Patient Safety

KEY POINTS
• Distractions are ubiquitous in the operating room and may be associated with negative outcomes.
• Some distractions have a positive impact on teamwork and may reduce boredom and increase awareness.
• Several strategies could be employed to reduce distractions and enhance patient safety.
• “Sterile OR rule” should be applied in critical situations that demand undivided attention.
INTRODUCTION
It’s 7 PM, your fifth case of the day, and your beeper rings about the lab results of the next patient you will be anesthetizing. The nurse is opening the instrument box, and an instrument falls to the ground. The surgeon is complaining about time because it is almost dinner and the rock music chosen by the surgical resident is raging. You are preparing to intubate a patient after induction, and suddenly, the monitor alarms loudly because the patient is hypotensive. How many can relate to this situation? Certainly, being distracted or out of focus in this situation is not only possible but likely.
The American Society of Anesthesiologists (ASA) issued a “Statement on Distractions” that states that “an essential aspect of the safe anaesthesia care environment includes managing the working environment to limit, and when possible to eliminate distractions that reduce appropriate attention to the patient. Equally important is the harmful effect distractions have on anaesthesia providers, resulting in higher mental stress and poorer teamwork.”1 Therefore, an understanding of the multiple distractions that occur in the operating room (OR) is essential to create strategies to avoid the impact of these on patient safety.1,2
Why do we tolerate smartphones or tablets in the OR? How many times did you feel distracted in the last week and why? Are these affecting our care of the patients? Would the patients be better served if we diminished distractions? These are some of the questions we will try to answer. In addition, we will provide some strategies to deal with and mitigate distractions as well as discuss their impact on patient care.
DISTRACTIONS IN THE OR: DEFINITION AND EPIDEMIOLOGY
Currently, there is no single, widely accepted definition of distractions, but those that exist have in common that distractions are elements that redirect attention to an action or to different objects unrelated to the primary task at hand, in this case, the patient care.3-5 These moments are frequent and sometimes unpredictable and lead to loss of “the global picture,” decreased vigilance and situational awareness (SA), cognitive disengagement and potentially causing a discontinuation or switch of tasks.6-8 Interruptions to workflow are associated with increases in error and procedural failures.4 Distractions also increase cognitive load, perceived stress and fatigue and are associated with a more negative mood.5
Depending how we classify or which ones we are searching, distractions are nearly ubiquitous and an integral part of anaesthetic practice, with some studies reporting an incidence of 1 every 10 minutes.3,7,9 Anaesthesiology and the OR environment are com- plex, dynamic and highly demanding of attention. Therefore, a deviation of attention could have an impact on our focus to detail, the ability to promptly respond to patients’ needs and, in the end, have an impact on patient safety and outcomes.1,6,10
Distractions are associated with a negative impact on patients, with at least 5% of human error in the OR related to distractions.3 The ASA Closed Claim database reports 10 (of 5822) injury claims related to distraction in the OR.6 However, the real harm of these interrupting moments is difficult to estimate due to the complex and multifaceted nature of the OR environment.3
Although some distractions may be inevitable, such as a surgical instrument falling to the ground, and a “sterile cockpit” environment seems impossible, there are some tasks or surgical procedures that demand full focus and undivided attention. Therefore, distractions should be actively avoided to improve patient safety.7,9
ATTENTION, VIGILANCE AND SA IN THE OR
Attention refers to the cognitive processes that allow us to maintain focus on certain tasks under varying levels of environmental distractions.3 Attention span is the length of time concentrating on a task before diverting to another stimulus.3 Vigilance is the capacity to detect and respond to changes in a patient’s physiological condition.11
SA, simply put, could be defined as “knowing what is going on” or, more precisely, as the perception and comprehension of the elements in the environment about the past (eg, medical history), present (eg, monitors) and the projection of their future status.8 When SA is lost, patients could be at risk, as shown in one study in which 74% of 266 claims of death or brain damage were related to lack of SA.12 SA is a core element in anaesthesia decision making, teamwork, task management and patient safety.7,12,13 Each member of the OR team has a responsibility to their colleagues and to the patient to maintain SA, and maintaining the team’s SA is a fundamental task of the team leader.8
Highly interrupting OR environments may weaken cognitive alertness, SA and memory processes that are important to keep focus and to perform tasks effectively.7 Multitasking implies some diversion of attention from a single task, and switching between tasks implies higher cognitive demand, referred to as “switch cost,” which lowers response time and increases stress and the likelihood of error.2-6 The longer we are disengaged, the more difficult it is to re-engage, with more latency of response.4
Some factors explain the occurrence of distractions in the OR, such as the repetitive nature of some contexts, the comfort with the procedure and sequence of future events, boredom and complacency.4 In routine surgeries where workload is low, because critical moments are rare, it can lead to relaxation and the perception that a quick break is harmless.4,8,9 However, we can miss critical clues while bored just as easily as when we are focused on a particular event, such as sudden marked blood loss.8
Nevertheless, anaesthesia work does not imply continuous beat-to-beat attention to the patient’s vital signs, and an interruption in itself does not always pose a risk to a patient’s safety. Usually, anaesthesiologists glance at monitors intermittently, spending less than 5% of time looking at them.11 Prolonged periods of vigilance tasks (such as in long routine cases with small fluid shifts and small blood loss) may lead to boredom that also harms performance and, just like driving in monotonous, long and lonely roads, may also impair vigilance and result in performance that declines over time.11 Therefore, some interruptions may be, in certain con- texts, essential for proper OR functioning. Case-irrelevant conversations (CIC) may reduce boredom and social tension, enhance teamwork, increase vigilance during monotonous or long work, or help to maintain awareness and vigilance, such as when we are tired or during night shift.7 Small mental breaks could help to keep focus and improve performance.5,11 A limited number of studies report that self-initiated distractions (such as reading), occurring during stable portions of cases, did not impair vigilance (measured by time response to an alarm light) and were associated with lower workload, but not with adverse events.5 Therefore, self-initiated distractions are thought to be less problematic than external distractions.5 However, the effectiveness of this strategy depends on how mentally absorbing they are, since more mentally engaging distractions (such as reading scientific articles) can interfere with performance.5
CLASSIFICATION AND TYPES
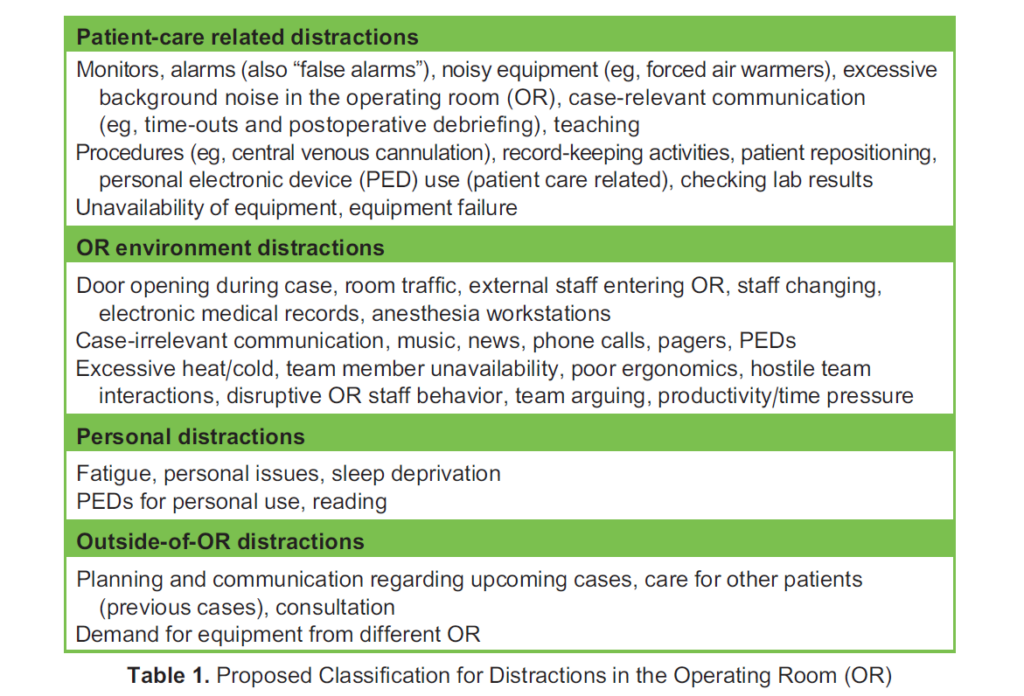
A classification of distractions in the OR is proposed in Table 1, combining the available literature in different categories, based on the source of distraction.1,3,4,6,7,9,10 Absolute and relative frequencies of distractions varied vastly between studies, but some of the most common were auditory, people entering and leaving the OR, equipment and personal electronic devices (PEDs).7,9,10 Distribution throughout different phases of surgery also varied. Some studies reported distractions being more frequent in the early stages of surgery, including induction.3,7 Others reported that self-initiated distractions happen nearly only in the maintenance phase.3,5 Distractions increase in those having general anaesthesia and longer cases.4 Longer OR procedures are also associated with team member rotations, lunch periods and breaks, which could also be a factor in diversion of attention.7,8
Auditory distractions (such as CIC, music, sudden drop of instrument, opening or closing trays) are generally negative.3,10 However, music could be a double-edged sword.10 On one hand, it could have a calming effect, but on the other hand, the volume, intensity and choice of music could have different impacts on different team members and should be taken into account. Higher volumes may negatively affect the ability to hear the alarms and may hamper important team communication.10
Intense acoustic distractions in the OR (an area of paramount communication and concentration) are associated with higher workload and stress.9,10 Noise impairs concentration, task performance, the ability to detect alarms and communication between OR staff. Even a momentary misunderstanding, such as a misperception of one drug dose to be administered, could have negative consequences.1,13 The average OR noise level is 66 dB (equivalent to normal conversations) but can be greater than 100 dB (equivalent to a motorcycle sound), particularly during orthopaedic and neurosurgical procedures.3 Studies found induction and emergence as the loudest periods, which are two of the moments requiring higher focus from the anaesthesia team.1
Anaesthetic equipment alarms play a critical role in raising awareness to parameters that may be outside a safe range.1 However, alarms could be disturbing and affect our focus on our surroundings if they are constantly beeping. Most (85%–99%) alarms do not require clinical intervention.1,6 This high frequency of false alarms could also be distracting and lead to a cycle of alarm fatigue.1,6 Ideally, alarms should be adjusted to the patient’s specific needs.1 Nevertheless, in critical situations, the same alarm constantly ringing could affect our ability to think.
The non-OR anaesthesia environment may present different or amplified challenges when it comes to distractions. Distractions encountered there may include a less familiar environment, unstandardized processes, unfamiliar team tasks and communication challenges.6 Therefore, staff working in these areas should have a heightened awareness of these new or different distractions.
BENEFITS AND HARMS OF PERSONAL ELECTRONIC DEVICES (PEDS)
Technology makes our lives easier and more efficient and helps solve problems.4,13 PEDs such as smartphones, smartwatches and tablets are now part of our daily routine and are very frequently used in the OR.13 PEDs can be used for many patient-related tasks such as accessing patient information, improved learning, consultation of guidelines or checklists, calculating drug doses and calling for help.1,2,4 Therefore, appropriate and selective use of PEDs may improve decision making, adherence to guidelines and, ultimately, patient care.2,13,14
However, PED use could be intrusive and addictive. Some evidence shows that electronic distractions worsen judgment and performance and affect teamwork by diverting from collaboration, communication and teaching.13 Research on the impact on clinical outcomes is still sparse, however.3,13
Unfortunately, PED use is not always restricted to noncritical phases of surgery. Moreover, distracting notifications from PEDs may occur at unexpected times.4,10 Although more relevant during critical periods of a case, even during noncritical phases of surgery, important information may go unnoticed with only a few seconds of inattention, which could affect the patient.4
Although PEDs have their benefits for medical practice, the OR team must have good judgment about choice, timing and duration of their use.5 Ideally, their use should be limited to patient care–related activities and kept to a minimum.1,11
IMPACT OF DISTRACTIONS ON TEAMWORK
OR teams are broadly heterogeneous, combining different personalities, ages, backgrounds and roles within the team.2 Therefore, individuals probably have different views and perceived impact about different distractions.2 Good teamwork and team dynamics are of great importance to patient care, as poor teamwork predisposes to errors.7,10 Distractions in the OR may actually play a role in improving teamwork.
Distractions may present either a positive or negative impact on OR teamwork. CIC, which usually occurs when workload is low, has positive influences of enhancing good working relationships, reducing monotony and relieving stress and pressure.7,9 Establishing meaningful relationships with the team may enhance relevant communication and team management throughout the case. However, it is not appropriate in all situations, as complex and challenging phases of the case need full attention, and CIC could impair effective case-relevant communication and team performance. Therefore, carefully chosen strategic moments for CIC could be beneficial.7 If the anaesthesiologist is engaged in personal distractions, though, such as a PED, they interact less with the remaining team and are less aware of their needs.
Other types of distractions, such as equipment failures and environment disruptions, have a negative impact on OR team- work.7 In these situations, team conflict management may be necessary, as a dysfunctional work environment increases stress, impairs collaboration and reduces productivity.7
STRATEGIES TO MITIGATE DISTRACTIONS
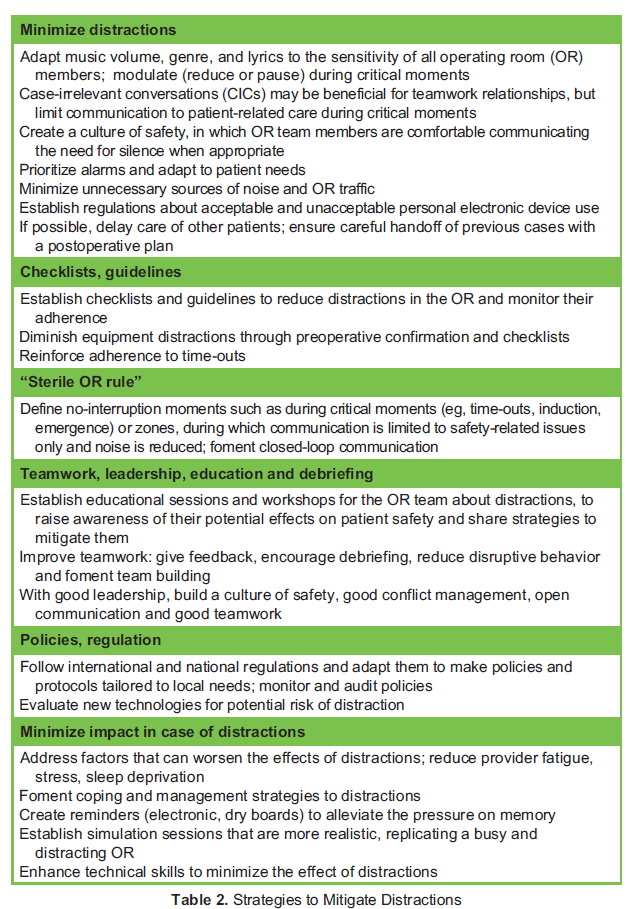
Efforts should be made to diminish unnecessary distractions while maintaining effective communication and teamwork.7 Managing distractions is a skill that comes with experience, with more senior anaesthesiologists dealing better with these than younger ones.3,11,14 In Table 2, we focus on some strategies to mitigate distractions.
Of particular relevance is that strategies should be adopted by the team as a whole. Therefore, promoting educational sessions regarding distractions and their impact is essential to encourage a change in culture aimed at improving patient safety.3
STERILE COCKPIT RULE
Airplane pilot distractions have resulted in disastrous accidents, leading to the creation of the “Sterile Cockpit Rule” by the Federal Aviation Administration.3,13 In addition, pilots have training and simulation practices to manage distractions in the cockpit.3 Once more, we can learn from other industries and adopt a similar strategy to limit OR distractions and probably enhance patient safety.3
A Sterile Cockpit Rule implies being fully mentally engaged in safety-critical moments of the flight (eg, ground operations, take- off, landing) without distractions. During safety-critical moments, no flight crewmember may engage in any activity that could distract another member from the performance of their tasks.3 In addition, flight crew cannot use PEDs unless it is a safety- related issue or related to the task at hand.3,14 Some industries, such as nuclear power, do not allow PEDs while on shift.6
A similar model could also apply to anaesthesia, such as a “Sterile OR Rule”.9 During critical phases of the surgical procedure (eg, time-outs, induction, critical surgical dissections, surgical counts, emergence), a no-interruption zone could be implemented in which nonessential conversations, noise and activities are prohibited.4 Bear in mind that during the maintenance phase, critical moments could also occur in an unpredictable fashion, so this rule could also be applied in those moments.3
One study implemented a “Distraction Free Induction Zone,” with the aim to reduce unnecessary conversations, loud noises
and music in paediatric ORs. To accomplish this, a quality improvement project was initiated in which several interventions were implemented and tested.13 Distractions during induction decreased from 61% to <15% in 6 months. A point to be noted is that OR team engagement and empowerment were essential for the success of this strategy.3,13 This kind of project could be expanded to other environments.
Standard scanning of monitors after a disruption of attention can avoid errors. In aviation, cockpit instrument scanning is part of the training and critical to safety, as pilots are instructed to scan the visual field in 108 increments for 1 second each to detect dangers.3 A similar approach may be used to scan anaesthesia monitors.3 Each time that we reengage in the case, we scan monitors in a systematic and repeatable pattern, similar to aviation with 108 increments or as one would perform a primary survey in a trauma patient (ABCDE: airway, breathing, circulation, drugs, everything else).
The intensity and impact of distractions depend on various factors: phase of the surgery, context, patient morbidity and the personal role on the team. Some distractions also sometimes have a perceived positive impact, such as music, teaching and case-relevant communications.10
SUMMARY
A multitude of distractions present in the OR may impair attention, vigilance and SA. Some are inevitable, whereas others may be superfluous. Any distraction may be associated with negative outcomes. Several strategies are available to mitigate distractions and should be adopted, especially in critical situations that demand our undivided attention.
REFERENCES
- American Society of Anesthesiologists (ASA). Statement on distractions. Accessed October 15, 2023. https://www.asahq.org/ standards-and-practice-parameters/statement-on-distractions
- Esenther B, Ko R. Smartphones in the operating room: distraction or diagnostic aid? A case of newly diagnosed Wolff- Parkinson White in a pediatric patient having bronchoscopy under general anesthesia. A A Case Rep. 2015;5:40-42.
- Riutort Distractions in the operating room. Curr Anesthesiol Rep. 2020;10:456-462.
- Cohen TN, Shappell SA, Reeves ST, et Distracted doctoring: the role of personal electronic devices in the operating room. Periop Care Oper Room Manag. 2018;10:10-13.
- Slagle JM, Porterfield ES, Lorinc AN, et Prevalence of potentially distracting noncare activities and their effects on vigi- lance, workload, and nonroutine events during anesthesia care. Anesthesiology. 2018;128:44-54.
- van Pelt M, Weinger MB. Distractions in the anesthesia work environment: impact on patient safety? Report of a meeting sponsored by the Anesthesia Patient Safety Foundation. Anesth Analg. 2017;125:347-350.
- Antoniadis S, Passauer-Baierl S, Baschnegger H et al. Identification and interference of intraoperative distractions and interruptions in operating rooms. J Surg Res. 2014;188:21-29.
- McIlvaine WB. Situational awareness in the operating room: a primer for the anesthesiologist. Semin Anesth Periop Med Pain. 2007;26:167-172.
- Wheelock A, Suliman A, Wharton R, et al. The impact of operating room distractions on stress, workload, and Ann Surg. 2015;261:1079-1084.
- Nasri B-N, Mitchell JD, Jackson C, et Distractions in the operating room: a survey of the healthcare team. Surg Endosc. 2022;37:2316-2325.
- Domino KB, Sessler Internet use during anesthesia care. Anesthesiology. 2012;117:1156-1158.
- Schulz CM, Burden A, Posner KL, et Frequency and type of situational awareness errors contributing to death and brain damage. Anesthesiology. 2017;127:326-337.
- Crockett CJ, Donahue BS, Vandivier Distraction-free induction zone: a quality improvement initiative at a large academic children’s hospital to improve the quality and safety of anesthetic care for our patients. Anesth Analg. 2019;129:794-803.
- Moshe C, Roscher CR, Porter Hold the phone! Perioperative personal electronic devices. Curr Anesthesiol Rep. 2022;12:476-483.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/