General Topics

KEYPOINTS
- Revision hip surgery is complex and poses unique challenges to the surgeon and anaesthetist
- Surgery is often prolonged duration with an increased incidence of major haemorrhage and significant post-operative pain
- Communication with surgical colleagues and understanding of the techniques is vital to anaesthetic management
- General anaesthesia with a supplemental regional technique is the anaesthetic of choice for all but the most straightforward of revisions
- Use of goal directed therapy (GDT), invasive monitoring and cell salvage should be considered for all cases
- Patients are at high risk of post-operative complications and care requires increased multidisciplinary team input
INTRODUCTION
Approximately 80,000 total hip replacements (THR) are performed annually in the UK. Increased patient life expectancy and number of primary total hip replacements means the burden of revision surgery is increasing, with around 9000 revision hip replacements taking place across the UK each year.1,2 The surgeon aims to reconstruct either in isolation or both the acetabulum and femur, restoring the patient’s biomechanics with preservation of soft tissue and muscle tension.
Post-operative complications are higher for several reasons. Patients are often elderly with complex co-morbidities. Revision specific factors include increased blood loss, increased risk of dislocation, infection, fracture, significant nerve or vessel injury and intra-pelvic organ injury contribute to post-operative morbidity. In addition, surgical duration is often much longer than the standard 2-3 hours for a primary THR.
These issues create a unique challenge for the anaesthetist, and have a significant impact on the peri-operative management. This tutorial aims to summarise the unique aspects of revision surgery and offer guidance on the anaesthetic management of such cases.
SURGERY
Surgical Indications for Revision Surgery
The indications for the majority of revisions in order of greatest frequency according to the English Joint Registry are aseptic loosening and osteolysis, infection, pain and peri-prosthetic fracture.1
Loosening is a combination of mechanical and biological factors accounting for revision in over 50 % of cases. Shear and tension at the prosthesis bone interface lead to mechanical failure and wear particles activate an inflammatory process stimulating bone reabsorption causing osteolysis. Patients with significant osteolysis are at increased risk of peri-prosthetic fracture, which has the potential for significant blood loss.
Several factors can predispose to infection; patient factors include immunosuppression, diabetes and obesity, intra-operative processes such as long procedure, contamination of instruments, inadequate air filtration and management and lastly, post-operative complications, for instance wound haematoma or superficial infection. Infections can be eradicated if diagnosed early with debridement and washout but after this the bacteria form a protective biofilm resistant to systemic antimicrobials.2
Metal on metal primary THRs were heavily marketed and favored for young patients due to the appeal of their resistance to wear and reduced dislocation rate, with additional evidence of higher levels of post-operative activity.3 Unfortunately these have suffered from unacceptable rates of early revision requirement due to a spectrum of necrotic and inflammatory changes to local tissue. Revision of these implants requires extensive soft tissue debridement with inevitable increase in blood loss and other complications such as dislocation and infection.
Surgical Techniques and Complications
The surgeon’s first aim is to remove the implants that are loose and causing symptoms and to do this with as little bone loss, blood loss or injury as possible. Uncemented acetabular components are removed using special curved osteotomes, which cut bone very close to the shell limiting bone loss. Cemented acetabular components are removed using a combination of osteotomes and extraction devices. If there are breaches in the floor of the acetabulum, care needs to be taken to avoid injuring any intra-pelvic structures and vessels. Cemented femoral components are tackled by first removing cement or bone from the shoulder of the stem then using an extraction device that attaches to the implant.
Infected Hips
Revision for Infection is undertaken in a two-stage process in an attempt to eradicate the infection. The first stage consists of removal of all implants and is concluded with implantation of an antibiotic laden cement spacer. Active infection results in more vascular tissue and increased peri-operative blood loss. The local infection may also lead to significant bacteraemia, and any systemic sign of infection should be a warning sign to the anaesthetist. The second stage occurs once the infection is cleared, and typically happens six to eight weeks following the first stage.
Blood Loss
Blood loss is expected to be significantly higher in revision procedures with the average around one litre, which is double the average for a primary arthroplasty. Risk factors for increased blood loss in revision surgery are male sex, older patients, revision of cemented prosthesis and dual component revision. Additional predictors of reaching a threshold blood loss for intra-operative blood salvage were extended trochanteric osteotomy and higher BMI.4
An extended trochanteric osteotomy refers to the controlled splitting of the femur to facilitate existing prosthesis removal or to improve surgical exposure. Splitting of the femur may also occur accidentally during insertion of new femoral components. This will inevitably lead to a significantly increased blood loss. If the femur is split or requires repair often wires are placed around the bone, which increases the risk of peri-operative neurovascular injury (figure 1).

Figure 1. Hip revision surgery with wire repair
Antibiotic Prophylaxis
As surgery involves the placement of an implant, patients should receive antibiotic prophylaxis on starting anaesthesia. For procedures lasting more than 4 hours, a repeat dose should be used to ensure effective surgical prophylaxis is maintained. Significant blood loss of greater than 1.5L, irrespective of surgical duration, should also prompt the need for re-dosing.
Choice of implants
The surgeon has the choice of using either an uncemented or cemented prosthesis or a combination of both. Uncemented implants undergo impaction to achieve initial stability and have a roughened or porous surface, which allow bone in growth and bone on growth respectively. Stability of the acetabular component can be improved with the addition of screws; however, there is a risk of damage to major vessels (figure 2). If a large calibre intra-pelvic vessel is injured the patient will require a rapid temporary closure, supine repositioning and abdominal approach to these vessels. Very rarely, other pelvic structures may also be at risk of perforation.
Uncemented femoral stems leads to on-going bleeding in the post-operative period as the femoral canal fills with blood as there is no cement to stop this process. This requires careful post-operative management, as blood loss can be significant.
Bone Cement Implantation Syndrome
Cement acts as a grout to hold the prosthesis; it is pressurized into the bone and can lead to the Bone Cement Implantation Syndrome. This is characterized by hypoxia, hypotension or unexpected loss of consciousness and is thought to be due to release of embolic material into the venous blood stream and reaction to the cement monomer causing vasodilatation. Femoral component revision requires reaming of the intramedullary canal as part of their preparation leading to potential for fat embolism or potentiation of the systemic inflammatory reaction syndrome associated with BCIS. [Please read ATOTW 351 Apr 2017 on BCIS]
ANAESTHESIA
Pre-operative Assessment and Optimisation
Pre-operative anaemia is a common problem encountered in the elective surgical patient and is associated with a number of adverse outcomes including increased blood transfusions, prolonged hospital stay and increased cardiorespiratory complications.5,6 It is estimated that approximately 30-35% of hospital transfusions occur for post-operative anaemia, which has significant cost, resource and safety implications. International guidelines on the management pre-operative anaemia published in 2017 serves to streamline the pre-operative process.6 Hip revision surgery, unless being performed for significant infection, is non-urgent surgery and therefore anaemic patients should be postponed for investigation and treatment of their low haemoglobin, with a pre-operative target Hb of >130 g/dL. Patients should be cross-matched for at least 2 units and cell salvage used if appropriate.
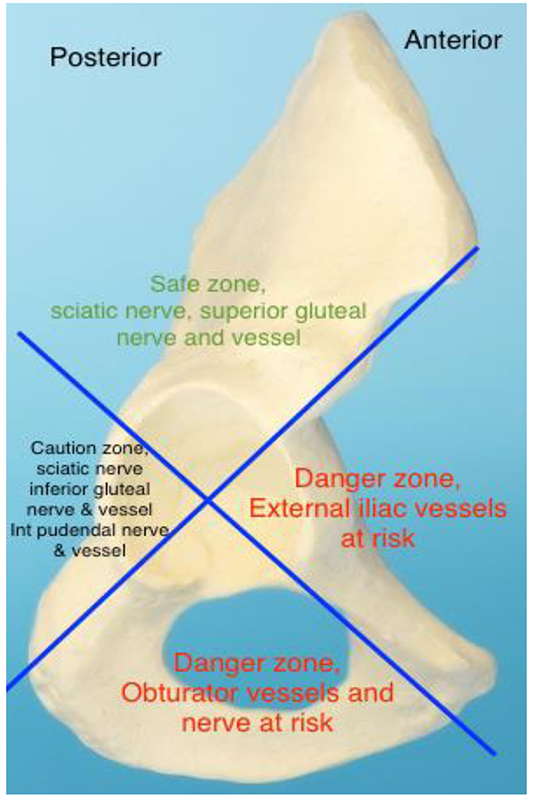
Figure 2. Acetabular Quadrants – Head on view of Right Acetabulum and Underlying Pelvic Structures susceptible to Surgical Damage
Other co-morbidities should be evaluated and optimized. In addition to anaemia, other predictors of post-operative morbidity and mortality include frailty, poor pre-operative functional capacity, renal insufficiency and cardiovascular disease.7,8 Frailty is defined as a syndrome of a lack of physiological reserve across multiple organ systems. It is more common with older age and can be assessed using a variety of different tools but is often not incorporated into peri-operative planning. Attempts to reduce frailty by improving pre-operative strength and cardiovascular fitness, known as pre-habilitation, make physiological sense for the frail patient, however the evidence base and outcomes remain equivocal.9
Intra-operative
There are multiple anaesthetic techniques available for revision hip replacement. General, spinal or epidural anaesthesia may be used and can be supplemented by intrathecal opioids, peripheral nerve blocks or surgical infiltration of local anaesthetic. The choice of technique will depend on several factors: the patient’s co-morbidities, the type of revision, reason for revision, expected duration and expected blood loss. Post-operative analgesia should also be considered when planning.
Spinal anaesthesia is quick and easy to perform and is currently the preferred option for patients undergoing primary hip replacement. It has been associated with a number of advantages and disadvantages for revision hip surgery.
(Table 1.) Certain cited benefits of spinal anaesthesia may be particularly useful in revision hip surgery. These include a reduction in VTE and peri-operative blood loss. However, relying on a spinal technique alone may not be of sufficient duration. In addition, a long duration of lying in the lateral position and potential for major blood loss might make general anaesthesia the preferred option.
A general anaesthetic (GA) can be combined with either a neuraxial or a peripheral regional technique. Combining GA and either a single shot spinal or lumbar epidural may help reduce blood loss, but can cause increased peri-operative hypotension. Intrathecal opioids can be added to help with early post-operative pain but are associated with increased PONV and pruritus. Hypotension can be limited by using a low volume of local anaesthetic as a carrier for intrathecal opioid. If a lumbar epidural is sited, then attention to coagulation status needs to be considered should major haemorrhage occur. A motor sparing infusion should be used post-operatively.
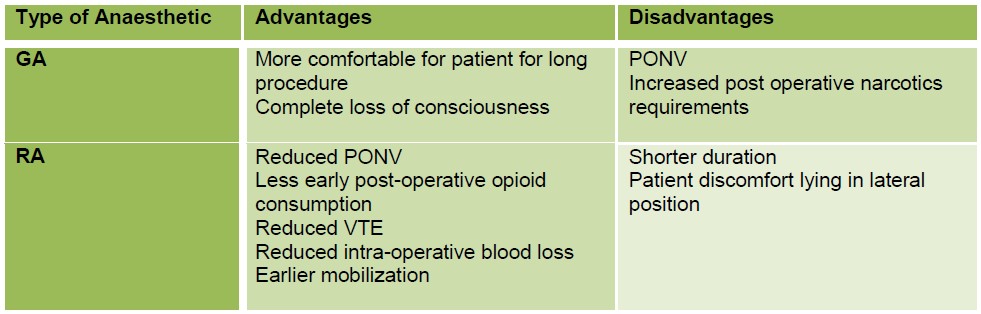
Table 1. Advantages and disadvantages of regional and general anaesthetic techniques
Regional techniques can be either single shot or continuous peripheral nerve blocks. The hip joint is innervated by three nerves; the femoral nerve (L2-4); sciatic nerve via the nerve to quadratus femoris (L4-S3); and the obturator nerve via its anterior division (L2-4). The lateral cutaneous nerve of the thigh is responsible for the area of skin through which the surgical incision is made. Complete analgesia therefore involves blocking all four nerves, which unfortunately is not obtainable with a single technique. Commonly performed nerve blocks include the lumbar plexus block, fascia iliaca compartment block and femoral nerve block. The lumbar plexus block covers all three nerves except the sciatic; however, it is a deep block and more technically challenging to perform reliably. The femoral nerve block and FICB are more superficial and straightforward to perform, but with less nerve coverage. If analgesia is desired then a sciatic nerve block will also be required.
Revision surgery is associated with a higher incidence of neurovascular injury than in primary hip replacements, and use of peripheral nerve blocks should be discussed with the surgeon, as they may be concerned regarding post-operative motor block.
Surgical infiltration of local anaesthetic is becoming increasingly popular, however there is conflicting evidence to suggest benefit over a fascia iliaca or femoral nerve blocks.10 The choice depends on preference and discussion between the orthopaedic and anaesthetic teams.
Monitoring
Choice of peri-operative monitoring depends on a multitude of factors including patient co-morbidity, expected duration, case complexity and physical access to the patient under anaesthesia. Wide bore peripheral access is mandatory given the potential for haemorrhage. Central venous access may be useful in patients with cardiovascular co-morbidity, in whom vasopressor and inotrope infusions are more likely, e.g. infected revision or cardiovascular co-morbidity, or in those with poor peripheral venous access. Obtaining central venous access mid-case is possible in the lateral position, but may be more challenging anatomically. Invasive arterial monitoring allows peri-operative blood sampling and more rapid detection of hypotension.
Goal directed therapy is associated with reduced complications in major abdominal surgery, and studies suggest there is also a role in elective major orthopaedic surgery.11 Options for patients under GA include pulse based contour analysis or trans-oesophageal Doppler. A recent study of patients undergoing revision hip surgery demonstrated reduced post-operative morbidity and length of stay in patients receiving GDT.12
As with any prolonged procedure consideration to pressure care and temperature management is vital. The operation is performed in the lateral position and therefore key areas for consideration include the upper limbs, contralateral hip and neck support. Patients should be kept normothermic using forced air and IV fluid warming techniques. This reduces peri-operative coagulopathy, post-operative confusion and patient comfort in recovery.
Haemodynamic control and haemorrhage
Tranexamic acid, an anti-fibrinolytic agent, has been shown to reduce peri-operative blood loss in patients undergoing primary and revision hip arthroplasty and is now common practice in many units for patients undergoing this surgery.13,14 The dose is 15mg/kg and its mechanism of action is by inhibition of plasminogen activation resulting in reduced clot lysis. It undergoes minimal hepatic metabolism and is therefore dependent on renal excretion; impaired kidney function requires careful dose reduction. Tranexamic acid contraindications include active thromboembolic disease and severe renal insufficiency. Despite not being associated with increased peri-operative VTE, patients with a personal or family history of VTE should only have tranexamic acid if there is a strong medical indication. Tranexamic acid has been shown to reduce haemoglobin drop and transfusion requirements in revision and in combination with cell salvage has been shown to reduce transfusions up to 60%.14
Intra-operative cell salvage should be considered for all cases considering the high risk of significant blood loss.15 It has been shown to reduce the need for blood transfusion and reduce the risk of post-operative cardiac events. Predictors of greater blood loss in revision surgery include male sex, older age, dual component revisions and cemented revisions.16
Cell salvage is not recommended for infected hip revisions. Cell salvage is also contraindicated in metal on metal wear as the indication for revision due to the higher chromium and cobalt levels found in the salvaged blood which are carcinogenic.17 Processing of salvaged blood removes platelets and plasma, and therefore early consideration should also be given to the management of coagulopathy in the face of major haemorrhage. Access to point of care devices, including ROTEM and TEG, may be helpful in guiding the administration of clotting products but remain unavailable in many centres.
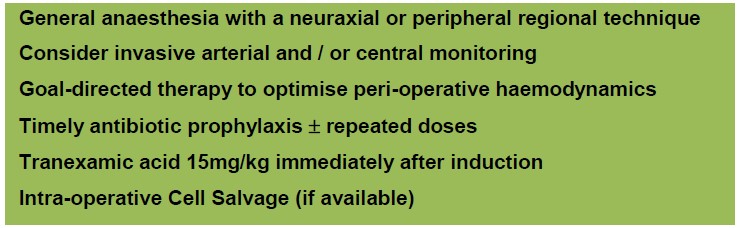
Table 2. Summary of Intra-operative Management
Post-operative
The post-operative care of patients’ who have undergone revision surgery is more complex (Table 3). Closer post-operative monitoring is essential and patients’ usually spend the first 24 to 48 hours in high-dependency care.
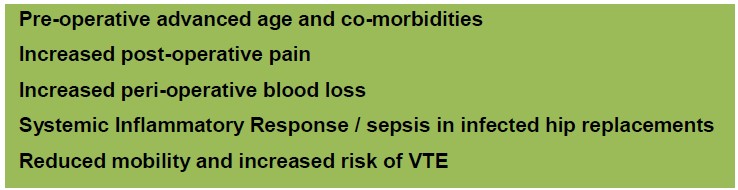
Table 3. Factors contributing to post-operative complications
Analgesia
Post-operative pain is usually higher than following a primary hip replacement for several reasons. A larger surgical incision is often required to gain adequate access to the acetabulum and femur, and a much larger surgical insult to the bony anatomy is made for implants removal and re-implantation. Patients taking regular analgesia should have this continued up to surgery, and may have significantly increased post-operative analgesic requirements due to down-regulation of opioid receptors. This needs to be factored in to the decision for post-operative analgesia (Figure 3).
Figure 3. Choices of analgesia available
Simple analgesia with paracetamol should be given provided there are no peri-operative contraindications. A short course of non-steroidals may be useful provided there are no ongoing concerns with haemostasis, or pre-existing renal impairment. Neuropathic adjuncts, such as gabapentin, have been show to reduce opioid requirements in primary arthoplasty, however, their role in revision surgery is unclear. Laxatives and anti-emetics should also be prescribed.
Recovery
Mobilisation is often slower and less aggressive than in primary hip replacement and requires increased physiotherapy and occupational therapy input. Coupled with the increased risk of post-operative complications, patients often require a longer hospital stay.
Disclosures: All figures and tables are the authors’ original work. There are no conflicts of interest to declare.
REFERENCES AND FURTHER READING
- National Joint Registry. National Joint Registry Annual Report (Internet). 2016 (Accessed 20/03/2017).http://www.njrcentre.org.uk/njrcentre/Portals/0/Documents/England/Reports/13th% 20Annual%20Report/07950%20NJR%20Annual%20Report%202016%20ONINE%20REPORT.pdf
- Frew NM, Cannon T, Nichol T, Smith TJ, Stockley I. Comparison of the elution properties of commercially available gentamicin and bone cement containing vancomycin with home-made™ preparations. Bone Joint J 2017 01/04;99-B(1):73.
- Fisher J, Jin Z, Tipper J, Stone M, Ingham E. Tribology of alternative bearings. Clin Ortho Relat Res 2006 Dec;453:25-34.
- Greenky M, Shaner J, Rasouli MR, Han S, Parvizi J, Hozack WJ. Intraoperative Blood Salvage in Revision Total Hip Arthroplasty: Who Benefits Most? J Arthroplasty 2014 6;29(6):1298-1300.
- Saleh E., McClelland D.B.L, Hay A. et al. Prevalence of anaemia before major joint arthroplasty and the potential impact of preoperative investigation and correction on perioperative blood transfusion. Br J Anaesth 2007;99:801-8
- Muñoz, M., Gómez-Ramírez, S. and Kozek-Langeneker, S. (2016), Pre-operative haematological assessment in patients scheduled for major surgery. Anaesthesia, 71: 19–28. doi:10.1111/anae.13304
- Jämsen E, Puolakka T, Eskelinen A, et al. Predictors of mortality following primary hip and knee replacement in the aged: A single-center analysis of 1,998 primary hip and knee replacements for primary osteoarthritis. Acta Orthopaedica. 2013;84(1):44-53. doi:10.3109/17453674.2012.752691.
- Richard Griffiths, MD FRCA, Madhur Mehta, FRCA MD DNB; Frailty and anaesthesia: what we need to know. Contin Educ Anaesth Crit Care Pain 2014; 14 (6): 273-277. doi: 10.1093/bjaceaccp/mkt069
- E. M. Soffin, J. T. YaDeau; Enhanced recovery after surgery for primary hip and knee arthroplasty: a review of the evidence. Br J Anaesth 2016; 117 (suppl_3): iii62-iii72. doi: 10.1093/bja/aew362
- Jiménez-Almonte JH, Wyles CC, Wyles SP, Norambuena-Morales GA, Báez PJ, Murad MH, Sierra RJ. Is Local Infiltration Analgesia Superior to Peripheral Nerve Blockade for Pain Management After THA: A Network Meta-analysis. Clin Orthop Relat Res. 2016 Feb;474(2):495-516. doi: 10.1007/s11999-015-4619-9.
- Cecconi M, Fasano N, Langiano N, et al. Goal-directed haemodynamic therapy during elective total hip arthroplasty under regional anaesthesia. Critical Care. 2011;15(3):R132. doi:10.1186/cc10246.
- Habicher M, Balzer F, Mezger V, et al. Implementation of goal-directed fluid therapy during hip revision arthroplasty: a matched cohort study. Perioperative Medicine. 2016;5:31. doi:10.1186/s13741-016-0056-x.
- Sukeik M, Alshryda S, Haddad FS, Mason JM. Systematic review and meta-analysis of the use of tranexamic acid in total hip replacement. J Bone Joint Surg Br. 2011 Jan;93(1):39-46.
- Park KJ, Couch CG, Edwards PK, Siegel ER, Mears SC, Barnes CL. Tranexamic Acid Reduces Blood Transfusions in Revision Total Hip Arthroplasty. J Arthroplasty 2016;31(12):2850-2855. e1.
- Herd JM, Joseph JJ, McGarvey M, et al. Intraoperative cell salvage in revision hip surgery. Annals of Medicine and Surgery 2014;3(1):8-12.
- Mahadevan D, Challand C, Keenan J. Revision total hip replacement: predictors of blood loss, transfusion requirements, and length of hospitalisation. Journal of Orthopaedics and Traumatology : Official Journal of the Italian Society of Orthopaedics and Traumatology. 2010;11(3):159-165.
- Coventry R, Cranfield K, Ashcroft GP. Cell Salvage and revision metal on metal total hip replacements. Anaesthesia Cases 2014. (Accessed 21/04/2017). Available from: http://www.anaesthesiacases.org/case-reports/2014-0214.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/