General Topics

Imagine you are presented with a patient with a neck tumour causing increasing airway obstruction. Control of the airway is one of the fundamental skills for all anaesthetists, but the range of techniques and equipment you might choose ranges from unsupplemented ketamine to awake fibreoptic intubation. How will you decide which is the right thing to do? Maybe you would like further training. This is the first in a series of airway masterclasses, aimed to help you develop the skills you already have, use the equipment available, and identify and teach other techniques which would help you in the future.
Write down the techniques and equipment actually available to you in your hospital for dealing with the above case. When you have finished, please email your answer back, as your reply will be important in helping us decide on the content of future masterclasses.
Keeping it simple
Airway management should always be done in the most simple and straightforward way possible. Introducing complex techniques when they are not needed brings the risk of added complications.
-
Recognise the problem
Most of the mistakes in airway management arise because of an incorrect assessment of what will happen when the patient is anaesthetised. There are some groups of patients in whom airway difficulties are more common. These are listed at the end of this tutorial, but make your own list now, and compare it with ours:
-
Assess your resources
Do I have the experience, skill and equipment to manage this patient? If not, the correct airway management is to get help before the crisis arises. Discuss the patient with the surgeon, and consider whether there is a more experienced anaesthetist who can help you. Getting such help will strengthen your own ability to cope with a difficult airway in future. If no local help is available, consider whether the patient should be referred to another hospital.
-
Focus on the patient
When you see the patient pre-operatively, they already have an airway which allows them to breathe, even while asleep. Your aim should be to maintain that airway and defend it against the harmful effects of anaesthesia and surgery.
The best protection of the airway is when the patients do it themselves, so ask yourself “Does this patient need to be unconscious, or could we do the case with regional anaesthesia”
A possible regional technique (superficial cervical plexus block) is described in the “Regional Anaesthesia” section of the free educational CD “Anaesthesia Resource 2”.
If you don’t have this CD you can get it free by emailing your request and your mailing address to “Info@talcuk.org”
Take a moment to list the possible advantages and disadvantages of regional anaesthesia in the case of a neck tumour described above. Then turn the page for the expert’s opinion.
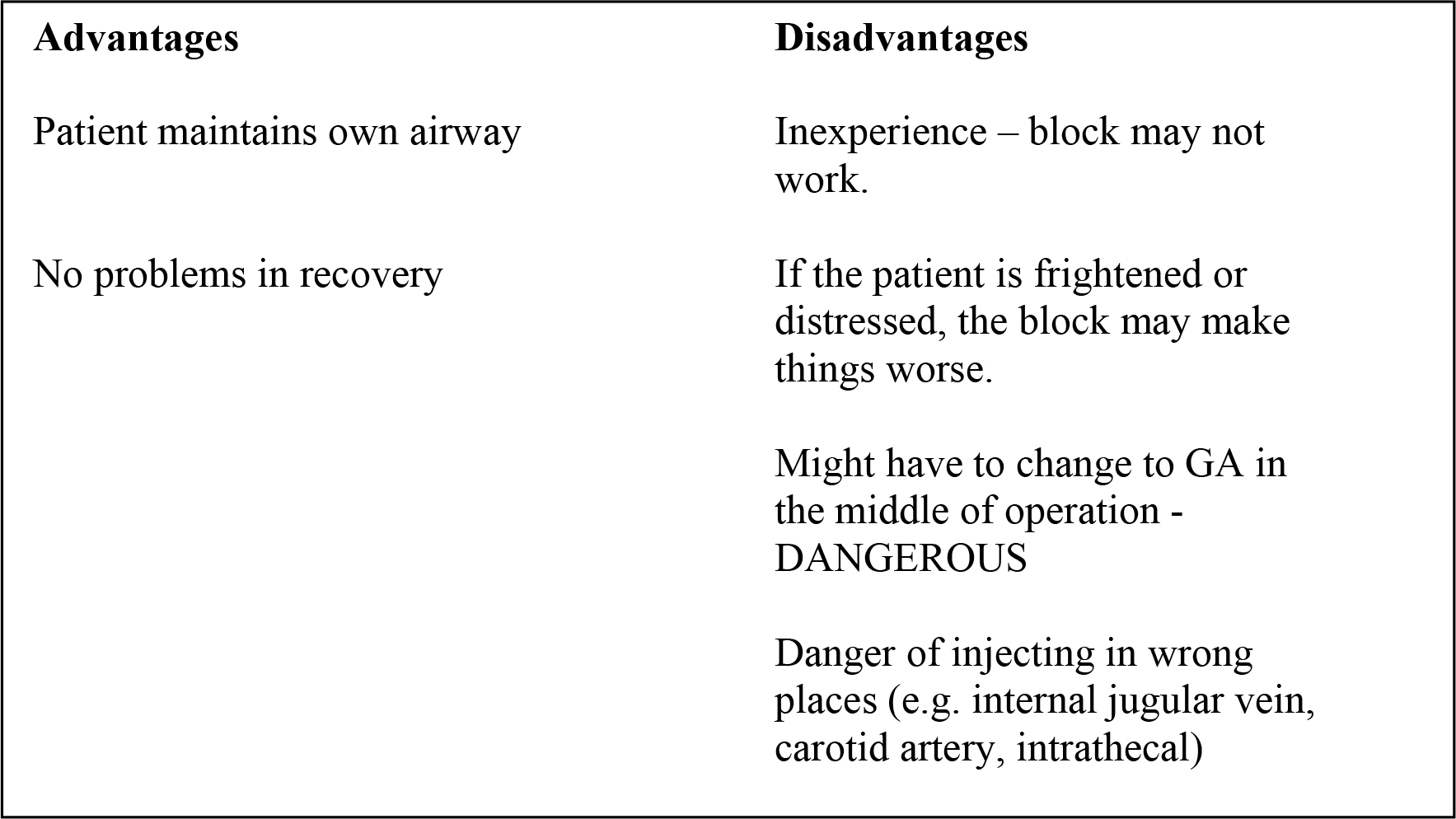
In this case, for most anaesthetists, the disadvantages of using regional anaesthesia would probably be greater than the potential advantages. However, here is a published account of a real case in Uganda, where local anaesthesia was in fact used.
A 30-year-old woman with a large goitre underwent thyroidectomy under local anaesthetic field block. A 1.9 kg goitre was resected. She was given light sedation but was able to communicate throughout the whole procedure which was performed comfortably under the local anaesthesia. She made an uneventful recovery with no complications. Local anaesthetic was chosen as the safest procedure in a remote rural Ugandan hospital which lacked close post-operative monitoring. Other benefits of using local anaesthesia are discussed.
Hodges, Andrew M.1 Tropical Doctor, January 2005, vol. 35, no. 1, pp. 43-43(1)
Suppose instead that a patient with a difficult airway needs a Caesarean section. How would this change your assessment of airway management? If your answer is different this time, you have begun to understand the importance of focussing on the patient and not just on the airway problem!

Strategies for improving your airway skills
Practice airway assessment in your daily work
Always make a conscious assessment of the airway of any patient you are due to anaesthetise and write it down. Then compare your predictions with your experience. Your accuracy will improve with practice; focus on whether the patient is one of the “likely difficult” groups you have identified above, and to this information add the physical examination findings. A later masterclass will focus on identifying difficult airways in advance. No-one gets it right 100% of the time – mostly you will be surprised that patients you thought would be difficult turn out to be easy, but from time to time you will find a patient who you thought would be easy but turns out to be difficult to manage, so you always need a “Plan B” for the unexpected difficulty. When you do find one of these patients, go back to your assessment – did you miss anything out? Did you examine the neck properly? Did you look in the mouth? Everybody makes occasional mistakes – learn from them, and talk about them so that other people can learn from your mistakes, and you can learn from theirs.
Become an “airway spotter” away from work
The world is full of people with potentially difficult airways who fortunately do not need anaesthetics. Look carefully at the face, jaw, neck etc of the people you see every day. When you are on the bus, try to identify the three people you think would give you the most airway trouble if you had to give them an anaesthetic. If someone next to you is snoring, try to work out why that person snores so loudly, while others don’t snore at all.
Aim for a perfect clinical technique
The skills of airway management are in some ways like playing a musical instrument, a combination of dexterity and knowledge. Don’t ever accept “good enough”, but think back on every case “how could I have done it better”.
Let’s take a routine intubation as an example.
Make sure that
- in every case that you have the patient’s head and neck in exactly the ideal position – check by standing at the side of the trolley and looking at the profile of the neck and head
- the table or trolley is at the right height to give you a good view (if you are short, practice intubating while standing on a box or low stool!)
- you use a perfect technique, deliberately inserting the blade in exactly the right place in the mouth, identifying all the landmarks, adjusting your technique to give the best possible view of the larynx, not merely one that shows you well enough where to insert the tube
Practice for difficult cases in routine situations
In some situations it will be essential for you to be able to intubate
- With the patient sitting up
- With the patient in the lateral position
- Without relaxants
- You can also simulate anatomical difficulty deliberately by getting an assistant to press backwards on the thyroid cartilage during laryngoscopy. This will displace the base of the tongue backwards, obscuring the front or possibly al of the larynx to convert a Grade 1 to a grade 2 or 3 view.
Practice these techniques on routine patients (expected normal airway, properly prepared, fasted etc) so that when you need to use them in earnest you are doing something that is already familiar.
Teach your airway skills to others
There is no doubt that when you have to teach something, you find out how well you know it yourself. Always be ready to teach about airways – even lay people with basic skills can be taught to save lives in the community and in the hospital by knowing about the recovery position and simple manoeuvres like chin lift/jaw thrust.
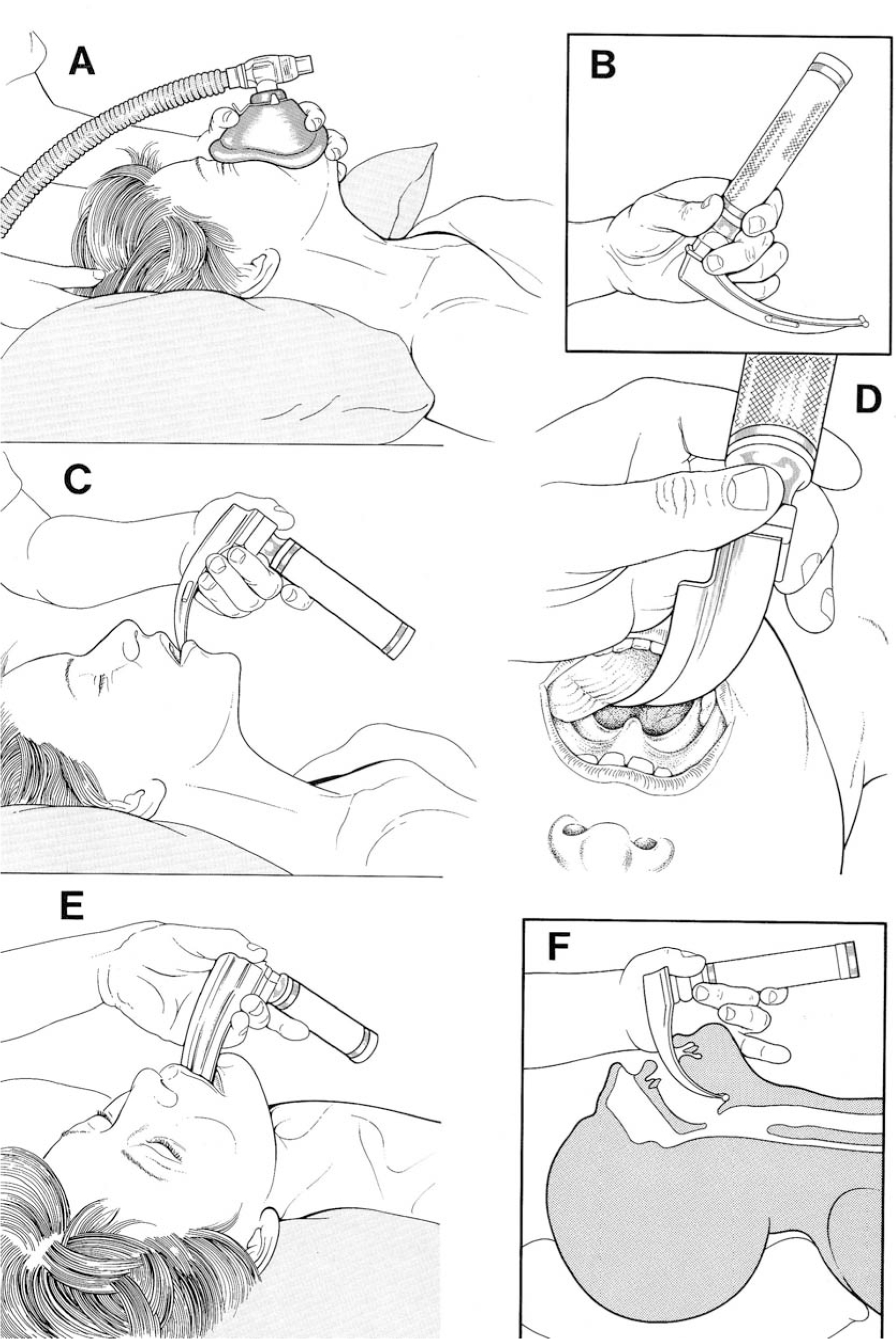
If you are a skilled practitioner, an untrained person watching you intubate will fail to see all the steps that you include in what appears to them to a single smooth action.
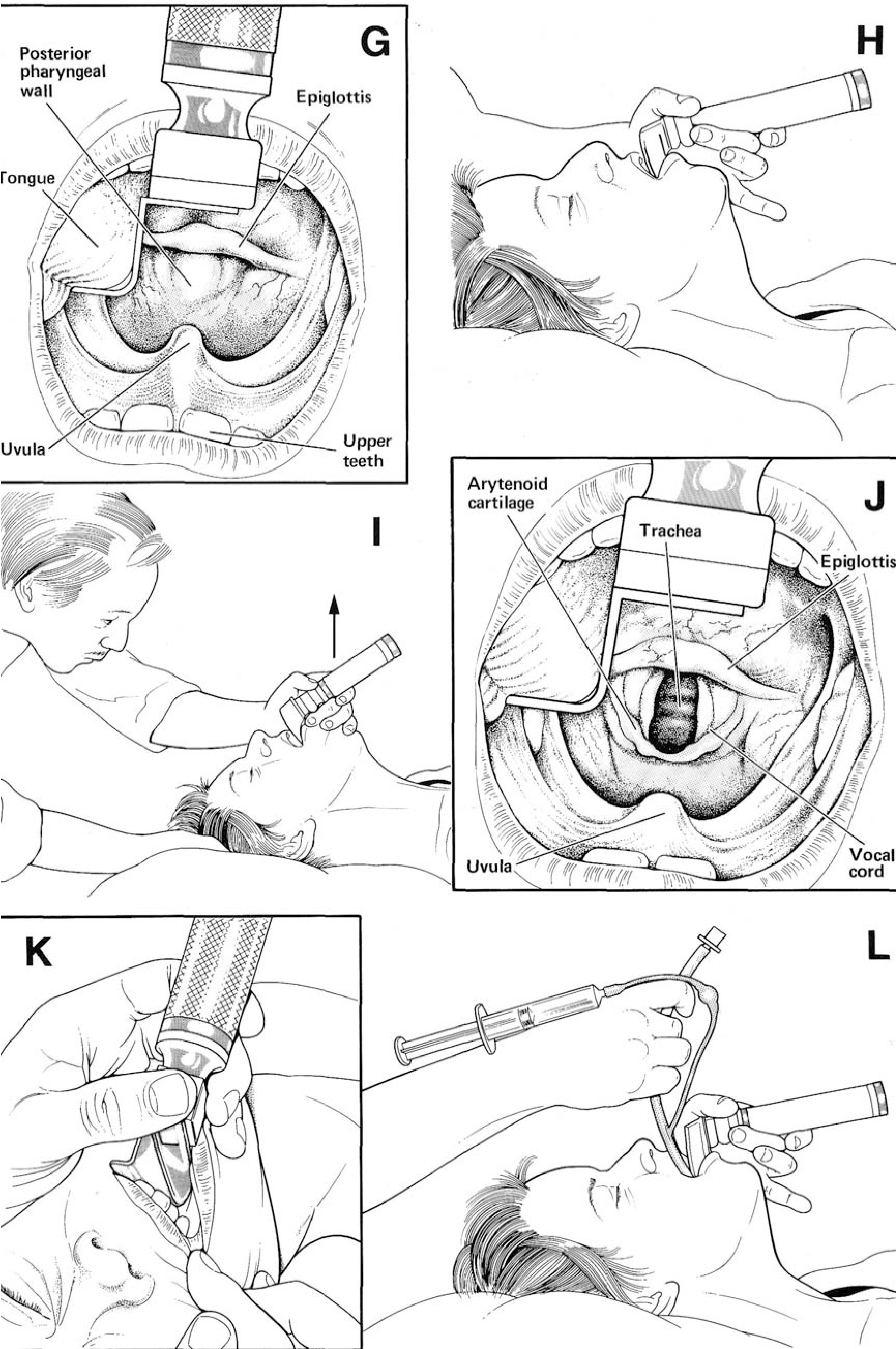
Below is a series of drawings taken from “Anaesthesia at the District Hospital” (a WHO publication also available free on “Anaesthesia Resource 1). In these drawings the process of intubation is “broken down” into a number of steps. Write down a commentary on each of these steps as if you were explaining it to your trainee.
Make your own copy of picture J – even if you are not an artist, when you try to draw something you look at in a deliberate, systematic way that helps you remember.
Practice making this drawing in stages to use as a teaching aid.
A
B
C
D
E
F
G
H
I
J
K
L
Groups of patients where airway difficulties are more common:
- Pregnant women (especially with pre-eclampsia or eclampsia)
- Obese patients
- Small children
- Patients with joint or spinal disease
- Patients with large tongues
- Patients with awkward or gappy teeth
- Patients with tumours of mouth, jaw or neck
Summary of this tutorial
- Airway skills are fundamental, and we all need to continue to work on improving them
- Assessing the airway before anaesthesia is the most important way of minimising difficulty
- Think carefully about what you need to do to ensure airway safety in this patient for procedure.
- Practice all the skills you might need as often as possible, and in controlled circumstances
- Teaching your skills to others saves lives and improves your own performance
Further resources for you to consult:
- “Anaesthesia at the District Hospital” available on order from www.talcuk.org or free on CD-ROM “Anaesthesia Resource 1” – send email to info@talcuk.org
- Useful materials for free download from the Difficult Airway Society http://www.das.uk.com/
- “Update in Anaesthesia” website – www.world-anaesthesia.org –use the search facility to find related articles on “difficult airway”
Please email your completed tutorial, together with any other comments or questions to ……………………………………………………………………………….……..
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/