Basic Sciences

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
Multiple Choice Questions: for each option, choose true or false.
- The following reduce the functional residual capacity:
a. obesity
b. old age
c. pregnancy
d. general anaesthesia
e. supine position - Alveolar partial pressure of oxygen (PAO2) is directly influenced by:
a. altitude
b. inspired oxygen
c. laryngoscopy
d. weight
e. hyperventilation - Single Best Answer: choose the single most appropriate option as the answer. Pre-oxygenation is best achieved by the following method:
a. 10 L/min O2 via Hudson mask for 5 minutes
b. 8 vital capacity breaths over one minute of 100% O2 via a tightly fitting face-mask
c. 12 tidal breaths over one minute of 100% O2 via a tightly fitting face-mask
d. 3 minutes of tidal breathing of 100% O2 with the patient holding the face-mask
e. 15 L/min O2 via a non-rebreathing mask for 7 minutes
INTRODUCTION
The purpose of pre-oxygenation is to increase physiological stores of oxygen in order to prolong the time to desaturation during a period of apnoea, such as frequently happens upon induction of anaesthesia. This is particularly the case during a rapid sequence induction, when positive pressure ventilation is avoided prior to intubation of the trachea. Pre-oxygenation can also be thought of as de-nitrogenation – highlighting the fact that it is the nitrogen within the lungs that is being displaced by a high inspired oxygen concentration.
The rate of oxygen de-saturation is influenced by the balance between oxygen stores and consumption. Oxygen is stored in the body within the lungs, blood and tissues. In the context of pre-oxygenation, the greatest increase in oxygen store is within the lungs; more specifically, the functional residual capacity (FRC). Lung oxygen reserves are a product of the fraction of oxygen within the alveoli (which we estimate by measuring the oxygen fraction in expired gas – FeO2) and FRC. Ventilation-perfusion (V/Q) mismatch, particularly shunt, is an additional factor that affects oxygen content of blood. This may be influenced by the relationship between the FRC and the closing capacity. Oxygen consumption is influenced by metabolic rate. Shorter time to desaturation occurs in certain clinical scenarios including obesity, sepsis, pregnancy and in the paediatric population.
FUNCTIONAL RESIDUAL CAPACITY
The FRC is the volume of gas remaining in the lungs at the end of a normal tidal expiration and reflects the balance between the tendencies for the chest wall to expand outwards and the lungs to collapse inwards. The spirometry diagram below depicts the FRC and other lung volumes. In a healthy adult, the FRC amounts to 30 ml/kg, totalling 2100 ml in a 70 kg adult. However, many patients presenting for surgery have a reduced FRC, which in turn will reduce the lung’s oxygen store. Reasons for this include obesity, pregnancy, anaesthesia (with or without neuromuscular blockade) and lung disease. Nonetheless, pre-oxygenation will still be beneficial in comparison to breathing room air.
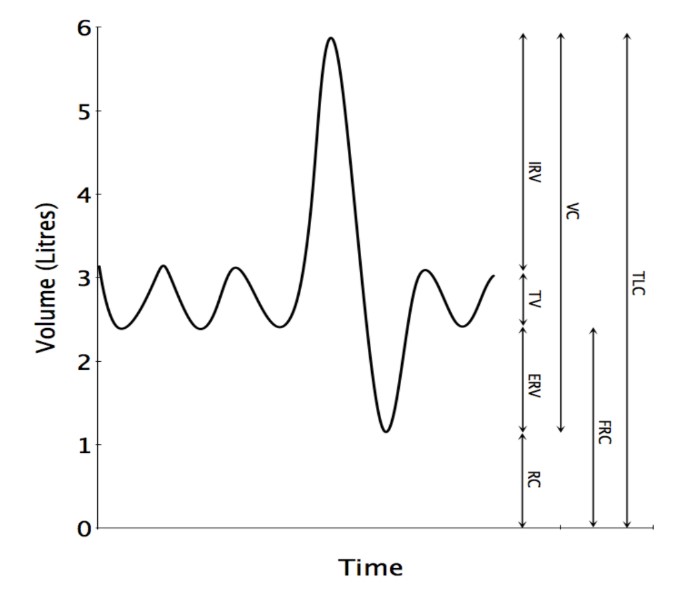
Figure 1. Spirometry trace depicting lung volumes and capacities. IRV = Inspiratory reserve volume, TV = Tidal volume, ERV = Expiratory reserve volume, RC = Residual capacity, VC = Vital capacity, FRC = Functional residual capacity, TLC = Total lung capacity.
Calculating oxygen reserves
It is possible to calculate oxygen delivery and usage to demonstrate the effects of pre-oxygenation:
The alveolar gas equation is used to calculate PAO2:
PAO2 = PiO2 – [PACO2/R]
When breathing air (21% O2):
PAO2 = 0.21 x (101.3 – 6.7) – 5.3/0.8 = 13.2 kPa
This is equivalent to 13% (273ml) of oxygen in an FRC of 2100ml, the remaining contents being 75% nitrogen, and the 7% water vapour and 5% carbon dioxide used in the alveolar gas equation calculation.
For the purposes of calculation, oxygen consumption at rest is considered to be 3.5 ml/kg/min. Continuing with the example of a 70 kg adult, approximately 250 ml/min of oxygen is consumed. Thus, in this model, the FRC provides a reservoir of oxygen equivalent to 70 seconds worth of oxygen consumption. Not all of this oxygen can be extracted from the alveoli; once the PAO2 falls below 6kPa, there will be little concentration gradient to maintain flux of oxygen to haemoglobin. The amount of useable oxygen in this reservoir is therefore likely to be only around 150ml. Actual time to desaturation depends on a complex set of factors as described above.
Pre-oxygenation is a highly efficacious way of extending the time to exhaustion of oxygen reserves and desaturation.
When breathing 100% Oxygen*:
PAO2 = (101.3 – 6.7) – [5.3/0.8] = 88 kPa*
This is equivalent to approximately 88% (1800ml) of oxygen in the FRC – equivalent to more than seven minutes worth of oxygen consumption, or around ten times the amount of useable oxygen compared to breathing room air.
This demonstrates that replacing the nitrogen in the FRC with oxygen greatly increases available reserves.
*Note – This is a theoretical figure. Achieving perfect pre-oxygenation is often not possible; aiming for an ETO2 > 85% is a good goal. This will still give over 1500ml of pulmonary oxygen in this example.
Shunt
As well as providing a smaller reservoir of oxygen, the relevance of a reduced FRC extends to V/Q mismatch. The closing capacity is the lung volume at which small airways will close. If the FRC falls within the closing capacity, airways will close during tidal breathing, resulting in alveoli that are perfused but not ventilated. This is known as shunt, a phenomenon which is not improved by the administration of 100% oxygen.
APNOEA
During the apnoeic period, oxygen continues to be taken up into the blood from the lungs. The uptake of oxygen from the lungs far exceeds the return of carbon dioxide from the blood to the alveoli (due to the body’s extensive buffering systems which absorb large quantities of CO2). This net loss of volume leads to a negative pressure developing in the lungs.
If the upper airway is patent, gas will be continually drawn via the trachea into the lungs, equalising the pressure gradient. If the gas in the upper airway is 100% oxygen, this pressure gradient can be maintained for a long period (this has been predicted with theoretical modelling for more than half an hour). This phenomenon (which may be referred to as the oxygen elevator) can significantly prolong the time until de-saturation. It should be noted that carbon dioxide is not transferred out of the lung during this process, so there will be a gradual rise in PaCO2.
If the gas in the upper airway has a low fraction of oxygen (e.g. air) then nitrogen will build up in the lungs, effectively being concentrated, resulting in loss of the pressure gradient and cessation of flow.
If the airway is obstructed during this time, there will be rapid development of negative intrapulmonary pressure. Not only will this result in missing the benefits of the oxygen elevator, but may cause airway collapse and pulmonary oedema.
This reinforces the benefits of maintenance of a patent airway and application of 100% oxygen as good practice during apnoea at induction of anaesthesia.
PRACTICALITIES
Various methods have been described to achieve the process of pre-oxygenation. A consistent feature is the requirement for a tightly fitting mask, with the avoidance of any leak which would allow for entrainment of room air, and therefore nitrogen. Selection of an appropriate size of mask is important. Difficulty achieving a good seal may be found with bearded or edentulous patients in particular. An alternative in situations such as inability to prevent leaks or a severe phobia of the mask, is to ask the patient to form a seal around the catheter-mount with the mask removed, ensuring that they do not breathe through the nose (consider the use of a nose clip). This can be useful for patients who suffer from claustrophobia with facemasks
Timing
The necessary duration of pre-oxygenation has been debated and studied extensively, with options including three minutes of tidal breathing, four vital capacity breaths in 30 seconds or eight vital capacity breaths in 60 seconds. To some extent these fixed regimens are unnecessary in the presence of end tidal oxygen monitoring (ETO2). If this monitoring is available it is possible to observe the rise in ETO2 on a breath-by-breath basis, with an endpoint of achieving an ETO2 > 85% (100% is not achievable due to the presence of CO2 and water vapour). The actual time required will vary between patients; it may be achieved more quickly than three minutes, especially if a patient has a relatively small FRC, while in certain circumstances it can take longer. In the absence of ETO2 monitoring, either 3 minutes of tidal breathing or eight vital capacity breaths in 60 seconds is recommended. Four vital capacity breaths in 30 seconds has been found to be inferior to the other two methods. With either method, it is advantageous for the patient to exhale completely (down to residual volume) prior to the start of pre- oxygenation.
The filling of the FRC with oxygen can be described by a wash-in curve and the contrasting process of de-nitrogenation is represented by a wash-out curve. Both processes are negatively exponential and allow for an understanding of the methods for pre-oxygenation suggested.
Time Constants
The nitrogen wash-out curve corresponds to the formula y = a.e-kt.
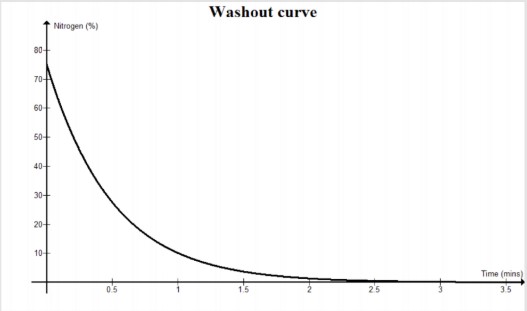
The time constant of an exponential process relates to the time taken for the value of the exponential (in this case the amount of nitrogen in the FRC) to fall to 37% of its previous value. As a result, after four time constants the process will be 98% complete. The time constant relates to the ratio of volume and flow, i.e. FRC and alveolar minute ventilation (VA). For the 70 kg patient with a tidal volume of 490 ml (7ml/kg), a respiratory rate of 12 breaths per minute and anatomical dead space of 140 ml (2 ml/kg), VA would be 4200 ml/min. As noted above, the FRC is 2100 ml. Consequently, a time constant of 0.5 minutes is obtained.
From the calculations above, it is evident that after two minutes (four time constants), 98% of the nitrogen in the FRC will have been washed out and replaced with oxygen. A three minute period ensures a safe margin to account for inter-patient variability.
Breathing system
The breathing system employed during pre-oxygenation should be taken into consideration. When using a circle system it is necessary to ensure an oxygen flow greater than minute ventilation (MV); i.e. at least 6 L/min in the 70 kg patient, in order to maintain 100% oxygen within the circuit. Higher flows (15 L/min) are required if vital capacity breaths, rather than tidal breathing, are taking place (due to the increased MV). With a Mapleson D breathing system (Bain circuit) high oxygen flows (2-3 x MV) are required to prevent rebreathing of expired nitrogen and carbon dioxide.
OTHER CONSIDERATIONS
Obesity
As noted above, the balance between oxygen stores and oxygen consumption determines the rate of de-saturation of a patient. Obese patients have a reduced FRC (store) and a greater metabolic rate (consumption). Consequently, their rate of de-saturation is notably greater than the non-obese patient. Coupled with a higher rate of difficult bag mask ventilation and difficult intubation, there is a key role for pre-oxygenation in the obese patient in order to maximise the PAO2 (store). A further adjustment to the process is to sit such patients up. This improves matters by increasing the FRC compared to the supine position, with a 25 degree elevation having been shown to significantly reduce the rate of de-saturation in obese patients.
Pregnancy
Pre-oxygenation has an important role to play in the anaesthetic management of the pregnant patient. The enlarging uterus causes elevation of the diaphragm and a reduced FRC, within which the closing capacity may fall. Metabolic demand increases due to the growing foetus and placenta. Therefore, de-saturation occurs more rapidly. Furthermore, airway management in obstetric patients is known to be difficult more frequently than in the general surgical population. Pre-oxygenation provides an added margin of safety if efforts at establishing an airway become prolonged. Unlike obesity the 25 degree head up position has not been shown to reduce the rate of desaturation of pregnant patients.
Sepsis
In critically ill and septic patients the time taken to de-saturate can be greatly reduced. Factors that influence this are an increase in oxygen demand and cardiac output, and reduced tissue oxygen extraction associated with sepsis. There is a likelihood that V/Q mismatch is increased, further compounding the problem of rapid desaturation. In such patients achieving ideal oxygen saturations approaching 100% can be difficult, even with the administration of 100% oxygen. However, good quality de-nitrogenation of the patient’s FRC prior to intubation (and associated apnoea) will still help to delay a precipitous fall in oxygen saturation.
Paediatrics
Children may be less likely to tolerate the process of pre-oxygenation. However, its use should be carefully considered as children have a higher metabolic rate than adults and de-saturate more quickly as a result. Many children will cooperate with the process when it is explained to them and efforts should be made to do this in individuals at high risk of desaturation.
Tracheal Extubation
Much of the preceding text has referred to the use of pre-oxygenation prior to induction of anaesthesia. It should be noted that the same principles of increasing oxygen stores within the FRC are of use prior to tracheal extubation, providing additional oxygen stores in the event of an airway complication at this time. Correlation with ETO2 is of use to ensure adequate de-nitrogenation.
CAUTIONS
One deleterious effect of the administration of 100% oxygen is atelectasis. This results from oxygen uptake from poorly-ventilated alveoli leading to alveolar collapse. However, this problem may be easily remedied through the use of recruitment manoeuvres and should not be seen as a contra-indication to the appropriate use of pre-oxygenation. Once a secure airway has been obtained, the FiO2 may be reduced to an appropriate level for that particular patient.
Rare circumstances where the risk-benefit balance may not be in favour of the use of 100% oxygen are in patients receiving bleomycin treatment and those with conditions in which the pulmonary vasculature is sensitive to changes in the FiO2. The latter are a special case where high FiO2 may need to be avoided. Expert advice should be sought. Bleomycin is asssociated with a pneumonitis, which can be potentiated by a high FiO2. The short periods of time for which 100% oxygen is used in the context of pre-oxygenation are deemed to be safe when balanced with a lower maintenance FiO2. Further detail about this is beyond the scope of this article.
SUMMARY
Pre-oxygenation is:
- Safe
- Simple
- Cheap
- Effective
- Well-tolerated
When properly performed it will prolong the time until desaturation when apnoea occurs.
Maintenance of a patent airway with continued application of 100% oxygen during apnoea further prolongs the time to desaturation.
ANSWERS TO QUESTIONS
Multiple Choice Questions:
- TFTTT
Obesity, pregnancy and general anaesthesia all reduce the FRC, as does changing from the erect to the supine position. Old age in itself does not reduce FRC, though the closing capacity may encroach upon tidal breathing with advancing age. - TTFFT
The alveolar gas equation is used to answer this question. High altitude is associated with a reduction on atmospheric pressure and therefore the partial pressure of oxygen. Hyperventilation reduces the PACO2. Although increasing weight/obesity reduces the FRC, this does not affect the PAO2. - Single Best Answer: B
Of the options offered, only 8 vital capacity breaths over one minute of 100% O2 via a tightly fitting face-mask is advised as a method of preoxygenation. Although 3 minutes of tidal breathing of 100% O2 can adequately preoxygenate a patient, there is a significant risk of leaks if the patient holds the face-mask for this.
REFERENCES and FURTHER READING
- Tanoubi I, Drolet P, Donati F. Optimizing pre-oxygenation in adults. Can J Anesth (2009) 56:449–466
- Hardman JG, Wills JS, Aitkenhead AR. Factors determining the onset and course of hypoxaemia during apnoea: an investigation using physiological modelling. Anesth Analg 2000; 90: 619–24
- Wills J, Sirian R. Physiology of apnoea and the benefits of pre-oxygenation. Continuing Education in Anaesthesia, Critical Care & Pain (2009) Volume 9 Number 4: 105 -108
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/