Basic Sciences

KEY POINTS
- Surgical face masks and respirators are recommended for prevention of droplet spread and contraction of COVID-19.
- SARS-CoV2 is mainly transmitted via droplets and contact routes, but evidence of airborne transmission is emerging.
- Spunbond and meltblown polypropylene make up the nonwoven fabric of masks. Filtration efficiency depends on the ability of the meltblown filtering layer to filter out particulates and bacteria (a key factor that determines their level of classification).
- Extended use, limited reuse and decontamination of respirators have been suggested as methods to conserve supplies during the current COVID-19 pandemic.
INTRODUCTION
The recent COVID-19 pandemic, caused by the novel coronavirus SARS-CoV2, has led to a worldwide shortage of personal protective equipment (PPE) for health care workers, especially face masks. There has been much confusion over the differences between various types of face masks and recommendations for their usage in different types of health care settings. In this tutorial, we review the various modes of respiratory pathogen transmission with a specific emphasis on COVID-19. In addition, we describe the basic structure of several types of face masks, recommendations for their use and suggestions for conservation. In the face of the ongoing pandemic and resulting PPE shortages, conservation while ensuring safety is paramount.
PATHOGEN TRANSMISSION
Transmission of pathogens requires 3 components: a source, a susceptible host and a mode of transmission.1 Depending on the pathogen, the mode of transmission varies.
Contact Transmission: Direct Versus Indirect
Direct transmission occurs when microorganisms are transferred from an infected individual to a susceptible individual by physical contact. Indirect contact transmission occurs when there is no direct human-to-human contact. There is an intermediate object that transmits the microorganism.
Respiratory Transmission: Droplet Versus Aerosol Versus ‘Airborne’
Droplets containing infectious pathogens can be generated via coughing, sneezing, or talking. Most droplets are too large to remain suspended in air for long periods of time and will quickly settle. Droplet particles .5-10 lm in diameter are transmitted this way.
An aerosol is a finer droplet (,5-10 lm) that can remain suspended in air when the velocities of the air current exceed the terminal velocities of the particles. Alternatively, the droplets may evaporate before they hit the floor, leaving an even smaller droplet nuclei, free to float over longer distances. In such situations, pathogens are considered ‘airborne’. Airborne transmission is defined as dried infectious material smaller than 5 lm that can travel on air currents over considerable distances.
The distance a droplet can reach and result in disease transmission depends on the following:
- the velocity and mechanism by which they are propelled;
- the density of respiratory secretions and infective load of the secretion;
- environmental factors such as concurrent airflow, temperature and humidity; and
- the ability of the pathogen to maintain infectivity over that distance.
Respiratory aerosols are created naturally or during aerosol-generating procedures (see below). They can carry the pathogen directly from the respiratory tract of the carrier to the mucosal surfaces of the recipient. Supporting evidence of such transmission came from epidemiological studies of disease outbreaks such as with the SARS-CoV outbreak as well as experimental studies on aerosol dynamics.
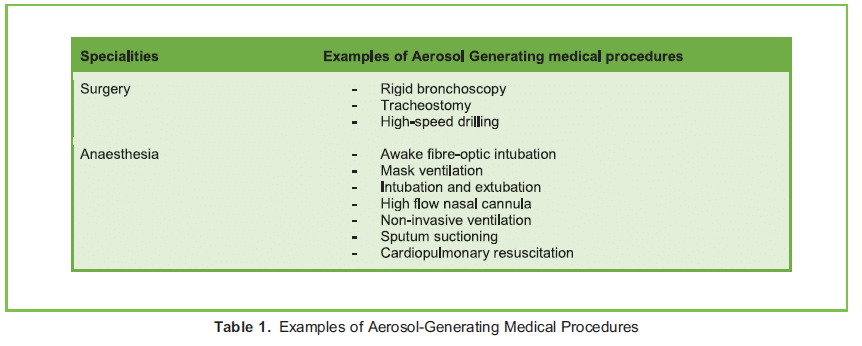
Aerosol-generating procedures (AGPs) are medical procedures that create aerosols in addition to those that the patient creates during regular breathing, coughing, sneezing and talking. They can produce both large and small droplets, and if done so in high enough concentration, may cause opportunistic airborne transmission of microbes that otherwise are not commonly spread by the airborne route (eg, SARS-CoV2, influenza). Examples of AGPs are shown in Table 1.3 It is important to note that aerosols are often generated as a mixture of small to large droplets. The distinction between droplet and airborne transmission should thus be viewed as a spectrum instead of 2 dichotomising entities. In summary, SARSCoV2 virus can be spread by direct and indirect contact, droplet and aerosol route, with rising evidence supporting possible airborne transmission.4
SURGICAL FACE MASKS
Purpose of Surgical Face Masks
A face mask is a mask that covers the user’s nose and mouth and may or may not meet fluid barrier or filtration efficiency levels. In contrast, a surgical mask is a loose-fitting, disposable mask that covers the wearer’s mouth and nose and creates a physical barrier to fluids and particulate materials. Contrary to common beliefs, it is designed to limit the expiratory spread of droplets from the wearer to the surroundings. However, an emerging systematic review suggests that the use of surgical face masks may prevent infected individuals from spreading respiratory pathogens to uninfected individuals.5 Whether widespread usage of surgical face masks should be implemented remains controversial, and further studies are needed.
Composition of Surgical Face Masks
Surgical masks are made up of multiple fabric layers, typically referred to as an SMS configuration or a 3-ply design. SMS stands for spunbond-meltblown-spunbond and describes the manufacturing technique of the 3 layers (Figure 1)6:
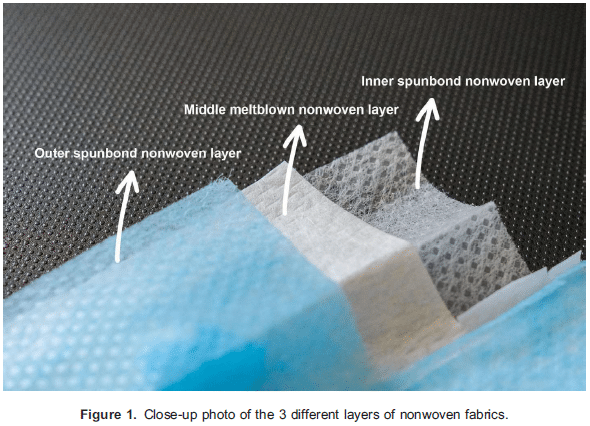
- Outer layer: nonwoven layer of spunbond polypropylene with hydrophobic repellent treatment
- Middle layer: filtering nonwoven layer of meltblown polypropylene
- Inner layer: nonwoven layer of spunbond polypropylene with hydrophilic surfactant treatment
Characteristics of these materials are as follows:
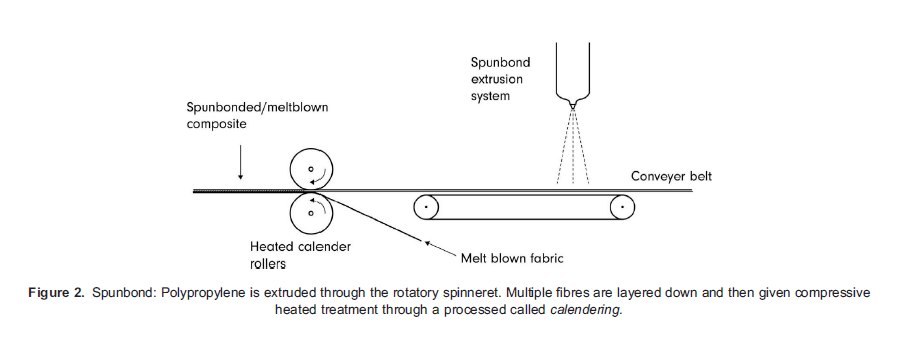
- Spunbond polypropylene: Polymers are extruded through a spinneret, forming a web from fine strands of polypropylene filament. The sheet of fabric then goes through calender bonding, in which it is compressed and heat-treated (Figure 2).
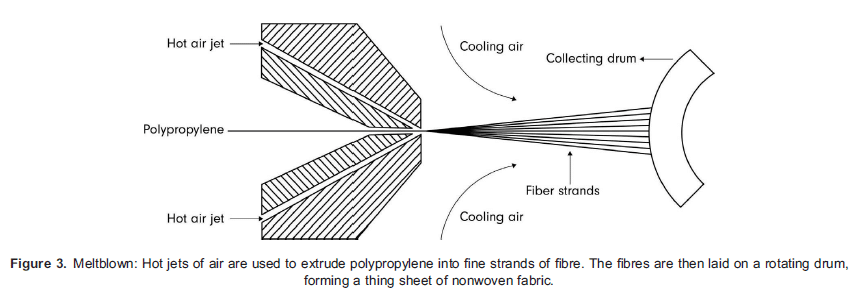
- Meltblown polypropylene: High-velocity hot air streams are used to extrude polypropylene polymers into even finer strands of filaments. As the filaments overlay, the fabric thickens to form the filtering layer (Figure 3).
- Spunbond fabric has good strength and durability as well as excellent moisture and temperature resistance. On the other hand, meltblown fabric has relatively weak tensile properties but excellent filtrating, wicking and barrier properties because of the smaller fibre and larger accumulated surface area. The technique of layering these 2 materials together is easy to do, inexpensive and results in a mask with good bacteria filtration efficiency and air permeability. With the addition of repellent and surfactant treatment, droplet transmission prevention is maximised.
- Besides polypropylene, alternative materials can be used to make nonwoven fabric such as polystyrene, polyethylene, polyesters and cellulose-based matter.
Evaluation and Classification of Face Masks
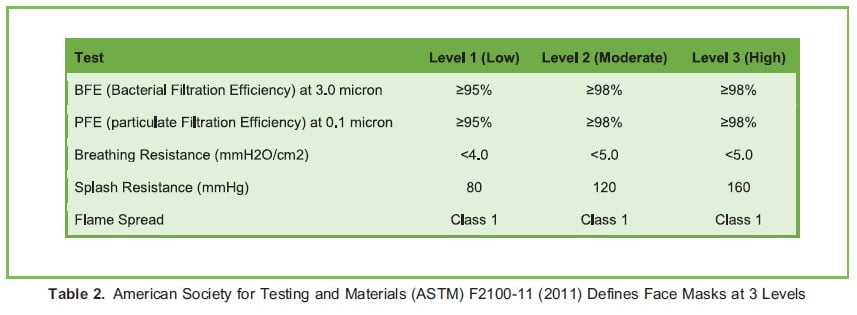
Once these nonwoven fabrics are made, trimmed and fashioned into a surgical face mask form factor, they are tested for the following criteria7:
- Bacterial filtration efficiency: Aerosols containing Staphylococcus aureus bacteria are propelled at the masks at a controlled volume and rate. A minimum 95% filtration efficiency rate is required.
- Particle filtration efficiency: Aerosols of polystyrene microspheres size from 0.1 to 5 lm are sprayed at the masks to ensure the mask can filter particles of various sizes. The percentage indicates the mask filtration efficiency rate for particles.
- Breathing resistance: This is tested by blowing air at the mask and measuring the difference in air pressure on both sides of the mask. The unit of measure is mmH2O/cm2.
- Splash resistance: Synthetic blood is forced onto the mask to ensure the liquid cannot penetrate and contaminate the wearer. Test pressure similar to human blood pressure is used.
- Flammability: All masks should be flame resistant to prevent fire hazard.
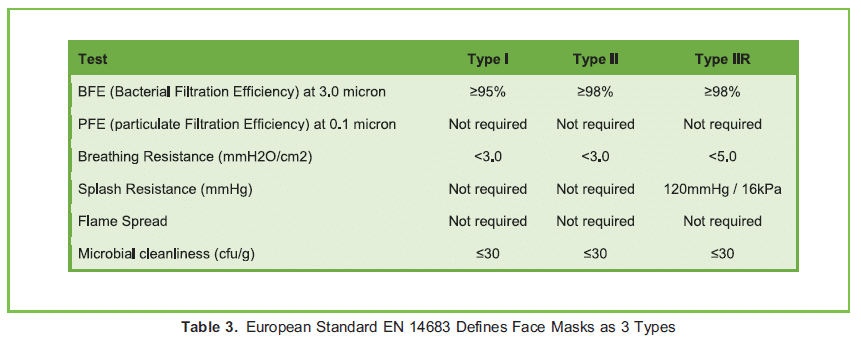
- Allergenicity: Face masks should be tested to an international standard (ISO 10993-5,10) for skin sensitivity.8
- Microbial cleanliness: Face masks are made in a clean, controlled environment to keep the total viable microbial count (cfu/g) on the surface as low as possible.
Based on the results from the above tests, the masks are classified into different levels. Tables 2 and 3 describe the classifications according to American and European standards, respectively.
FILTERING FACEPIECE RESPIRATORS
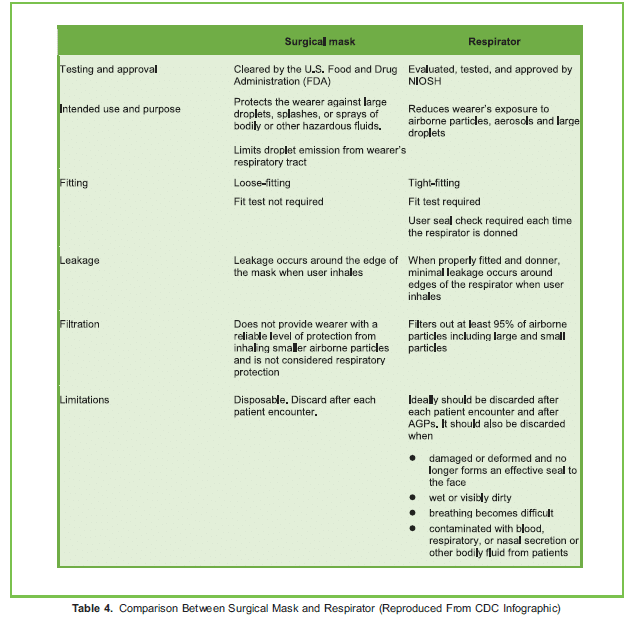
A filtering facepiece respirator (FFR) is a respiratory protective device intended to cover the nose and mouth of the wearer to help reduce wearer exposure to pathogenic biological airborne particulates. In contrast to a surgical mask, it is designed to achieve a close facial fit and efficient filtration of airborne particles.
Makeup of Respirators
Disposable respirators such as the commonly used N95 or FFP2 are generally made up of 4 layers.9
- Outer layer: hydrophobic nonwoven layer of spunbond polypropylene with repellent treatment.
- Prefiltration layer: nonwoven material that is needle punched together and thermally treated. It forms a thicker, stiffer layer, which can then be moulded to desired shapes. Some manufacturers use cellulose-based material for this layer, which has different implications when considering decontamination (see below).
- Filtration layer: polarised nonwoven layer of meltblown polypropylene, which determines the filtration efficiency of the respirator.
- Inner layer: hydrophilic nonwoven layer of spunbond polypropylene with surfactant treatment.
Although the manufacturing process may be similar to that of surgical masks, respirators have higher filtering efficiency with a form factor that allows for a better seal around the face (Table 4). They are designed to protect the wearer from airborne particles and finer respiratory droplets. They are especially recommended when a high concentration of infective aerosols and droplets is anticipated.
Respirator Classification
Respirators are classified according to the following:
- Barrier characteristics and filtration efficiency;
- Degree of oil resistance of the filter;
- How they are designed to be worn.
Barrier Characteristics and Filtration Efficiency
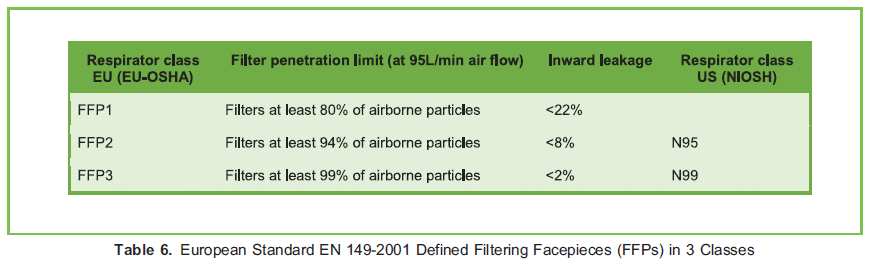
Respirators undergo a series of tests to determine classification and certification. Testing criteria are similar across different standardising bodies but may vary slightly in their cutoffs. The most commonly used FFR standards are the American NIOSH-42CFR84 (Table 5) and the European EN 149-2001 (Table 6).9 The 2 most recognised FFRs certified by these 2 standards are the N95 and FFP2. The Chinese manufactured KN95 (GB2626-2006) is gaining in popularity because of rising demands, but
further testing may be warranted to establish its reliability.10
Degree of Oil Resistance of the Filter
Series
The American National Institute for Occupational Safety and Health (NIOSH) classifies respirator filters into 3 series based on oil resistance:
- N series filter solid and water-based particulates;
- R series are resistant to oil;
- P series are oil proof.
Water-based particulates are responsible for disease transmission; therefore, the N series is more appropriate in most health care settings.
Evaluating Respirators
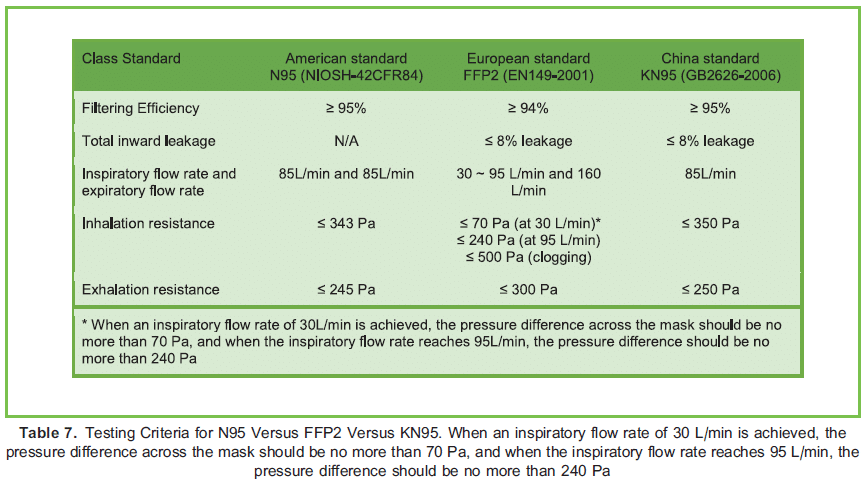
Prior to testing, respirators are conditioned at 388C at 85% relative humidity for 24 hours. After conditioning, they are tested for the following criteria11 (Table 7):
- Filtrating efficiency: Charge-neutralised sodium chloride aerosol with a median size of 0.3 lm is used to test for particle penetration. Filtration efficiency is reported in terms of the percentage of particles filtered.
- Leakage: Inward leakage is assessed, as it should be as low as possible to prevent exposure to airborne diseases. An inward leak of 8% or lower is acceptable. However, this is required only by the European and Chinese standards.
- Flow rate: The respirator is assessed for fast air movement in and out so that the user can wear with ease even with heavy/ fast breathing. A flow rate of about 85 L/min is required.
- Inhalation and exhalation resistance: Breathing resistance is assessed and should be kept as low as possible at a given flow rate of air to minimise the work of breathing.
Throughout the test, the filtration ability of the respirators must stay above their certification class level at all times. In addition to
these criteria, the respirators should be flame resistant, hypoallergenic and resistant to fluids.
The terms surgical N95 respirators and medical respirators refer to NIOSH-approved N95 respirators that have also been validated by the US Food and Drug Administration (FDA) to be used as surgical masks at medical facilities. They are recommended only for health care professionals who need protection from both airborne and fluid hazards, in comparison with other ‘industrial’ N95 respirators. If high-velocity splashes, sprays, or splatters of blood or body fluids are anticipated, then standard N95 respirators should be used in conjunction with face shields. Face shields prevent surface contamination and soiling of the respirators but do not add to the filtration. Some models of respirators have exhalation valves. These are designed
to reduce expiratory airflow resistance and contribute to the comfort of prolonged mask wearing. However, they do not protect others from potential exposure if the person wearing the mask is infected.12
How the Respirators Are Designed to be Worn by Health Care Workers
NIOSH subdivides respirators into 3 categories depending on how the filters are designed to be worn by health care workers (Table 8).
- FFRs: These are relatively inexpensive and lightweight. They are disposable, do not affect mobility and require no maintenance or cleaning if disposed after a single use. They do not provide eye protection, and a suboptimal seal is an issue for individuals with facial hair.
- Elastomeric facepiece respirators (EFRs) with or without eye coverage: These provide higher filtration efficiency against airborne pathogens and can be used for many hours, depending on the manufacturers’ specifications. However, they are bulky and may hinder mobility and communication. The Centers for Disease and Control and Prevention (CDC) has raised concerns regarding the use of respirators with valves in surgical settings, as droplets spreading through their expiratory valves is still a potential risk. Some advise wearing a standard surgical mask over these respirators to minimise this risk.13
- Power air-purifying respirators (PAPRs): These devices provide full head coverage including hair, eyes, face and mouth (and neck coverage with some models). They provide a better seal for individuals with facial hair, missing teeth, or facial scars.
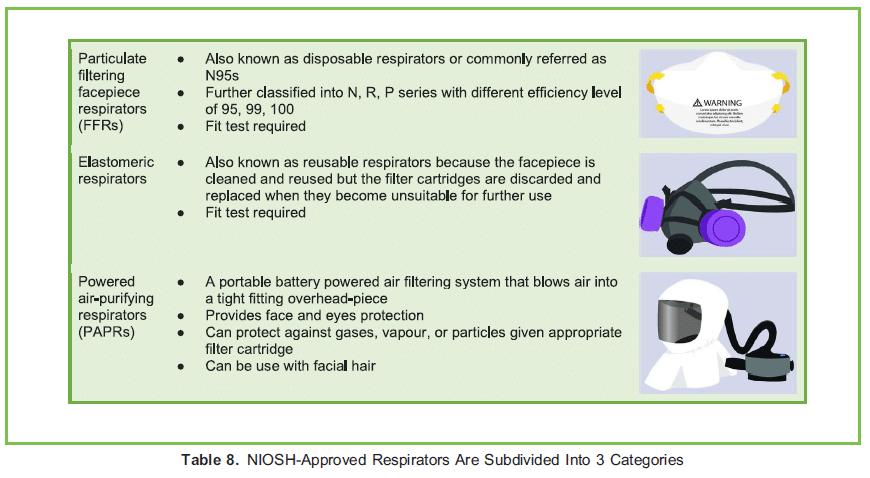
Compared with N95 respirators, PAPRs provide superior filtration efficiency, lower breathing resistance and higher comfort level during prolonged usage despite the added weight of the headpiece, battery and pump. However, they are more expensive, the battery requires charging and regular maintenance is required to ensure all connections remain secure. Despite initial concerns, more recent studies have shown that PAPR utilisation in the operating room does not increase particulate transfer to the surgical field, unlike EFRs.13
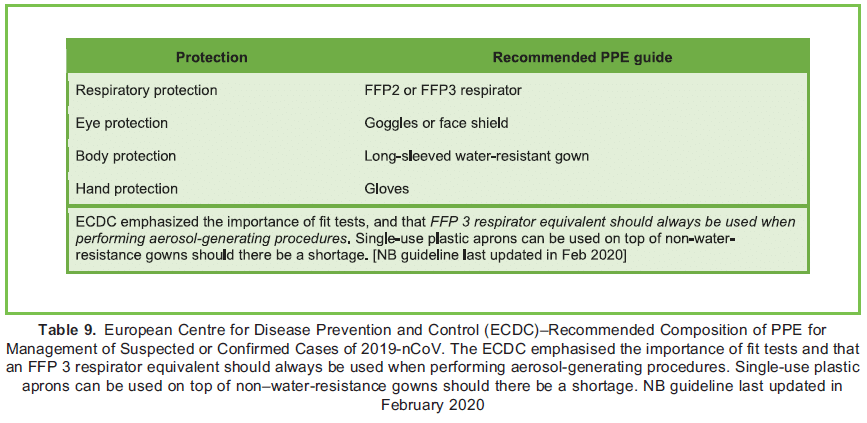
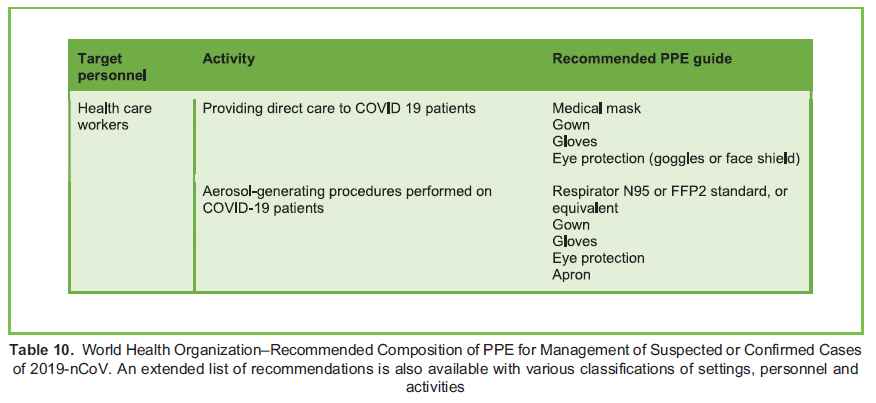
RECOMMENDATIONS FOR COVID-19
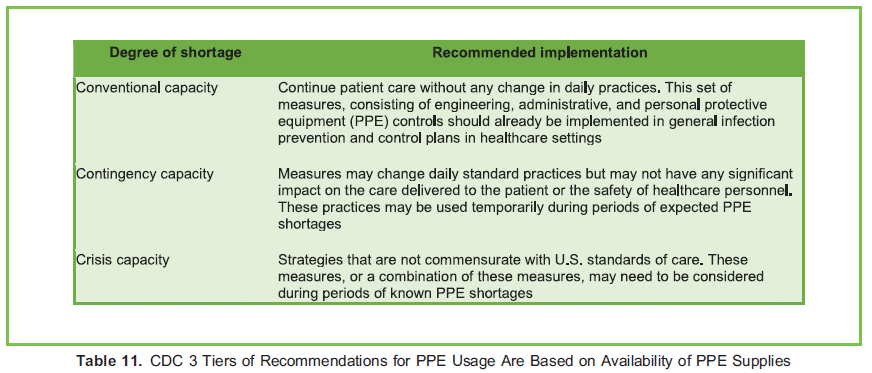
Tables 9 and 10 summarise the European Centre for Disease Prevention and Control (ECDC) and the World Health Organization (WHO) recommendations for PPE that health care providers should wear when caring for COVID-19 patients. Table 11 summarises CDC’s PPE recommendations for health care providers while caring for COVID-10 patients. In contrast to the ECDC and WHO recommendations, the CDC recommendations take supply availability into consideration.14
Extended Use and Limited Reuse of Respirators
Because of dramatically increased demands for N95 or equivalent (FFR), many countries have adopted strategies to conserve respirators.15 The CDC guidelines include a variety of approaches to conserve supplies while safeguarding health care workers during times of shortage. The most basic strategy includes extended use and limited reuse.
Extended use refers to the practice of wearing the same FFR continuously for repeated close contact with several patients, without removing the respirator between patient encounters. It may be implemented when the same respiratory pathogen infects multiple patients and the patients are located together in dedicated wards. Health care workers may be required to wear the same FFR for a few hours until they can remove it, such as at mealtime or the end of a shift.
Limited reuse refers to the practice of using the same FFR for multiple encounters with patients but removing it (‘doffing’) in between patient encounters. The FFR is stored in between encounters and placed on again (‘donned’) prior to the next encounter with the same or different patient. The number of times the same FFR is reused should be restricted and it is often referred to as ‘limited reuse.’
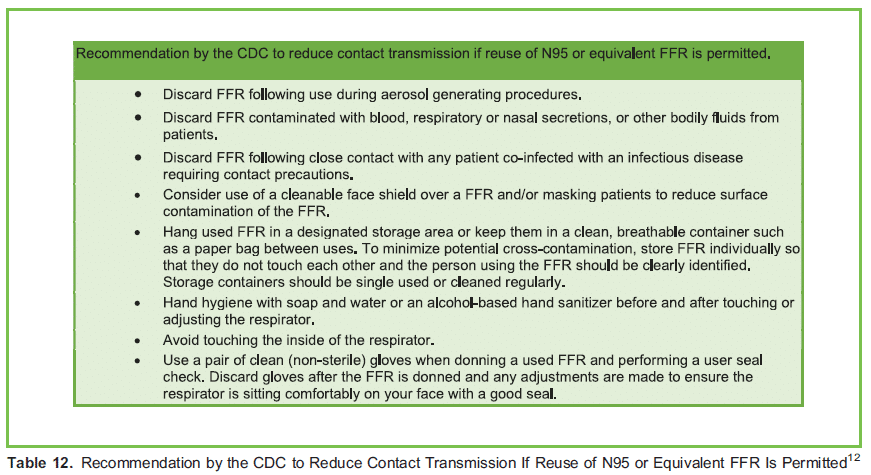
Although extended use and limited reuse are being practiced out of necessity in many countries during the COVID-19 pandemic, NIOSH specifies that such practice should still take into account FFR hygiene, damage and breathing resistance. FFR should still be replaced whenever they are noticeably damaged or soiled or there is difficulty breathing due to increased resistance. Table 12 lists some steps recommended by the CDC to reduce contact transmission if reuse of N95 or equivalent FFR is permitted.16
Decontamination and Reuse of FFRs
The US FDA does not recommend disposable N95 respirators to be reused or shared.17 However, FFR decontamination and reuse may need to be considered during a crisis, such as with the COVID-19 pandemic, to ensure continued availability. As a result, the CDC and N95 DECON group suggest 3 potential decontamination processes: vaporous hydrogen peroxide, ultraviolet germicidal irradiation and moist heat.18,19
Regardless of which method is used, an individual FFR should be clearly labelled with the user’s name and stored individually. A decontamination log should also be maintained so the FFR can be identified and returned to its owner.20
Vaporous Hydrogen Peroxide
Hydrogen peroxide (H2O2) vapor and plasma decontamination is an established industrial decontamination method used in hospitals and health care and pharmaceutical industries.21 Hydrogen peroxide vapor (wet HPV or dry VHPe) and hydrogen peroxide gas plasma (HPGP) inactivate highly resistant pathogens, including nosocomial bacterial spores and viruses. In a recent study, it was found to inactivate SARS-CoV-2 on all N95 mask types tested.22
A possible concern for its use is that harmful concentrations of hydrogen peroxide may remain on the mask for days after decontamination.23 In addition, repeat decontamination cycles can lead to deformation of the masks and affect filtration efficiency.24
The Bioquell Battelle Decontamination System is an HPV system for decontaminating N95 masks. It received emergency use authorization from the FDA on 28 March 2020 and can be used for up to 20 cycles without degrading filter quality or straps for FFR 3M model 1860.25 It is important to note that HPV, VHPe, and HPGP are not compatible with cellulose, which is absent in 3M model 1860 N95 masks but may be present in other FFR such as 3M model 1870 and 1870þ masks. The presence of cellulose is an important consideration in the adoption of VHP-based strategies, because hydrogen peroxide degrades cellulose-based products (eg, cotton, present in some head straps or some FFR layers). In addition, cellulose absorbs hydrogen peroxide, and this can lower hydrogen peroxide vapor concentration in the devices, affecting the sterilisation performance.
Ultraviolet Germicidal Irradiation
Ultraviolet germicidal irradiation (UVGI) uses short-wavelength ultraviolet, mainly ultraviolet C (UVC), to kill or inactivate microorganisms by disrupting their DNA and vital cellular functions. UVC has the shortest wavelength (100 to 280 nm) and greatest energy compared with ultraviolet A and ultraviolet B. UVGI is a promising method, but the disinfection efficacy is dependent on the following factors.26,27
Dose (Energy Level and Duration of Exposure)
UVGI at 1 J/cm2 was found to be effective in inactivating various viruses, including MERS-CoV and SARS-CoV, at the exterior surface of the face mask from 99.9% to .99.999% in about 60 seconds.26 A higher dose of UVC may improve the effectiveness in terms of penetration but may degrade the materials and affect the fit for reuse.
Shadow Effects
The presence of shadows indicates the blocking of ultraviolet (UV) light, thus lowering the decontamination efficiency at the unexposed area. This shadow effect is particularly relevant for masks that have horizontal ridges or folding across the front of the facepieces.26 Multiple UV lamps are required to facilitate sufficient exposure from different directions. In addition, cosmetics and sunscreen left by the wearer on N95 may reduce decontamination efficacy.
Mask and Strap Composition
The FFR facepiece and the straps vary in design (eg, material, thickness, shapes and elasticity), which may influence the effectiveness of decontamination. Because UV light primarily acts on surfaces, absorption of the viral inoculum below its surface could potentially shield the virus from exposure, hence limiting the UVGI decontamination efficiency. Hydrophilic material tends to absorb both mucin and virus, thus affecting the UVGI effectiveness.26
Moist Heat
With this method, warm moist heat (60-758C at 80% relative humidity) for at least 30 minutes acts as a biocidal decontamination process. This process has been found to be preferred over dry heat sterilisation. Moist heat is more effective in killing microorganisms through protein denaturation and less likely to cause degradation in filter performance.27
Moist heat has been shown to effectively disinfect FFRs contaminated with H1N1, although no data on similar inactivation in case of coronaviruses, other bacteria and mould spores has been published. Although the CDC has released guidelines on the use of moist heat for decontaminating N95 or equivalent FFRs, this method has not been validated by the FDA and its use should be used cautiously.
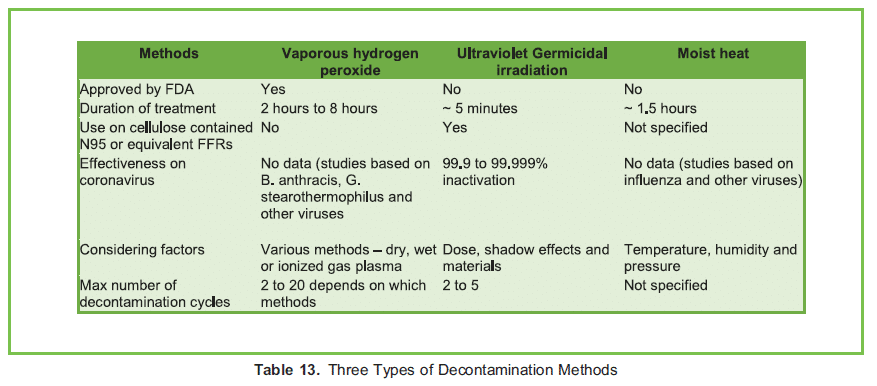
Table 13 summarises important characteristics of the various proposed decontamination processes.
CONCLUSION
In general, face masks used in the health care settings can be divided into 2 groups: surgical face masks and FFRs. Surgical face masks are loose fitting and are used widely to prevent the spread of droplet-transmissible diseases such as SARS-CoV-2. They are made up of nonwoven materials and tested against strict standards. On the other hand, respirators are tight fitting and have higher filtering efficiency and are designed to protect the wearer from droplets as well as airborne particles. They can be found in the forms of N95, EFRs, or PAPRs. Because of limited supplies and dramatically increased demands, decontamination and reusing FFRs may be needed. Current recommended methods for decontamination include UV germicidal irradiation, vaporous hydrogen peroxide and moist heat decontamination. Familiarization with the various types of potentially AGPs and choosing the most appropriate level of face mask based on exposure risk is recommended.
REFERENCES
1. Access Continuing Education, Inc. Element II: the modes and mechanisms of transmission of pathogenic organisms in the healthcare setting and strategies for prevention and control. https://www.accesscontinuingeducation.com/ACE1000-10/c2/index.htm. Accessed April 4, 2020.
2. Van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARSCoV-1. N Engl J Med. 2020;382(16):1564.
3. Tang C, Chan A. Perioperative management of suspected/confirmed cases of COVID-19. ATOTW. 2020;421:1-13
4. Wilson NM, Norton A, Young FP, Collins DW. Airborne transmission of severe acute respiratory syndrome coronavirus-2 to healthcare workers: a narrative review. Anaesthesia. 2020;75(8):1086-1095.
5. Cowling BJ, Zhou Y, Ip, Leung GM, Aiello AE. Face masks to prevent transmission of influenza virus: a systematic review. Epidemiol Infect. 2010;138:449-456.
6. Science Direct. Melt blown process. https://www.sciencedirect.com/topics/engineering/melt-blown-process. Accessed April 5, 2020.
7. Chellamani KP, Veerasubramanian D, Vignesh Balaji RS. Surgical face masks: manufacturing methods and classification. J Acad Indust Res. 2013;2(6):320-324.
8. ISO 10993-5,10 Biological evaluation of medical devices. Part 10: Tests for irritation and skin sensitization. https://www.iso.org/obp/ui#iso:std:iso:10993:-5:ed-3:v1:en. Accessed April 11, 2020.
9. Centers for Disease Control and Prevention. Standards for respirators with chemical, biological, radiological, and nuclear protection. https://www.cdc.gov/niosh/npptl/RespStds.html. Accessed April 7, 2020.
10. International Respirator Assessment Request. https://www.cdc.gov/niosh/npptl/respirators/testing/NonNIOSH.html. Accessed July 16, 2020.
11. 3M. Comparison of FFP2, KN95, and N95 and other filtering facepiece respirator classes. https://multimedia.3m.com/mws/media/1791500O/comparison-ffp2-kn95-n95-filtering-facepiece-respirator-classes-tb.pdf. Accessed April 26, 2020.
12. Vincent M, Edwards P. Disposable surgical face masks for preventing surgical wound infection in clean surgery. Cochrane Database Syst Rev. 2016;4(4):CD002929.
13. The use of personal protective equipment by anesthesia professionals during the COVID-19 pandemic. https://www.apsf.org/news-updates/the-use-of-personal-protective-equipment-by-anesthesia-professionals-during-the-covid-19-pandemic/. Accessed August 2, 2020.
14. Centers for Disease Control and Prevention. Crisis capacity strategies (during known shortage). https://www.cdc.gov/coronavirus/2019-ncov/hcp/respirators-strategy/index.html. Accessed April 6, 2020.
15. ECRI. Safety of extended use and reuse of N95 respirators. Clinical evidence assessment. https://www.elsevier.com/__
data/assets/pdf_file/0006/997863/COVID-ECRI-N95-Respirators_2020-03.pdf. Accessed April 8, 2020.
16. National Institute for Occupational Safety and Health. Recommended guidance for extended use and limited reuse of N95 filtering facepiece respirators in healthcare settings. https://www.cdc.gov/niosh/topics/hcwcontrols/recom
mendedguidanceextuse.html. Accessed April 8, 2020.
17. US Food and Drug Administration. Coronavirus (COVID-19) update: FDA issues second emergency use authorization to decontaminate N95 respirators. 2020. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-up
date-fda-issues-second-emergency-use-authorization-decontaminate-n95. Accessed April 8, 2020.
18. Centers for Disease Control and Prevention. Decontamination and reuse of filtering facepiece respirators. https://www.
cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/decontamination-reuse-respirators.html. Accessed April 8, 2020.
19. N95 Decon group. COVID N95 decon and reuse. https://www.n95decon.org/publications. Accessed April 8, 2020.
20. N95 respirators, surgical masks, and face masks. https://www.fda.gov/medical-devices/personal-protective-equipmentinfection-
control/n95-respirators-surgical-masks-and-face-masks. Accessed May 15, 2020.
21. Viscusi D, Bergman M, Eimer B, et al. Evaluation of five decontamination methods for filtering facepiece respirators. Ann Occup Hyg. 2009;53(8):815-827.
22. Oral E, Wannomae K, Connolly R, et al. Vapor H2O2 sterilization as a decontamination method for the reuse of N95 respirators in the COVID-19 emergency. medRxiv. 2020;04.11.20062026.
23. N95 Decon. Technical report for H2O2-based N95 reuse risk management. N95 Decon research document. https://static1.squarespace.com/static/5e8126f89327941b9453eeef/t/5e86d8be51cbbf1de3b3688e/1585895615567/200402_N95DECON_HPV_technicalreport_v1.2_final.pdf. Accessed April 8, 2020.
24. RIVM. Reuse of FFP2 masks. National Institute for Public Health and the Environment. https://www.rivm.nl/en/documenten/reuse-of-ffp2-masks. Accessed April 8, 2020.
25. Battelle. FDA letter of approval (3/28/2020) for emergency use authorization for the Battelle Decontamination System, an HPV system for decontaminating N95 respirators. https://www.battelle.org/inb/battelle-critical-care-decontamination-system-for-covid19. Accessed April 8, 2020.
26. Mills D, Harnish D, Lawrence C, et al. Ultraviolet germicidal irradiation of influenza-contaminated N95 filtering facepiece respirators. Am J Infect Control. 2018;46(7):e49-e55.
27. Lore M, Heimbuch B, Brown T, et al. Effectiveness of three decontamination treatments against influenza virus applied to filtering facepiece respirators. Ann Occup Hyg. 2012;56(1):92-101.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/