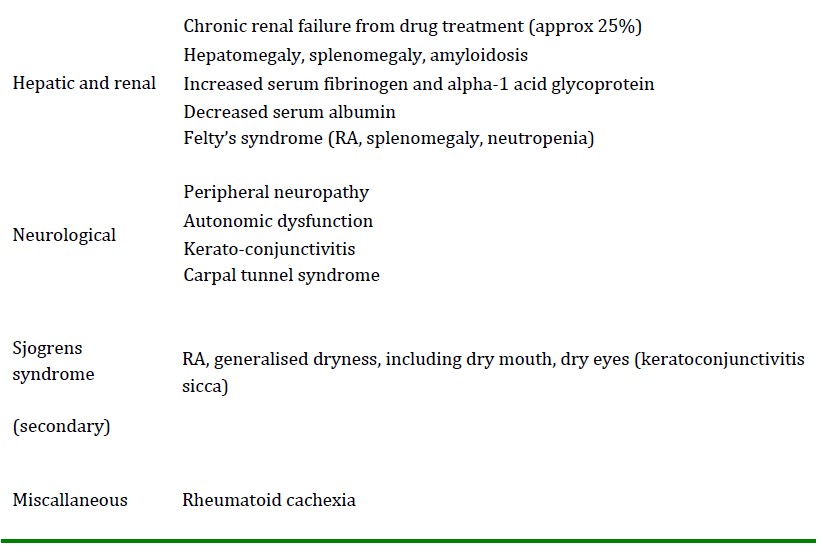
Table 1: Extra-articular involvement in RA
DIAGNOSIS
The diagnosis of RA is mainly clinical, and confirmed with laboratory tests for autoantibodies and elevated inflammatory markers. Plain radiography can demonstrate periarticular soft tissue swelling, joint space narrowing, erosions and osteopenia. Ultrasound and magnetic resonance imaging (MRI) may be used to demonstrate early stages of the disease. New biomarkers such as anti-cyclic citrullinated peptide antibodies (anti-CCP or ACPA) are now being used to diagnose early disease.
MANAGEMENT
The main treatment aims for RA are symptom relief and altering the immune response before the onset of erosions (disease modification), thus preventing disability and maintaining joint function.
Symptom relief
The standard treatments for symptom relief include non selective NSAIDs, COX-2 specific NSAIDs and corticosteroids. Corticosteroids are primarily used to overcome acute flares whilst the patient becomes established on disease-modifying agents.
In addition to acute pain from inflammation, patients with RA may suffer from chronic pain due to immobility, joint destruction, tendon rupture and muscle atrophy. Long-acting opioid preparations are used to control this form of pain.
Disease modification
Disease modifying anti-rheumatic drugs (DMARDs) reduce frequency of exacerbations and prevent long-term disability. There is a proven mortality benefit over uncontrolled disease. Methotrexate remains the first-line treatment for inflammatory arthritis and is very effective in preventing exacerbations and reducing disease activity and improves both quality of life and mortality rates in RA. Current understanding of RA implicates tumour necrosis factor (TNF) α in influencing the behaviour of all the effector cell types involved in the inflammatory cascade in the synovium. Hence the biological anti-TNF α agents are also used for the first-line management of RA. These drugs are effective treatments in reducing erosive damage, disability and improving quality of life scores. Furthermore, they reduce long-term mortality and may induce remission and even reversal of erosive disease. They have been shown to be even more potent if used in combination with methotrexate. These drugs are very expensive.
PROGNOSIS
The course of the disease is varied, with some having mild short-term symptoms, but in most the disease is progressive for life, with remissions and exacerbations. Poor prognostic factors include persistent synovitis, early erosive disease, extra-articular findings (including subcutaneous rheumatoid nodules), positive serum rheumatoid factor, HLA-DR4 alleles, family history of RA, poor functional status, socioeconomic factors, elevated acute phase response (erythrocyte sedimentation rate, Creactive protein), and increased clinical severity.
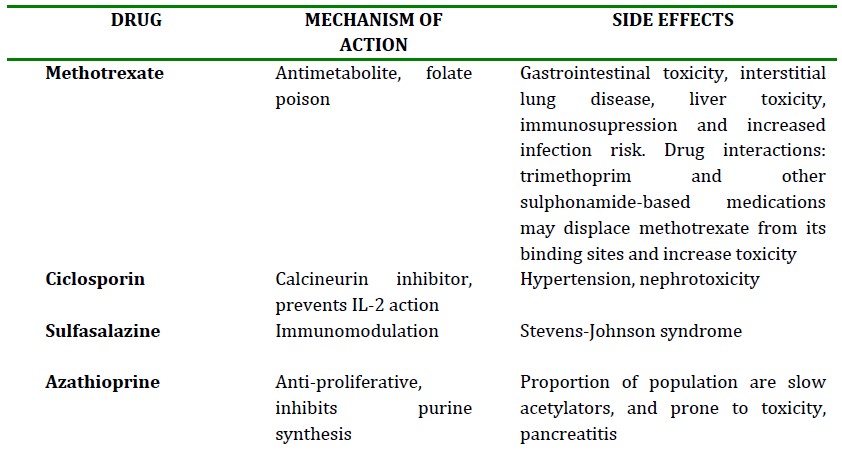
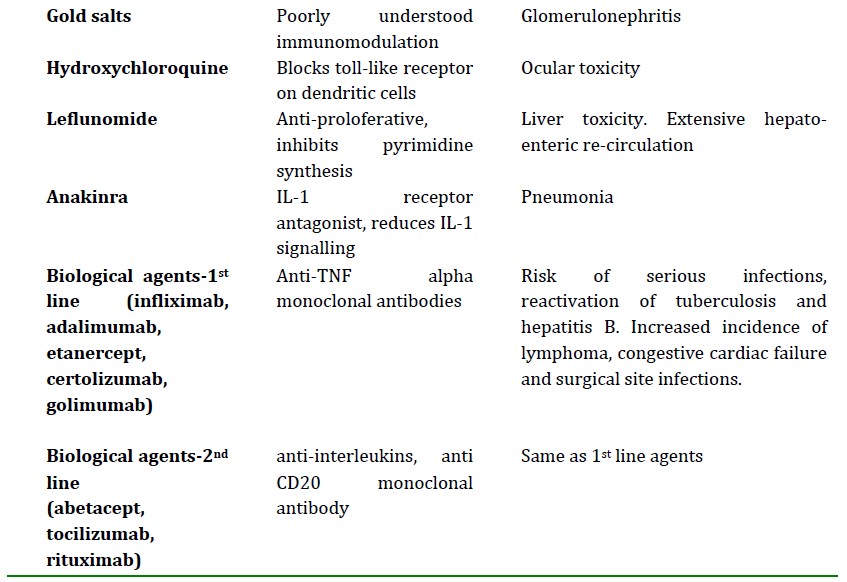
Table 2: Disease modifying agents used in RA
SUMMARY
RA is a multisystem progressive disorder that significantly affects quality of life. Early diagnosis and treatment with DMARDs is key in reducing long term morbidity. Optimal care of patients with RA requires an integrated approach of pharmacologic therapies such as NSAIDs, DMARDs, biological agents, glucocorticoids, and immunomodulators as well as non pharmacologic techniques like physiotherapy, occupational therapy, patient education and counselling.
ANSWERS
Answer 1
FFTFT
RA is a multisystem disorder and is not limited to the bones and connective tissue. Axial skeleton involvement does occur, but more commonly affected joints include the wrists, fingers, neck, shoulders, elbows, hips, knees, ankles and feet. Approximately 70% of cases are associated with the HLA-DR4 subtype, and only 80% of patients are seropositive for rheumatoid factor. Environmental factors may also play a role, including as yet, unidentified viral or bacterial agents.
Answer 2
TFTFT
Long standing RA patients can develop Sjogrens syndrome with dry eyes and mouth. RA causes restrictive (not obstructive) lung disease due to pulmunory fibrosis and costochondral arthritis limiting chest wall movement. Anaemia is common; anaemia of chronic disease (normochromic) and anaemia due to gastric bleeding secondary to drugs (microcytic). RA is associated with rheumatoid cachexia, and weight gain is rare. RA patients have an increased susceptibility to infections as a result of the immunosupressive effects of the drugs used to manage their disease.
Answer 3
TFTTF
The drugs that are useful to treat symptoms of RA are paracetamol, NSAIDs and corticosteroids. The others modify the disease process, prevent exacerbations and long term disability, but do not treat symptoms.
REFERENCES
- Samanta R, Shoukrey K, Griffiths R. Rheumatoid arthritis and anaesthesia. Anaesthesia 2011; 66: 1146–59.
- Fombon FN, Thompson JP. Anaesthesia for the adult patient with rheumatoid arthritis. CEACCP 2006; 6: 235–9.
- Temprano K. Rheumatoid arthritis. Emedicine. Online at http://emedicine.medscape.com/article/331715-overview
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/