Obstetrics Anaesthesia

KEY POINTS
- Preconception counselling, planning, and evaluating patients is essential in pregnant patients with Takayasu arteritis.
- Multidisciplinary management of these patients during pregnancy is important to ensure good maternal and foetal outcomes.
- Planning the mode of delivery, assessing both obstetric and anaesthetic factors, while managing blood pressure control is the main goal in managing patients with Takayasu arteritis.
INTRODUCTION
Takayasu arteritis (TA) is a rare granulomatous pan-arteritis of unknown aetiology affecting the aorta and its main branches.1 It is characterized by stenosis, thrombosis, and formation of aneurysms, which affect organ perfusion.1 The global incidence of TA is 1.2-2.6 cases per million annually and it is most prevalent in Asia. Females of childbearing age are predominantly affected.2 TA has a preocclusive phase of rheumatic or systemic symptoms with segmental arterial involvement.1 Angiography (computed tomography or magnetic resonance imaging) is the gold standard for the diagnosis and classification of TA. Classification is based on the distribution of the vessels affected and is summarized in Table 1.3 Criteria for the classification of TA are summarized in Table 2.4
The normal physiological cardiovascular changes seen during pregnancy (as discussed in ATOTW 25 and 185) occur secondary to changes in hormone activity, mechanical effects of an enlarging uterus and the increased metabolic demands of pregnancy.5 Typical changes include an increase in heart rate and stroke volume and a decrease in systemic vascular resistance (SVR). The decrease in SVR is due to nitric oxide, prostaglandins, progesterone, the low resistance of the placenta and decreased blood viscosity from dilutional anaemia, which all contribute to physiological lower blood pressure (BP). As a result, the cardiac output (CO) increases up to 50% as the pregnancy advances. The increase in CO directs blood toward the uterus, placenta, kidneys, skin and extremities. In late pregnancy, uterine blood flow significantly increases and renal blood flow increases by 50%.6 During active labour, uterine contractions result in ‘auto-transfusion’ of 500 mL of blood back into maternal circulation, increasing preload to the heart, and following delivery, relief of inferior vena cava compression leads to a 75% CO increase.6
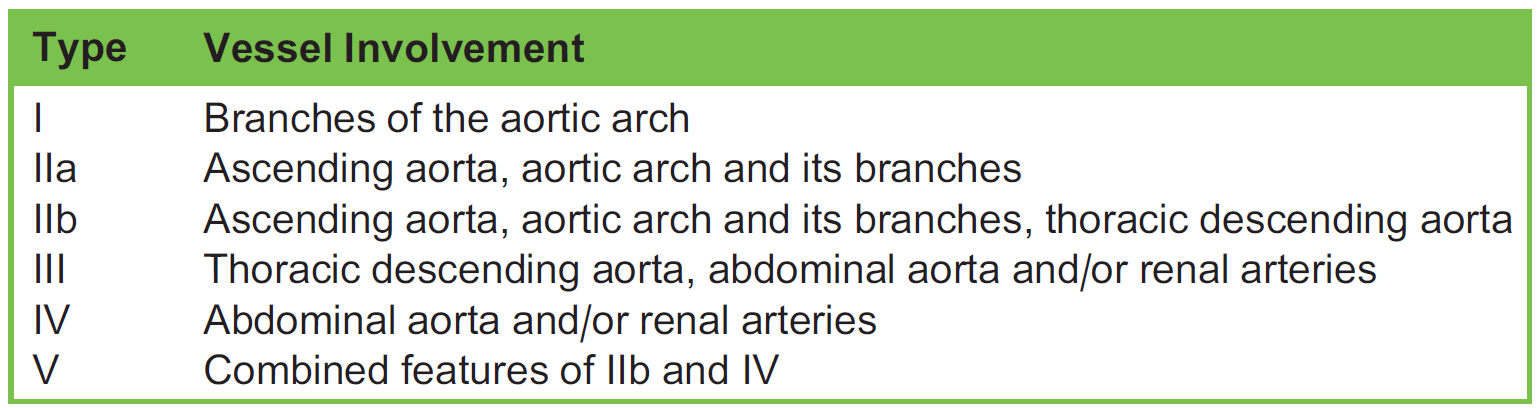
Table 1. The Classification of Takayasu Arteritis
ANTEPARTUM CONSIDERATIONS IN A PATIENT WITH TA
In the preconception period, counselling is important, focusing on the optimal timing of pregnancy, education on the risks associated with TA to mother and foetus, dosage adjustments of medications, treatment regimen alterations, and cessation of cytotoxic medications. The treatment of TA in pregnancy involves the use of corticosteroids as the first line of treatment for the inflammatory activity and immunosuppressors, including methotrexate and azathioprine, as well as antihypertensives.
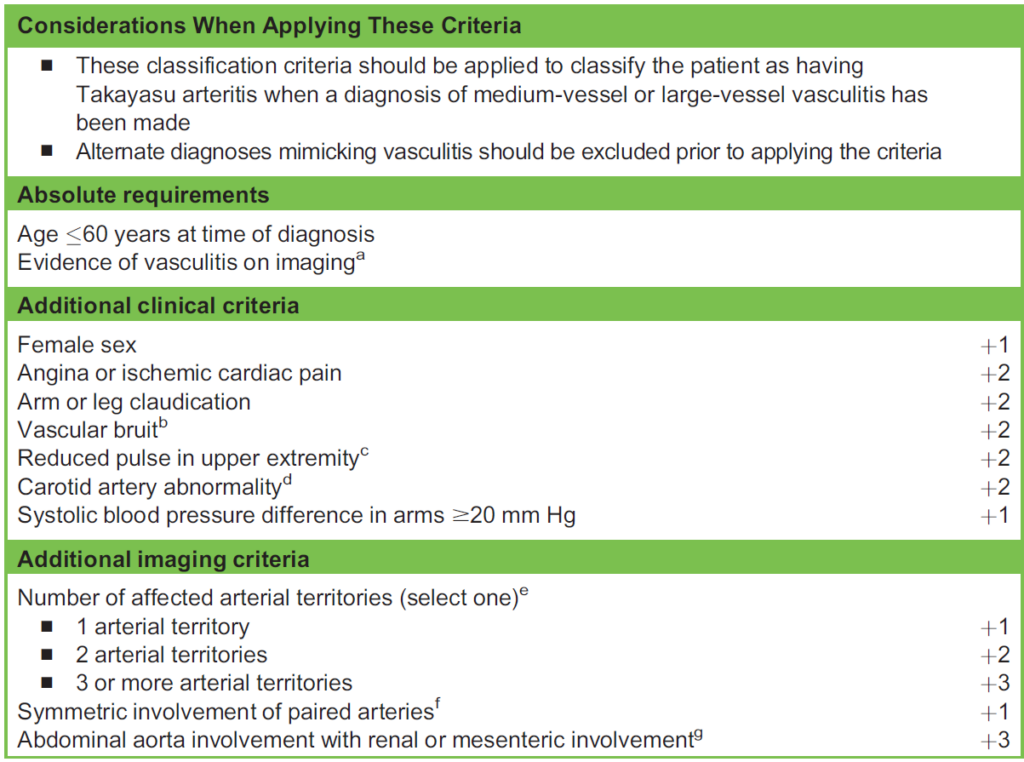
Table 2. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Takayasu Arteritis. Sum the scores for 10 items, if present. A score of $5 points is needed for the classification of Takayasu arteritis. aEvidence of vasculitis in the aorta or branch arteries must be confirmed by vascular imaging (eg, computed tomographic/catheter-based/ magnetiable 2c resonance angiography, ultrasound, positron emission tomography). bBruit detected by auscultation of a large artery, including the aorta, carotid, subclavian, axillary, brachial, renal, or iliofemoral arteries. cReduction or absence of pulse by physical examination of the axillary, brachial, or radial arteries. dReduction or absence of pulse of the carotid artery or tenderness of the carotid artery. eNumber of arterial territories with luminal damage (eg, stenosis, occlusion, or aneurysm) detected by angiography or ultrasonography from the following 9 territories: thoracic aorta, abdominal aorta, mesenteric, left or right carotid, left or right subclavian, left or right renal arteries. fBilateral luminal damage (stenosis, occlusion, or aneurysm) detected by angiography or ultrasonography in any of the following paired vascular territories: carotid, subclavian, or renal arteries. gLuminal damage (stenosis, occlusion, aneurysm) detected by angi- ography or ultrasonography involving the abdominal aorta and either the renal or mesenteric arteries
Chronic use of corticosteroids could potentially lead to adrenal suppression during stress, gestational diabetes, infections, and foetal malformations.7 Although azathioprine has been shown to be compatible with pregnancy, methotrexate is associated with miscarriage and birth defects. Maintaining BP control is crucial, and antihypertensive agents that are safely used in pregnancy include labetalol, hydralazine, and alpha-methyldopa.8
During the antepartum period these patients should be managed in a high-risk obstetric unit. Frequent antenatal visits are required to monitor the foetus, maternal BP (with preeclamptic screening), and maternal renal function.9 Antepartum care requires a multidisciplinary approach involving input from obstetricians, cardiologists, anaesthesiologists, rheumatologists, and neonatologists. It is important to prevent disease progression and inflammation with the early identification, vigilant monitoring, and active treatment of hypertension as well as cardiac, stenotic, and occlusive lesions.3 Timeous referral for an anaesthetic consultation for a planned delivery is beneficial for patient evaluation, optimization, and appropriate investigations.
Current literature suggests that pregnancy does not affect the disease progression of TA, but cardiovascular complications (hypertension, preeclampsia, aortic dissection, and heart failure) are possibly enhanced because of the cardiovascular changes that occur during pregnancy and labour and the vascular pathology associated with TA, especially in type III and IV patients with renovascular involvement.2 Uncontrolled hypertension, extensive aortic disease and reduced iliac artery blood flow due to stenotic lesions may result in utero-placental insufficiency, intrauterine growth restriction, low birth weight, and pregnancy loss.2
ANAESTHETIC CONSIDERATIONS WHEN MANAGING AN INTRAPARTUM PATIENT WITH TA
Complications during labour arise because of acute increases in SVR from increased sympathetic nervous system (SNS) activation from pain during contractions and delivery. This can exacerbate hypertension, predisposing the TA patient to a cerebral vascular accident (CVA) and heart failure.10
The decision on the timing and mode of delivery is individualized and based on the health status and type of TA. The goal in patients with TA undergoing anaesthesia includes the maintenance of BP and end-organ perfusion (especially cerebral, renal, myocardial, and placental) in the perioperative period.3
The pathophysiology of TA makes end organs susceptible to hypoperfusion because a drop in mean arterial pressure (MAP) leads to flow-limiting effects from stenotic lesions and aneurysmal dilatations along the aorta and its branches. This reduced blood flow may result in a CVA, myocardial infarction (MI) and foetal acidosis with or without hypoxemia. Conversely, complications due to vessel wall stress from a hypertensive response include CVA, exsanguination from dissection or rupture of aortic aneurysms, cardiac tamponade, coronary occlusion and MI, or aortic regurgitation.
These patients are prone to secondary chronic hypertension and their cerebral blood flow (CBF) autoregulation curve shifts to the right. The lower MAP limit, at which autoregulation of CBF is maintained, is likely higher in these patients, further emphasizing the importance of tighter BP control.1
Noninvasive BP monitoring may be inaccurate because of discrepancies in limb pulses caused by stenotic lesions.9 Invasive BP (IBP) monitoring is beneficial, allowing for beat-to-beat BP monitoring and prompt hemodynamic management provided a central site or one with good pulses is chosen. IBP monitoring should be placed in vessels that are unaffected by stenotic lesions, or in central arteries such as the femoral artery. In the setting where no IBP is available, monitoring of noninvasive BP in limbs with unaffected vessels should be considered and attention should be paid to maintaining BP close to baseline values.
Anaesthetic technique is important to maintain hemodynamic stability.11 Generally, vaginal delivery with epidural analgesia and hemodynamic monitoring is the preferred method of delivery in patients with type I or IIa TA. BP monitoring and the prevention of fluctuations in BP are important during the intrapartum period.3
Caesarean section is recommended in more complicated cases (type IIb and type III disease).2 Currently, there is no expert consensus or evidence-based data to support one approach. Case studies describe the successful intraoperative management of these patients for caesarean section using both general anaesthetic (GA) and neuraxial anaesthetic techniques. The choice depends on the availability of resources, hemodynamic monitoring tools, and anaesthesia provider experience.
Considerations with the use of GA include tracheal intubation and extubation, as well as depth of anaesthesia. Regarding the first two, these may produce a SNS hypertensive response to intubation, followed by a hypotensive response to vasodilatation from the induction and maintenance anaesthetic agents, leading to complications discussed above. Blunting of the intubation and extubation response is essential, and attention must be paid to depth of anaesthesia as target MACs of volatile agents are often lowered to reduce effects on uterine contractility and avoid possible peripartum haemorrhage after delivery. A multimodal intraoperative and postoperative analgesic plan is critical.
Neurophysiological or cerebral oximetry monitoring is recommended when available for patients undergoing GA. It is used as a surrogate marker of adequacy of regional brain tissue perfusion for such patients. When not available, as in resource-limited settings, IBP is useful as MAP can guide the maintenance of cerebral perfusion pressure where the intracranial pressure is normal.12
Airway management, as discussed in ATOTW 393, has special considerations in obstetric patients, as the physiological effects of pregnancy make laryngoscopy and intubation more difficult as they are prone to rapid desaturation and are an aspiration risk. Rheumatoid arthritis, which may coexist with TA, can limit joint mobility and neck extension, which adds further risk to airway management.13 Neuraxial techniques (spinal and epidural) are preferred for caesarean section as they avoid the airway management risks mentioned above.14 Their use allows for mother-infant bonding, improved patient experience and postoperative analgesia (in centres with resources for postoperative epidural analgesia).14 Single-shot spinals can cause hypotension due to the loss of SNS effect on vessel tone, resulting in complications discussed above. Their use may not be suitable in patients with hemodynamic instability, those with severe cardiac pathology, and those on anticoagulants or with coagulopathy.1 Graded epidurals, on the other hand, allow for the slow titration of the neuraxial blockade and compensatory mechanisms prevent an acute drop in preload. The choice of anaesthetic used should be tailored according to the presentation of the patient after a careful consideration of the risks and benefits.
A neonatologist should attend the delivery to assist with possible resuscitation of the neonate, particularly if there is evidence of intrauterine growth restriction or foetal hypoxaemia or if the decision for GA is made. The maternal drug history should be communicated to the neonatologist.
ANAESTHETIC CONSIDERATIONS WHEN MANAGING A POSTPARTUM PATIENT WITH TA
Because of massive fluid shifts seen during the intrapartum period, close monitoring should continue postoperatively to ensure adequate arterial BP and organ perfusion is achieved. Adequate postoperative multimodal analgesia should be prescribed to alleviate the increase in BP associated with pain; patient-controlled analgesia and regional techniques should be considered. Postoperative monitoring in a high-dependency unit setting in the first 24-72 hours postoperatively is important to monitor for hypoperfusion and hypertensive complications.7 Investigations such as renal function testing, cardiac biomarker monitoring or postdelivery imaging may be required to diagnose and manage any complications occurring in the immediate postoperative period if there is clinical suspicion. Pregnancy is generally considered a procoagulant state, and TA patients are at risk for thrombosis due to low flow in stenotic vessels. Therefore, deep vein thrombosis prophylaxis should be initiated carefully postoperatively in these patients, especially if epidural anaesthesia is utilized. Attention should be paid to the timing of removal of epidural catheters in relation to the last dose of anticoagulation administration.
Close follow-up post hospital discharge of these patients by the obstetric team will be required because of the risks of preeclampsia persisting for up to 6 weeks postdelivery, and consideration should be given to the optimum form of contraception for these patients. Consultation with the patient’s long-term health care providers will be required to reestablish anti-inflammatory medication while considering the drugs that are safe for breastfeeding mothers. The degree and duration of follow-up required are based on the severity of TA in the individual patient. The mortality of patients with TA is increased compared with age- and sex-matched healthy controls, with one study reporting a median age at death of 38 years old. Common causes of death include mesenteric ischaemia and aortic aneurysm rupture.15
SUMMARY
The main goal in the management of a pregnant TA patient is to avoid hemodynamic changes and to maintain organ perfusion during the perioperative period.16 Anaesthetic considerations need to be decided on a case-by-case basis and based on the availability of infrastructure and equipment. A neuraxial technique, specifically a graded epidural, with invasive arterial BP monitoring allows for this in a resource-constrained setting.
REFERENCES
Dutta B, Pandey R, Darlong V, et al. Low-dose spinal anaesthesia for a parturient with Takayasu’s arteritis undergoing emergency caesarean section. Singapore Med J. 2010;51(6):e111-e113.
Bharuthram N, Tikly M. Pregnancy and Takayasu arteritis: case-based review. Rheumatol Int. 2020;40(5):799-809.
Itani R, Elmallahi N, Ramadan MAA, et al. Pregnancy with Takayasu’s arteritis: a case report and literature review. Cureus. 2018;10(9):e3370.
Johnston S, Lock RJ, Gompels M. Takayasu arteritis: a review. J Clin Pathol. 2002;55(7):481-486.
Gropper MA, Cohen NH, Eriksson LI, Fleisher LA, Leslie K, Wiener-Kronish JP. Miller’s Anesthesia. Vol 2. 9th ed. Philadelphia, PA: Elsevier; 2020:2367-2370.
Kepley JM, Bates K, Mohiuddin SS. Physiology, maternal changes. In: StatPearls. Treasure Island, FL; StatPearls Publishing; 2022.
Leal PC, Silveira FF, Sadatsune EJ, et al. Takayasus’s arteritis in pregnancy. Case report and literature review. Rev Bras Anestesiol. 2011;61(4):479-485.
Shafi NA, Malik A, Silverman DI. Management of Takayasu arteritis during pregnancy. J Clin Hypertens. 2009;11(7):383-385. doi: 10.1111/j.1751-7176.2009.00135.x- Raka M, Singh A. Takayasu’s arteritis in pregnancy: a rare case report. Cureus. 2022;14(9):e28815.
Ioscovich A, Gislason R, Fadeev A, et al. Peripartum anesthetic management of patients with Takayasu’s arteritis: case series and review. Int J Obstet Anesth. 2008;17(4):358-364.
Motiaa Y, Ouassou Z, Azizi K, et al. Anesthetic management of cesarean section for parturient with Takayasu’s arteritis. J Anesth Intensive Care Med. 2019;9(1):555751.
Poonam SG, Kalpana DH. Anesthetic considerations in a patient with Takayasu’s arteritis for caesarean section. Ain-Shams J Anaesthesiol. 2015;8:681-682.
Lee EH, Choi E, Ahn W. Application of cerebral oximetry for a parturient with Takayasu’s arteritis undergoing cesarean section— a case report. Korean J Anesthesiol. 2013;65(2):158-162.
Iddrisu M, Khan ZH. Anesthesia for cesarean delivery: general or regional anesthesia—a systematic review. Ain-Shams J Anesthesiol. 2021;13(1).
Mirouse A, Biard L, Comarmond C, et al. Overall survival and mortality risk factors in Takayasu’s arteritis: a multicenter study of 318 patients. J Autoimmun. 2019;96:35-39.
Beilin Y, Bernstein H. Successful epidural anaesthesia for a patient with Takayasu’s arteritis presenting for caesarean section. Can J Anaesth. 1993;40(1):64-66.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/